| Glycated hemoglobin | |
|---|---|
| MedlinePlus | 003640 |
| eMedicine | 2049478 |
| LOINC | 41995-2 |
Glycated hemoglobin, also known as HbA1c, glycohemoglobin, hemoglobin A1c, A1C, is a form of hemoglobin (Hb) that is chemically linked to a sugar. Most monosaccharides, including glucose, galactose and fructose, spontaneously (i.e. non-enzymatically) bond with hemoglobin when present in the bloodstream. However, glucose is less likely to do so than galactose and fructose (13% that of fructose and 21% that of galactose), which may explain why glucose is used as the primary metabolic fuel in humans.[1][2]
The formation of the sugar-hemoglobin linkage indicates the presence of excessive sugar in the bloodstream, often indicative of diabetes in high concentration (HbA1c >6.4%).[3] A1C is of particular interest because it is easy to detect. The process by which sugars attach to hemoglobin is called glycation and the reference system is based on HbA1c, defined as beta-N-1-deoxy fructosyl haemoglobin as component.[4]
HbA1c is measured primarily to determine the three-month average blood sugar level and can be used as a diagnostic test for diabetes mellitus and as an assessment test for glycemic control in people with diabetes.[5] The test is limited to a three-month average because the average lifespan of a red blood cell is four months. Since individual red blood cells have varying lifespans, the test is used as a limited measure of three months. Normal levels of glucose produce a normal amount of glycated hemoglobin. As the average amount of plasma glucose increases, the fraction of glycated hemoglobin increases in a predictable way. In diabetes, higher amounts of glycated hemoglobin, indicating poorer control of blood glucose levels, have been associated with cardiovascular disease, nephropathy, neuropathy, and retinopathy.
Terminology[edit]
Glycated hemoglobin is preferred over glycosylated hemoglobin to reflect the correct (non-enzymatic) process. Early literature often used glycosylated as it was unclear which process was involved until further research was performed. The terms are still sometimes used interchangeably in English-language literature.[6]
The naming of HbA1c derives from hemoglobin type A being separated on cation exchange chromatography. The first fraction to separate, probably considered to be pure hemoglobin A, was designated HbA0, and the following fractions were designated HbA1a, HbA1b, and HbA1c, in their order of elution. Improved separation techniques have subsequently led to the isolation of more subfractions.[7]
History[edit]
Hemoglobin A1c was first separated from other forms of hemoglobin by Huisman and Meyering in 1958 using a chromatographic column.[8] It was first characterized as a glycoprotein by Bookchin and Gallop in 1968.[9] Its increase in diabetes was first described in 1969 by Samuel Rahbar et al.[10] The reactions leading to its formation were characterized by Bunn and his coworkers in 1975.[11]
The use of hemoglobin A1c for monitoring the degree of control of glucose metabolism in diabetic patients was proposed in 1976 by Anthony Cerami, Ronald Koenig and coworkers.[12]
Damage mechanisms[edit]
Glycated hemoglobin causes an increase of highly reactive free radicals inside blood cells, altering the properties of their cell membranes. This leads to blood cell aggregation and increased blood viscosity, which results in impaired blood flow.[13]
Another way glycated hemoglobin causes damage is via inflammation, which results in atherosclerotic plaque (atheroma) formation. Free-radical build-up promotes the excitation of Fe2+-hemoglobin through Fe3+-Hb into abnormal ferryl hemoglobin (Fe4+-Hb). Fe4+ is unstable and reacts with specific amino acids in hemoglobin to regain its Fe3+ oxidation state. Hemoglobin molecules clump together via cross-linking reactions, and these hemoglobin clumps (multimers) promote cell damage and the release of Fe4+-hemoglobin into the matrix of innermost layers (subendothelium) of arteries and veins. This results in increased permeability of interior surface (endothelium) of blood vessels and production of pro-inflammatory monocyte adhesion proteins, which promote macrophage accumulation in blood vessel surfaces, ultimately leading to harmful plaques in these vessels.[13]
Highly glycated Hb-AGEs go through vascular smooth muscle layer and inactivate acetylcholine-induced endothelium-dependent relaxation, possibly through binding to nitric oxide (NO), preventing its normal function. NO is a potent vasodilator and also inhibits formation of plaque-promoting LDLs (i.e. “bad cholesterol”) oxidized form.[13]
This overall degradation of blood cells also releases heme from them. Loose heme can cause oxidation of endothelial and LDL proteins, which results in plaques.[13]
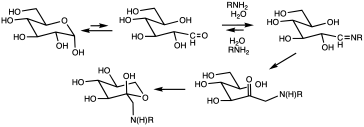
Glycation pathway via Amadori rearrangement (in HbA1c, R is typically N-terminal valine).[14]
Principle in medical diagnostics[edit]
Glycation of proteins is a frequent occurrence, but in the case of hemoglobin, a nonenzymatic condensation reaction occurs between glucose and the N-end of the beta chain. This reaction produces a Schiff base (R-N=CHR’, R = beta chain, CHR’= glucose-derived), which is itself converted to 1-deoxyfructose. This second conversion is an example of an Amadori rearrangement.
When blood glucose levels are high, glucose molecules attach to the hemoglobin in red blood cells. The longer hyperglycemia occurs in blood, the more glucose binds to hemoglobin in the red blood cells and the higher the glycated hemoglobin.[citation needed]
Once a hemoglobin molecule is glycated, it remains that way. A buildup of glycated hemoglobin within the red cell, therefore, reflects the average level of glucose to which the cell has been exposed during its life-cycle. Measuring glycated hemoglobin assesses the effectiveness of therapy by monitoring long-term serum glucose regulation.
A1c is a weighted average of blood glucose levels during the life of the red blood cells (117 days for men and 106 days in women[15]). Therefore, glucose levels on days nearer to the test contribute substantially more to the level of A1c than the levels in days further from the test.[16]
This is also supported by data from clinical practice showing that HbA1c levels improved significantly after 20 days from start or intensification of glucose-lowering treatment.[17]
Measurement[edit]
Several techniques are used to measure hemoglobin A1c. Laboratories may use high-performance liquid chromatography, immunoassay, enzymatic assay, capillary electrophoresis, or boronate affinity chromatography. Point of care (e.g., doctor’s office) devices use immunoassay boronate affinity chromatography.[citation needed]
In the United States, HbA1c testing laboratories are certified by the National Glycohemoglobin Standardization Program to standardize them against the results of the 1993 Diabetes Control and Complications Trial (DCCT).[18] An additional percentage scale, Mono S has previously been in use by Sweden and KO500 is in use in Japan.[19][20]
Switch to IFCC units[edit]
The American Diabetes Association, European Association for the Study of Diabetes, and International Diabetes Federation have agreed that, in the future, HbA1c is to be reported in the International Federation of Clinical Chemistry and Laboratory Medicine (IFCC) units.[21] IFCC reporting was introduced in Europe except for the UK in 2003;[22] the UK carried out dual reporting from 1 June 2009 [23] until 1 October 2011.
Conversion between DCCT and IFCC is by the following equation:[24]
![{displaystyle mathrm {IFCC} ,mathrm {HBA1c} ,{frac {text{mmol}}{text{mol}}}=[mathrm {DCCT} ,mathrm {HBA1c} ,(%)-2.14]times 10.929}](https://wikimedia.org/api/rest_v1/media/math/render/svg/83bb46eea683065c6ccf6362628534f60f3c0aa8)
| IFCC-HbA1c | DCCT-HbA1c | Mono S- HbA1c[20] |
|---|---|---|
| (mmol/mol) | (%) | (%) |
| 10 | 3.1 | 2.0 |
| 20 | 4.0 | 2.9 |
| 30 | 4.9 | 3.9 |
| 40 | 5.8 | 4.8 |
| 45 | 6.3 | 5.3 |
| 50 | 6.7 | 5.8 |
| 55 | 7.2 | 6.3 |
| 60 | 7.6 | 6.8 |
| 65 | 8.1 | 7.2 |
| 70 | 8.6 | 7.7 |
| 80 | 9.5 | 8.7 |
| 90 | 10.4 | 9.6 |
| 100 | 11.3 | 10.6 |
Interpretation of results[edit]
Laboratory results may differ depending on the analytical technique, the age of the subject, and biological variation among individuals. Higher levels of HbA1c are found in people with persistently elevated blood sugar, as in diabetes mellitus. While diabetic patient treatment goals vary, many include a target range of HbA1c values. A diabetic person with good glucose control has an HbA1c level that is close to or within the reference range.[citation needed]
The International Diabetes Federation and the American College of Endocrinology recommend HbA1c values below 48 mmol/mol (6.5 DCCT %), while the American Diabetes Association recommends HbA1c be below 53 mmol/mol (7.0 DCCT %) for most patients.[25] Results from large trials in 2008–09 suggested that a target below 53 mmol/mol (7 DCCT %) for older adults with type 2 diabetes may be excessive: Below 53 mmol/mol, the health benefits of reduced A1c become smaller, and the intensive glycemic control required to reach this level leads to an increased rate of dangerous hypoglycemic episodes.[26]
A retrospective study of 47,970 type 2 diabetes patients, aged 50 years and older, found that patients with an HbA1c more than 48 mmol/mol (6.5 DCCT %) had an increased mortality rate,[27] but a later international study contradicted these findings.[28][29][30]
A review of the UKPDS, Action to Control Cardiovascular Risk in Diabetes (ACCORD), Advance and Veterans Affairs Diabetes Trials (VADT) estimated that the risks of the main complications of diabetes (diabetic retinopathy, diabetic nephropathy, diabetic neuropathy, and macrovascular disease) decreased by about 3% for every 1 mmol/mol decrease in HbA1c.[31]
However, a trial by ACCORD designed specifically to determine whether reducing HbA1c below 6.0% using increased amounts of medication would reduce the rate of cardiovascular events found higher mortality with this intensive therapy, so much so that the trial was terminated 17 months early.[32]
Practitioners must consider patients’ health, their risk of hypoglycemia, and their specific health risks when setting a target HbA1c level. Because patients are responsible for averting or responding to their own hypoglycemic episodes, their input and the doctors’ assessments of the patients’ self-care skills are also important.
Persistent elevations in blood sugar (and, therefore, HbA1c) increase the risk of long-term vascular complications of diabetes, such as coronary disease, heart attack, stroke, heart failure, kidney failure, blindness, erectile dysfunction, neuropathy (loss of sensation, especially in the feet), gangrene, and gastroparesis (slowed emptying of the stomach). Poor blood glucose control also increases the risk of short-term complications of surgery such as poor wound healing.
Lower-than-expected levels of HbA1c can be seen in people with shortened red blood cell lifespans, such as with glucose-6-phosphate dehydrogenase deficiency, sickle-cell disease, or any other condition causing premature red blood cell death. Blood donation will result in rapid replacement of lost RBCs with newly formed red blood cells. Since these new RBCs will have only existed for a short period of time, their presence will lead HbA1c to underestimate the actual average levels. There may also be distortions resulting from blood donation during the preceding two months, due to an abnormal synchronization of the age of the RBCs, resulting in an older than normal average blood cell life (resulting in an overestimate of actual average blood glucose levels). Conversely, higher-than-expected levels can be seen in people with a longer red blood cell lifespan, such as with iron deficiency.[33]
Results can be unreliable in many circumstances, for example after blood loss, after surgery, blood transfusions, anemia, or high erythrocyte turnover; in the presence of chronic renal or liver disease; after administration of high-dose vitamin C; or erythropoetin treatment.[34] In general, the reference range (that found in healthy young persons), is about 30–33 mmol/mol (4.9–5.2 DCCT %).[35] The mean HbA1c for diabetics type 1 in Sweden in 2014 was 63 mmol/mol (7.9 DCCT%) and for type 2, 61 mmol/mol (7.7 DCCT%).[36]
The approximate mapping between HbA1c values given in DCCT percentage (%) and eAG (estimated average glucose) measurements is given by the following equation:[34]
- eAG(mg/dL) = 28.7 × A1C − 46.7
eAG(mmol/L) = 1.59 × A1C − 2.59
Data in parentheses are 95% confidence intervals
| HbA1c | eAG | ||
|---|---|---|---|
| % | mmol/mol[37] | mmol/L | mg/dL |
| 5 | 31 | 5.4 (4.2–6.7) | 97 (76–120) |
| 6 | 42 | 7.0 (5.5–8.5) | 126 (100–152) |
| 7 | 53 | 8.6 (6.8–10.3) | 154 (123–185) |
| 8 | 64 | 10.2 (8.1–12.1) | 183 (147–217) |
| 9 | 75 | 11.8 (9.4–13.9) | 212 (170–249) |
| 10 | 86 | 13.4 (10.7–15.7) | 240 (193–282) |
| 11 | 97 | 14.9 (12.0–17.5) | 269 (217–314) |
| 12 | 108 | 16.5 (13.3–19.3) | 298 (240–347) |
| 13 | 119 | 18.1 (15–21) | 326 (260–380) |
| 14 | 130 | 19.7 (16–23) | 355 (290–410) |
| 15 | 140 | 21.3 (17–25) | 384 (310–440) |
| 16 | 151 | 22.9 (19–26) | 413 (330–480) |
| 17 | 162 | 24.5 (20–28) | 441 (460–510) |
| 18 | 173 | 26.1 (21–30) | 470 (380–540) |
| 19 | 184 | 27.7 (23–32) | 499 (410–570) |
Normal, prediabetic, and diabetic range[edit]
The 2010 American Diabetes Association Standards of Medical Care in Diabetes added the =HbA1c ≥ 48 mmol/mol (≥6.5 DCCT %) as another criterion for the diagnosis of diabetes.[38]
| HbA1C | Diagnosis |
|---|---|
| <5.7% | Normal |
| 5.7–6.4% | Prediabetes |
| >6.4% | Diabetes |
Indications and uses[edit]
Glycated hemoglobin testing is recommended for both checking the blood sugar control in people who might be prediabetic and monitoring blood sugar control in patients with more elevated levels, termed diabetes mellitus. For a single blood sample, it provides far more revealing information on glycemic behavior than a fasting blood sugar value. However, fasting blood sugar tests are crucial in making treatment decisions. The American Diabetes Association guidelines are similar to others in advising that the glycated hemoglobin test be performed at least twice a year in patients with diabetes who are meeting treatment goals (and who have stable glycemic control) and quarterly in patients with diabetes whose therapy has changed or who are not meeting glycemic goals.[40]
Glycated hemoglobin measurement is not appropriate where a change in diet or treatment has been made within six weeks. Likewise, the test assumes a normal red blood cell aging process and mix of hemoglobin subtypes (predominantly HbA in normal adults). Hence, people with recent blood loss, hemolytic anemia, or genetic differences in the hemoglobin molecule (hemoglobinopathy) such as sickle-cell disease and other conditions, as well as those who have donated blood recently, are not suitable for this test.[citation needed]
Due to glycated hemoglobin’s variability (as shown in the table above), additional measures should be checked in patients at or near recommended goals. People with HbA1c values at 64 mmol/mol or less should be provided additional testing to determine whether the HbA1c values are due to averaging out high blood glucose (hyperglycemia) with low blood glucose (hypoglycemia) or the HbA1c is more reflective of an elevated blood glucose that does not vary much throughout the day. Devices such as continuous blood glucose monitoring allow people with diabetes to determine their blood glucose levels on a continuous basis, testing every few minutes. Continuous use of blood glucose monitors is becoming more common, and the devices are covered by many health insurance plans, but not by Medicare in the United States. The supplies tend to be expensive, since the sensors must be changed at least every 2 weeks. Another useful test in determining if HbA1c values are due to wide variations of blood glucose throughout the day is 1,5-anhydroglucitol, also known as GlycoMark. GlycoMark reflects only the times that the person experiences hyperglycemia above 180 mg/dL over a two-week period.[citation needed]
Concentrations of hemoglobin A1 (HbA1) are increased, both in diabetic patients and in patients with kidney failure, when measured by ion-exchange chromatography. The thiobarbituric acid method (a chemical method specific for the detection of glycation) shows that patients with kidney failure have values for glycated hemoglobin similar to those observed in normal subjects, suggesting that the high values in these patients are a result of binding of something other than glucose to hemoglobin.[41]
In autoimmune hemolytic anemia, concentrations of HbA1 is undetectable. Administration of prednisolone will allow the HbA1 to be detected.[42] The alternative fructosamine test may be used in these circumstances and it also reflects an average of blood glucose levels over the preceding 2 to 3 weeks.
All the major institutions such as the International Expert Committee Report, drawn from the International Diabetes Federation, the European Association for the Study of Diabetes, and the American Diabetes Association, suggest the HbA1c level of 48 mmol/mol (6.5 DCCT %) as a diagnostic level.[43] The Committee Report further states that, when HbA1c testing cannot be done, the fasting and glucose-tolerance tests be done. Diagnosis of diabetes during pregnancy continues to require fasting and glucose-tolerance measurements for gestational diabetes, and not the glycated hemoglobin.[citation needed]
Modification by diet[edit]
Meta-analysis has shown probiotics to cause a statistically significant reduction in glycated hemoglobin in type 2 diabetics.[44] Trials with multiple strains of probiotics had statistically significant reductions in glycated hemoglobin, whereas trials with single strains did not.[44]
Standardization and traceability[edit]
Hemoglobin A1c is now standardized and traceable to IFCC methods HPLC-CE and HPLC-MS. The change to the newer unit of mmol/mol is part of this standardization. The standardized test does not test for iodine levels in the blood; hypothyroidism or iodine supplementation are known to artificially raise the A1c.[45][unreliable medical source?]
[46]
Veterinary medicine[edit]
HbA1c testing has not been found useful in the treatment of cats and dogs with diabetes, and is not generally used; fructosamine is favoured instead.[47]
See also[edit]
- Diabetes mellitus
- Hemoglobin A2
- Prediabetes
- Proteopedia: Structure of glycated hemoglobin
References[edit]
- ^ Bunn HF, Higgins PJ (July 1981). «Reaction of monosaccharides with proteins: possible evolutionary significance». Science. 213 (4504): 222–224. Bibcode:1981Sci…213..222B. doi:10.1126/science.12192669. PMID 12192669.
- ^ McPherson JD, Shilton BH, Walton DJ (March 1988). «Role of fructose in glycation and cross-linking of proteins». Biochemistry. 27 (6): 1901–1907. doi:10.1021/bi00406a016. PMID 3132203.
- ^ Pongudom, Saranya (1 November 2019). «Determination of Normal HbA1C Levels in Non-Diabetic Patients with Hemoglobin E». Annals of Clinical & Laboratory Science. 49 (6): 804–809 – via PubMed.
- ^ Miedema K (2005). «Standardization of HbA1c and Optimal Range of Monitoring». Scandinavian Journal of Clinical and Laboratory Investigation. 240: 61–72. doi:10.1080/00365510500236143. PMID 16112961. S2CID 30162967.
- ^ Use of Glycated Haemoglobin (HbA1C) in the Diagnosis of Diabetes Mellitus: Abbreviated Report of a WHO Consultation. Geneva: World Health Organization. 2011. p. 2, Glycated haemoglobin (HbA1c) for the diagnosis of diabetes. Retrieved 2 December 2018.
- ^ Oliwia Witczak, Trine B. Haugen (25 November 2014). «Glycated or glycosylated?». Journal of the Norwegian Medical Association. 134 (22): 2179. doi:10.4045/tidsskr.14.0172. PMID 25423986. Retrieved 5 December 2018.
Hospitals should ensure that the correct term for HbA1c – glycated haemoglobin – is now to be found in laboratory manuals.
- ^ Peterson KP, Pavlovich JG, Goldstein D, Little R, England J, Peterson CM (1998). «What is hemoglobin A1c? An analysis of glycated hemoglobins by electrospray ionization mass spectrometry». Clinical Chemistry. 44 (9): 1951–1958. doi:10.1093/clinchem/44.9.1951. PMID 9732983.
- ^ Huisman TH, Martis EA, Dozy A (1958). «Chromatography of hemoglobin types on carboxymethylcellulose». J. Lab. Clin. Med. 52 (2): 312–327. PMID 13564011.
- ^ Bookchin RM, Gallop PM (1968). «Structure of haemoglobin A1c: nature of the N-terminal beta chain blocking group». Biochem. Biophys. Res. Commun. 32 (1): 86–93. doi:10.1016/0006-291X(68)90430-0. PMID 4874776.
- ^ Rahbar S, Blumenfeld O, Ranney HM (1969). «Studies of an unusual hemoglobin in patients with diabetes mellitus». Biochem. Biophys. Res. Commun. 36 (5): 838–843. doi:10.1016/0006-291X(69)90685-8. PMID 5808299.
- ^ Bunn HF, Haney DN, Gabbay KH, Gallop PM (1975). «Further identification of the nature and linkage of the carbohydrate in haemoglobin A1c». Biochem. Biophys. Res. Commun. 67 (1): 103–109. doi:10.1016/0006-291X(75)90289-2. PMID 1201013.
- ^ Koenig RJ, Peterson CM, Jones RL, Saudek C, Lehrman M, Cerami A (1976). «Correlation of glucose regulation and hemoglobin AIc in diabetes mellitus». N. Engl. J. Med. 295 (8): 417–420. doi:10.1056/NEJM197608192950804. PMID 934240.
- ^ a b c d Saleh, Jumana (2015-08-26). «Glycated hemoglobin and its spinoffs: Cardiovascular disease markers or risk factors?». World Journal of Cardiology. 7 (8): 449–453. doi:10.4330/wjc.v7.i8.449. ISSN 1949-8462. PMC 4549778. PMID 26322184.
- ^ Yaylayan, Varoujan A.; Huyghues-Despointes, Alexis (1994). «Chemistry of Amadori Rearrangement Products: Analysis, Synthesis, Kinetics, Reactions, and Spectroscopic Properties». Critical Reviews in Food Science and Nutrition. 34 (4): 321–369. doi:10.1080/10408399409527667. PMID 7945894.
- ^ Unnikrishnan, Ranjit (Jul–Aug 2012). «Drugs affecting HbA1c levels». Indian Journal of Endocrinology and Metabolism. 16 (4): 528–531. doi:10.4103/2230-8210.98004. PMC 3401751. PMID 22837911.
- ^ «NGSP: HbA1c and eAG». www.ngsp.org. Retrieved 2015-10-28.
- ^ Sidorenkov G, Haaijer-Ruskamp FM, de Zeeuw D, Denig P (2011). «A longitudinal study examining adherence to guidelines in diabetes care according to different definitions of adequacy and timeliness». PLOS ONE. 6 (9): e24278. Bibcode:2011PLoSO…624278S. doi:10.1371/journal.pone.0024278. PMC 3169586. PMID 21931669.
- ^ Developing Point of care HbA1c tests for Diabetes monitoring Archived 2008-08-29 at the Wayback Machine, Barry Plant, Originally Published IVDT July/August 2008
- ^ [Clinical Chemistry 50:1 166–174 (2004)]
- ^ a b HbA1c in a new way Archived 2022-07-13 at the Wayback Machine By the Swedish Diabetes Association. Retrieved Mars 2011
- ^ Geistanger A, Arends S, Berding C, Hoshino T, Jeppsson JO, Little R, Siebelder C, Weykamp C (August 2008). «Statistical methods for monitoring the relationship between the IFCC reference measurement procedure for hemoglobin A1c and the designated comparison methods in the United States, Japan, and Sweden». Clin. Chem. 54 (8): 1379–1385. doi:10.1373/clinchem.2008.103556. PMID 18539643.
- ^ Manley S, John WG, Marshall S (July 2004). «Introduction of IFCC reference method for calibration of HbA: implications for clinical care». Diabet. Med. 21 (7): 673–676. doi:10.1111/j.1464-5491.2004.01311.x. PMID 15209757. S2CID 30468208.
- ^ «Standardisation of the reference method for the measurement of HbA1c to improve diabetes care» (PDF). The Association for Clinical Biochemistry and Diabetss UK. April 2008. Archived from the original (PDF) on 2011-07-22. Retrieved 2009-07-02.
- ^ «HbA1c Standardisation For Laboratory Professionals» (PDF). Diabetes UK. Archived from the original (PDF) on 2011-07-20. Retrieved 2009-07-02.
- ^ «Executive Summary: Standards of medical care in diabetes – 2009». Diabetes Care. 32: S6–S12. 2009. doi:10.2337/dc09-S006. PMC 2613586. PMID 19118288.
- ^ Lehman R, Krumholz HM (2009). «Tight control of blood glucose in long standing type 2 diabetes». Br Med J. 338: b800. doi:10.1136/bmj.b800. PMID 19264821. S2CID 45188963.
- ^ Currie, Craig J; Peters, John R; Tynan, Aodán; Evans, Marc; Heine, Robert J; Bracco, Oswaldo L; Zagar, Tony; Poole, Chris D (2010). «Survival as a function of HbA1c in people with type 2 diabetes: a retrospective cohort study». The Lancet. 375 (9713): 481–489. doi:10.1016/S0140-6736(09)61969-3. PMID 20110121. S2CID 21223855.
- ^ «Advance Study Contradicts ACCORD Findings». Diabetes Self-Management. 2008-03-07. Retrieved 2013-06-10.
- ^ «The largest ever study of diabetes shows intensive glucose control reduces serious complications». Advance-trial.com. Archived from the original on 2013-01-16. Retrieved 2013-06-10.
- ^ Heller, Simon R. (2009-11-01). «A Summary of the Advance Trial». Diabetes Care. 32 (Suppl 2): S357–S361. doi:10.2337/dc09-S339. ISSN 0149-5992. PMC 2811451. PMID 19875581.
- ^ Shubrook JH, Shubrook J (2010). «Risks and benefits of attaining HbA(1c) goals: Examining the evidence». The Journal of the American Osteopathic Association. 110 (7 Suppl 7): e7–e12. PMID 20644204.
- ^ Gerstein HC, Miller ME, Byington RP, et al. (2008). «Effects of Intensive Glucose Lowering in Type 2 Diabetes». New England Journal of Medicine. 358 (24): 2545–2559. doi:10.1056/NEJMoa0802743. ISSN 0028-4793. PMC 4551392. PMID 18539917.
- ^ Kilpatrick ES, Bloomgarden ZT, Zimmet PZ (2009). «Is haemoglobin A1c a step forward for diagnosing diabetes?». BMJ. 339: b4432. doi:10.1136/bmj.b4432. PMID 19903702. S2CID 36941786.
- ^ a b Nathan DM, Kuenen J, Borg R, Zheng H, Schoenfeld D, Heine RJ (2008). «Translating the A1C assay into estimated average glucose values». Diabetes Care. 31 (8): 1473–1478. doi:10.2337/dc08-0545. PMC 2742903. PMID 18540046.
- ^ Saaddine, Jinan B.; Fagot-Campagna, Anne; Rolka, Deborah; Narayan, K. M. Venkat; Geiss, Linda; Eberhardt, Mark; Flegal, Katherine M. (2002-08-01). «Distribution of HbA(1c) levels for children and young adults in the U.S.: Third National Health and Nutrition Examination Survey». Diabetes Care. 25 (8): 1326–1330. doi:10.2337/diacare.25.8.1326. ISSN 0149-5992. PMID 12145229.
- ^ «Nationella Diabetesregistret Årsrapport 2014 års resultat» (PDF). Nationella Diabetesregistret Årsrapport 2014 års resultat (in Swedish). Nationella Diabetes Registret. Retrieved 2015-12-14.
- ^ Change to HbA1c values Archived 2014-03-01 at the Wayback Machine at Diabetes UK, 2013
- ^ «Executive summary: Standards of medical care in diabetes—2010». Diabetes Care. 33 (Suppl 1): S4–S10. January 2010. doi:10.2337/dc10-S004. PMC 2797389. PMID 20042774.
- ^ «Diagnosing Diabetes and Learning About Prediabetes». American Diabetes Association. Retrieved 2 December 2018.
- ^ American Diabetes Association (2007). «Standards of medical care in diabetes». Diabetes Care. 30 (Suppl 1): S4–S41. doi:10.2337/dc07-S004. PMID 17192377.
- ^ Dufresne, L.; Joly, J. G.; Lepage, R.; Lessard, F.; Bannon, P. (1984). «Glycated Hemoglobin in Uremic Patients as Measured by Affinity and Ion-Exchange Chromatography» (PDF). clinchem.com. pp. 485–486. doi:10.1093/clinchem/30.3.485. PMID 6697506. Retrieved 2009-08-31.
- ^ «Undetectable Glycosolated Hemoglobin in Autoimmune Hemolytic Anemia» (PDF). repository.oai.yamaguchi-u.ac.jp. Retrieved 2009-08-31.
- ^ The International Expert Committee (2009). «International expert committee report on the role of the A1C assay in the diagnosis of diabetes». Diabetes Care. 32 (7): 1327–1334. doi:10.2337/dc09-9033. PMC 2699715. PMID 19502545.
- ^ a b Sun J, Buys NJ (2016). «Glucose- and glycaemic factor-lowering effects of probiotics on diabetes: a meta-analysis of randomised placebo-controlled trials». British Journal of Nutrition. 115 (7): 1167–1177. doi:10.1017/S0007114516000076. PMID 26899960.
- ^ «Hypothyroidism Falsely Raises HbA1c and Glycated Albumin Levels». Diabetes In Control. 12 November 2010.
- ^ Kim, M. K.; Kwon, H. S.; Baek, K. H.; Lee, J. H.; Park, W. C.; Sohn, H. S.; Lee, K. W.; Song, K. H. (7 September 2010). «Effects of Thyroid Hormone on A1C and Glycated Albumin Levels in Nondiabetic Subjects With Overt Hypothyroidism». Diabetes Care. 33 (12): 2546–2548. doi:10.2337/dc10-0988. PMC 2992186. PMID 20823345.
- ^ Delack JB, Stogdale L (October 1983). «Glycosylated hemoglobin measurement in dogs and cats: implications for its utility in diabetic monitoring». Can Vet J. 24 (10): 308–311. PMC 1790442. PMID 17422317.
External links[edit]
- National Diabetes Information Clearinghouse Archived 2010-02-21 at the Wayback Machine
- American Diabetes Association Standards of Medical Care 2007
| Glycated hemoglobin | |
|---|---|
| MedlinePlus | 003640 |
| eMedicine | 2049478 |
| LOINC | 41995-2 |
Glycated hemoglobin, also known as HbA1c, glycohemoglobin, hemoglobin A1c, A1C, is a form of hemoglobin (Hb) that is chemically linked to a sugar. Most monosaccharides, including glucose, galactose and fructose, spontaneously (i.e. non-enzymatically) bond with hemoglobin when present in the bloodstream. However, glucose is less likely to do so than galactose and fructose (13% that of fructose and 21% that of galactose), which may explain why glucose is used as the primary metabolic fuel in humans.[1][2]
The formation of the sugar-hemoglobin linkage indicates the presence of excessive sugar in the bloodstream, often indicative of diabetes in high concentration (HbA1c >6.4%).[3] A1C is of particular interest because it is easy to detect. The process by which sugars attach to hemoglobin is called glycation and the reference system is based on HbA1c, defined as beta-N-1-deoxy fructosyl haemoglobin as component.[4]
HbA1c is measured primarily to determine the three-month average blood sugar level and can be used as a diagnostic test for diabetes mellitus and as an assessment test for glycemic control in people with diabetes.[5] The test is limited to a three-month average because the average lifespan of a red blood cell is four months. Since individual red blood cells have varying lifespans, the test is used as a limited measure of three months. Normal levels of glucose produce a normal amount of glycated hemoglobin. As the average amount of plasma glucose increases, the fraction of glycated hemoglobin increases in a predictable way. In diabetes, higher amounts of glycated hemoglobin, indicating poorer control of blood glucose levels, have been associated with cardiovascular disease, nephropathy, neuropathy, and retinopathy.
Terminology[edit]
Glycated hemoglobin is preferred over glycosylated hemoglobin to reflect the correct (non-enzymatic) process. Early literature often used glycosylated as it was unclear which process was involved until further research was performed. The terms are still sometimes used interchangeably in English-language literature.[6]
The naming of HbA1c derives from hemoglobin type A being separated on cation exchange chromatography. The first fraction to separate, probably considered to be pure hemoglobin A, was designated HbA0, and the following fractions were designated HbA1a, HbA1b, and HbA1c, in their order of elution. Improved separation techniques have subsequently led to the isolation of more subfractions.[7]
History[edit]
Hemoglobin A1c was first separated from other forms of hemoglobin by Huisman and Meyering in 1958 using a chromatographic column.[8] It was first characterized as a glycoprotein by Bookchin and Gallop in 1968.[9] Its increase in diabetes was first described in 1969 by Samuel Rahbar et al.[10] The reactions leading to its formation were characterized by Bunn and his coworkers in 1975.[11]
The use of hemoglobin A1c for monitoring the degree of control of glucose metabolism in diabetic patients was proposed in 1976 by Anthony Cerami, Ronald Koenig and coworkers.[12]
Damage mechanisms[edit]
Glycated hemoglobin causes an increase of highly reactive free radicals inside blood cells, altering the properties of their cell membranes. This leads to blood cell aggregation and increased blood viscosity, which results in impaired blood flow.[13]
Another way glycated hemoglobin causes damage is via inflammation, which results in atherosclerotic plaque (atheroma) formation. Free-radical build-up promotes the excitation of Fe2+-hemoglobin through Fe3+-Hb into abnormal ferryl hemoglobin (Fe4+-Hb). Fe4+ is unstable and reacts with specific amino acids in hemoglobin to regain its Fe3+ oxidation state. Hemoglobin molecules clump together via cross-linking reactions, and these hemoglobin clumps (multimers) promote cell damage and the release of Fe4+-hemoglobin into the matrix of innermost layers (subendothelium) of arteries and veins. This results in increased permeability of interior surface (endothelium) of blood vessels and production of pro-inflammatory monocyte adhesion proteins, which promote macrophage accumulation in blood vessel surfaces, ultimately leading to harmful plaques in these vessels.[13]
Highly glycated Hb-AGEs go through vascular smooth muscle layer and inactivate acetylcholine-induced endothelium-dependent relaxation, possibly through binding to nitric oxide (NO), preventing its normal function. NO is a potent vasodilator and also inhibits formation of plaque-promoting LDLs (i.e. “bad cholesterol”) oxidized form.[13]
This overall degradation of blood cells also releases heme from them. Loose heme can cause oxidation of endothelial and LDL proteins, which results in plaques.[13]
Glycation pathway via Amadori rearrangement (in HbA1c, R is typically N-terminal valine).[14]
Principle in medical diagnostics[edit]
Glycation of proteins is a frequent occurrence, but in the case of hemoglobin, a nonenzymatic condensation reaction occurs between glucose and the N-end of the beta chain. This reaction produces a Schiff base (R-N=CHR’, R = beta chain, CHR’= glucose-derived), which is itself converted to 1-deoxyfructose. This second conversion is an example of an Amadori rearrangement.
When blood glucose levels are high, glucose molecules attach to the hemoglobin in red blood cells. The longer hyperglycemia occurs in blood, the more glucose binds to hemoglobin in the red blood cells and the higher the glycated hemoglobin.[citation needed]
Once a hemoglobin molecule is glycated, it remains that way. A buildup of glycated hemoglobin within the red cell, therefore, reflects the average level of glucose to which the cell has been exposed during its life-cycle. Measuring glycated hemoglobin assesses the effectiveness of therapy by monitoring long-term serum glucose regulation.
A1c is a weighted average of blood glucose levels during the life of the red blood cells (117 days for men and 106 days in women[15]). Therefore, glucose levels on days nearer to the test contribute substantially more to the level of A1c than the levels in days further from the test.[16]
This is also supported by data from clinical practice showing that HbA1c levels improved significantly after 20 days from start or intensification of glucose-lowering treatment.[17]
Measurement[edit]
Several techniques are used to measure hemoglobin A1c. Laboratories may use high-performance liquid chromatography, immunoassay, enzymatic assay, capillary electrophoresis, or boronate affinity chromatography. Point of care (e.g., doctor’s office) devices use immunoassay boronate affinity chromatography.[citation needed]
In the United States, HbA1c testing laboratories are certified by the National Glycohemoglobin Standardization Program to standardize them against the results of the 1993 Diabetes Control and Complications Trial (DCCT).[18] An additional percentage scale, Mono S has previously been in use by Sweden and KO500 is in use in Japan.[19][20]
Switch to IFCC units[edit]
The American Diabetes Association, European Association for the Study of Diabetes, and International Diabetes Federation have agreed that, in the future, HbA1c is to be reported in the International Federation of Clinical Chemistry and Laboratory Medicine (IFCC) units.[21] IFCC reporting was introduced in Europe except for the UK in 2003;[22] the UK carried out dual reporting from 1 June 2009 [23] until 1 October 2011.
Conversion between DCCT and IFCC is by the following equation:[24]
| IFCC-HbA1c | DCCT-HbA1c | Mono S- HbA1c[20] |
|---|---|---|
| (mmol/mol) | (%) | (%) |
| 10 | 3.1 | 2.0 |
| 20 | 4.0 | 2.9 |
| 30 | 4.9 | 3.9 |
| 40 | 5.8 | 4.8 |
| 45 | 6.3 | 5.3 |
| 50 | 6.7 | 5.8 |
| 55 | 7.2 | 6.3 |
| 60 | 7.6 | 6.8 |
| 65 | 8.1 | 7.2 |
| 70 | 8.6 | 7.7 |
| 80 | 9.5 | 8.7 |
| 90 | 10.4 | 9.6 |
| 100 | 11.3 | 10.6 |
Interpretation of results[edit]
Laboratory results may differ depending on the analytical technique, the age of the subject, and biological variation among individuals. Higher levels of HbA1c are found in people with persistently elevated blood sugar, as in diabetes mellitus. While diabetic patient treatment goals vary, many include a target range of HbA1c values. A diabetic person with good glucose control has an HbA1c level that is close to or within the reference range.[citation needed]
The International Diabetes Federation and the American College of Endocrinology recommend HbA1c values below 48 mmol/mol (6.5 DCCT %), while the American Diabetes Association recommends HbA1c be below 53 mmol/mol (7.0 DCCT %) for most patients.[25] Results from large trials in 2008–09 suggested that a target below 53 mmol/mol (7 DCCT %) for older adults with type 2 diabetes may be excessive: Below 53 mmol/mol, the health benefits of reduced A1c become smaller, and the intensive glycemic control required to reach this level leads to an increased rate of dangerous hypoglycemic episodes.[26]
A retrospective study of 47,970 type 2 diabetes patients, aged 50 years and older, found that patients with an HbA1c more than 48 mmol/mol (6.5 DCCT %) had an increased mortality rate,[27] but a later international study contradicted these findings.[28][29][30]
A review of the UKPDS, Action to Control Cardiovascular Risk in Diabetes (ACCORD), Advance and Veterans Affairs Diabetes Trials (VADT) estimated that the risks of the main complications of diabetes (diabetic retinopathy, diabetic nephropathy, diabetic neuropathy, and macrovascular disease) decreased by about 3% for every 1 mmol/mol decrease in HbA1c.[31]
However, a trial by ACCORD designed specifically to determine whether reducing HbA1c below 6.0% using increased amounts of medication would reduce the rate of cardiovascular events found higher mortality with this intensive therapy, so much so that the trial was terminated 17 months early.[32]
Practitioners must consider patients’ health, their risk of hypoglycemia, and their specific health risks when setting a target HbA1c level. Because patients are responsible for averting or responding to their own hypoglycemic episodes, their input and the doctors’ assessments of the patients’ self-care skills are also important.
Persistent elevations in blood sugar (and, therefore, HbA1c) increase the risk of long-term vascular complications of diabetes, such as coronary disease, heart attack, stroke, heart failure, kidney failure, blindness, erectile dysfunction, neuropathy (loss of sensation, especially in the feet), gangrene, and gastroparesis (slowed emptying of the stomach). Poor blood glucose control also increases the risk of short-term complications of surgery such as poor wound healing.
Lower-than-expected levels of HbA1c can be seen in people with shortened red blood cell lifespans, such as with glucose-6-phosphate dehydrogenase deficiency, sickle-cell disease, or any other condition causing premature red blood cell death. Blood donation will result in rapid replacement of lost RBCs with newly formed red blood cells. Since these new RBCs will have only existed for a short period of time, their presence will lead HbA1c to underestimate the actual average levels. There may also be distortions resulting from blood donation during the preceding two months, due to an abnormal synchronization of the age of the RBCs, resulting in an older than normal average blood cell life (resulting in an overestimate of actual average blood glucose levels). Conversely, higher-than-expected levels can be seen in people with a longer red blood cell lifespan, such as with iron deficiency.[33]
Results can be unreliable in many circumstances, for example after blood loss, after surgery, blood transfusions, anemia, or high erythrocyte turnover; in the presence of chronic renal or liver disease; after administration of high-dose vitamin C; or erythropoetin treatment.[34] In general, the reference range (that found in healthy young persons), is about 30–33 mmol/mol (4.9–5.2 DCCT %).[35] The mean HbA1c for diabetics type 1 in Sweden in 2014 was 63 mmol/mol (7.9 DCCT%) and for type 2, 61 mmol/mol (7.7 DCCT%).[36]
The approximate mapping between HbA1c values given in DCCT percentage (%) and eAG (estimated average glucose) measurements is given by the following equation:[34]
- eAG(mg/dL) = 28.7 × A1C − 46.7
eAG(mmol/L) = 1.59 × A1C − 2.59
Data in parentheses are 95% confidence intervals
| HbA1c | eAG | ||
|---|---|---|---|
| % | mmol/mol[37] | mmol/L | mg/dL |
| 5 | 31 | 5.4 (4.2–6.7) | 97 (76–120) |
| 6 | 42 | 7.0 (5.5–8.5) | 126 (100–152) |
| 7 | 53 | 8.6 (6.8–10.3) | 154 (123–185) |
| 8 | 64 | 10.2 (8.1–12.1) | 183 (147–217) |
| 9 | 75 | 11.8 (9.4–13.9) | 212 (170–249) |
| 10 | 86 | 13.4 (10.7–15.7) | 240 (193–282) |
| 11 | 97 | 14.9 (12.0–17.5) | 269 (217–314) |
| 12 | 108 | 16.5 (13.3–19.3) | 298 (240–347) |
| 13 | 119 | 18.1 (15–21) | 326 (260–380) |
| 14 | 130 | 19.7 (16–23) | 355 (290–410) |
| 15 | 140 | 21.3 (17–25) | 384 (310–440) |
| 16 | 151 | 22.9 (19–26) | 413 (330–480) |
| 17 | 162 | 24.5 (20–28) | 441 (460–510) |
| 18 | 173 | 26.1 (21–30) | 470 (380–540) |
| 19 | 184 | 27.7 (23–32) | 499 (410–570) |
Normal, prediabetic, and diabetic range[edit]
The 2010 American Diabetes Association Standards of Medical Care in Diabetes added the =HbA1c ≥ 48 mmol/mol (≥6.5 DCCT %) as another criterion for the diagnosis of diabetes.[38]
| HbA1C | Diagnosis |
|---|---|
| <5.7% | Normal |
| 5.7–6.4% | Prediabetes |
| >6.4% | Diabetes |
Indications and uses[edit]
Glycated hemoglobin testing is recommended for both checking the blood sugar control in people who might be prediabetic and monitoring blood sugar control in patients with more elevated levels, termed diabetes mellitus. For a single blood sample, it provides far more revealing information on glycemic behavior than a fasting blood sugar value. However, fasting blood sugar tests are crucial in making treatment decisions. The American Diabetes Association guidelines are similar to others in advising that the glycated hemoglobin test be performed at least twice a year in patients with diabetes who are meeting treatment goals (and who have stable glycemic control) and quarterly in patients with diabetes whose therapy has changed or who are not meeting glycemic goals.[40]
Glycated hemoglobin measurement is not appropriate where a change in diet or treatment has been made within six weeks. Likewise, the test assumes a normal red blood cell aging process and mix of hemoglobin subtypes (predominantly HbA in normal adults). Hence, people with recent blood loss, hemolytic anemia, or genetic differences in the hemoglobin molecule (hemoglobinopathy) such as sickle-cell disease and other conditions, as well as those who have donated blood recently, are not suitable for this test.[citation needed]
Due to glycated hemoglobin’s variability (as shown in the table above), additional measures should be checked in patients at or near recommended goals. People with HbA1c values at 64 mmol/mol or less should be provided additional testing to determine whether the HbA1c values are due to averaging out high blood glucose (hyperglycemia) with low blood glucose (hypoglycemia) or the HbA1c is more reflective of an elevated blood glucose that does not vary much throughout the day. Devices such as continuous blood glucose monitoring allow people with diabetes to determine their blood glucose levels on a continuous basis, testing every few minutes. Continuous use of blood glucose monitors is becoming more common, and the devices are covered by many health insurance plans, but not by Medicare in the United States. The supplies tend to be expensive, since the sensors must be changed at least every 2 weeks. Another useful test in determining if HbA1c values are due to wide variations of blood glucose throughout the day is 1,5-anhydroglucitol, also known as GlycoMark. GlycoMark reflects only the times that the person experiences hyperglycemia above 180 mg/dL over a two-week period.[citation needed]
Concentrations of hemoglobin A1 (HbA1) are increased, both in diabetic patients and in patients with kidney failure, when measured by ion-exchange chromatography. The thiobarbituric acid method (a chemical method specific for the detection of glycation) shows that patients with kidney failure have values for glycated hemoglobin similar to those observed in normal subjects, suggesting that the high values in these patients are a result of binding of something other than glucose to hemoglobin.[41]
In autoimmune hemolytic anemia, concentrations of HbA1 is undetectable. Administration of prednisolone will allow the HbA1 to be detected.[42] The alternative fructosamine test may be used in these circumstances and it also reflects an average of blood glucose levels over the preceding 2 to 3 weeks.
All the major institutions such as the International Expert Committee Report, drawn from the International Diabetes Federation, the European Association for the Study of Diabetes, and the American Diabetes Association, suggest the HbA1c level of 48 mmol/mol (6.5 DCCT %) as a diagnostic level.[43] The Committee Report further states that, when HbA1c testing cannot be done, the fasting and glucose-tolerance tests be done. Diagnosis of diabetes during pregnancy continues to require fasting and glucose-tolerance measurements for gestational diabetes, and not the glycated hemoglobin.[citation needed]
Modification by diet[edit]
Meta-analysis has shown probiotics to cause a statistically significant reduction in glycated hemoglobin in type 2 diabetics.[44] Trials with multiple strains of probiotics had statistically significant reductions in glycated hemoglobin, whereas trials with single strains did not.[44]
Standardization and traceability[edit]
Hemoglobin A1c is now standardized and traceable to IFCC methods HPLC-CE and HPLC-MS. The change to the newer unit of mmol/mol is part of this standardization. The standardized test does not test for iodine levels in the blood; hypothyroidism or iodine supplementation are known to artificially raise the A1c.[45][unreliable medical source?]
[46]
Veterinary medicine[edit]
HbA1c testing has not been found useful in the treatment of cats and dogs with diabetes, and is not generally used; fructosamine is favoured instead.[47]
See also[edit]
- Diabetes mellitus
- Hemoglobin A2
- Prediabetes
- Proteopedia: Structure of glycated hemoglobin
References[edit]
- ^ Bunn HF, Higgins PJ (July 1981). «Reaction of monosaccharides with proteins: possible evolutionary significance». Science. 213 (4504): 222–224. Bibcode:1981Sci…213..222B. doi:10.1126/science.12192669. PMID 12192669.
- ^ McPherson JD, Shilton BH, Walton DJ (March 1988). «Role of fructose in glycation and cross-linking of proteins». Biochemistry. 27 (6): 1901–1907. doi:10.1021/bi00406a016. PMID 3132203.
- ^ Pongudom, Saranya (1 November 2019). «Determination of Normal HbA1C Levels in Non-Diabetic Patients with Hemoglobin E». Annals of Clinical & Laboratory Science. 49 (6): 804–809 – via PubMed.
- ^ Miedema K (2005). «Standardization of HbA1c and Optimal Range of Monitoring». Scandinavian Journal of Clinical and Laboratory Investigation. 240: 61–72. doi:10.1080/00365510500236143. PMID 16112961. S2CID 30162967.
- ^ Use of Glycated Haemoglobin (HbA1C) in the Diagnosis of Diabetes Mellitus: Abbreviated Report of a WHO Consultation. Geneva: World Health Organization. 2011. p. 2, Glycated haemoglobin (HbA1c) for the diagnosis of diabetes. Retrieved 2 December 2018.
- ^ Oliwia Witczak, Trine B. Haugen (25 November 2014). «Glycated or glycosylated?». Journal of the Norwegian Medical Association. 134 (22): 2179. doi:10.4045/tidsskr.14.0172. PMID 25423986. Retrieved 5 December 2018.
Hospitals should ensure that the correct term for HbA1c – glycated haemoglobin – is now to be found in laboratory manuals.
- ^ Peterson KP, Pavlovich JG, Goldstein D, Little R, England J, Peterson CM (1998). «What is hemoglobin A1c? An analysis of glycated hemoglobins by electrospray ionization mass spectrometry». Clinical Chemistry. 44 (9): 1951–1958. doi:10.1093/clinchem/44.9.1951. PMID 9732983.
- ^ Huisman TH, Martis EA, Dozy A (1958). «Chromatography of hemoglobin types on carboxymethylcellulose». J. Lab. Clin. Med. 52 (2): 312–327. PMID 13564011.
- ^ Bookchin RM, Gallop PM (1968). «Structure of haemoglobin A1c: nature of the N-terminal beta chain blocking group». Biochem. Biophys. Res. Commun. 32 (1): 86–93. doi:10.1016/0006-291X(68)90430-0. PMID 4874776.
- ^ Rahbar S, Blumenfeld O, Ranney HM (1969). «Studies of an unusual hemoglobin in patients with diabetes mellitus». Biochem. Biophys. Res. Commun. 36 (5): 838–843. doi:10.1016/0006-291X(69)90685-8. PMID 5808299.
- ^ Bunn HF, Haney DN, Gabbay KH, Gallop PM (1975). «Further identification of the nature and linkage of the carbohydrate in haemoglobin A1c». Biochem. Biophys. Res. Commun. 67 (1): 103–109. doi:10.1016/0006-291X(75)90289-2. PMID 1201013.
- ^ Koenig RJ, Peterson CM, Jones RL, Saudek C, Lehrman M, Cerami A (1976). «Correlation of glucose regulation and hemoglobin AIc in diabetes mellitus». N. Engl. J. Med. 295 (8): 417–420. doi:10.1056/NEJM197608192950804. PMID 934240.
- ^ a b c d Saleh, Jumana (2015-08-26). «Glycated hemoglobin and its spinoffs: Cardiovascular disease markers or risk factors?». World Journal of Cardiology. 7 (8): 449–453. doi:10.4330/wjc.v7.i8.449. ISSN 1949-8462. PMC 4549778. PMID 26322184.
- ^ Yaylayan, Varoujan A.; Huyghues-Despointes, Alexis (1994). «Chemistry of Amadori Rearrangement Products: Analysis, Synthesis, Kinetics, Reactions, and Spectroscopic Properties». Critical Reviews in Food Science and Nutrition. 34 (4): 321–369. doi:10.1080/10408399409527667. PMID 7945894.
- ^ Unnikrishnan, Ranjit (Jul–Aug 2012). «Drugs affecting HbA1c levels». Indian Journal of Endocrinology and Metabolism. 16 (4): 528–531. doi:10.4103/2230-8210.98004. PMC 3401751. PMID 22837911.
- ^ «NGSP: HbA1c and eAG». www.ngsp.org. Retrieved 2015-10-28.
- ^ Sidorenkov G, Haaijer-Ruskamp FM, de Zeeuw D, Denig P (2011). «A longitudinal study examining adherence to guidelines in diabetes care according to different definitions of adequacy and timeliness». PLOS ONE. 6 (9): e24278. Bibcode:2011PLoSO…624278S. doi:10.1371/journal.pone.0024278. PMC 3169586. PMID 21931669.
- ^ Developing Point of care HbA1c tests for Diabetes monitoring Archived 2008-08-29 at the Wayback Machine, Barry Plant, Originally Published IVDT July/August 2008
- ^ [Clinical Chemistry 50:1 166–174 (2004)]
- ^ a b HbA1c in a new way Archived 2022-07-13 at the Wayback Machine By the Swedish Diabetes Association. Retrieved Mars 2011
- ^ Geistanger A, Arends S, Berding C, Hoshino T, Jeppsson JO, Little R, Siebelder C, Weykamp C (August 2008). «Statistical methods for monitoring the relationship between the IFCC reference measurement procedure for hemoglobin A1c and the designated comparison methods in the United States, Japan, and Sweden». Clin. Chem. 54 (8): 1379–1385. doi:10.1373/clinchem.2008.103556. PMID 18539643.
- ^ Manley S, John WG, Marshall S (July 2004). «Introduction of IFCC reference method for calibration of HbA: implications for clinical care». Diabet. Med. 21 (7): 673–676. doi:10.1111/j.1464-5491.2004.01311.x. PMID 15209757. S2CID 30468208.
- ^ «Standardisation of the reference method for the measurement of HbA1c to improve diabetes care» (PDF). The Association for Clinical Biochemistry and Diabetss UK. April 2008. Archived from the original (PDF) on 2011-07-22. Retrieved 2009-07-02.
- ^ «HbA1c Standardisation For Laboratory Professionals» (PDF). Diabetes UK. Archived from the original (PDF) on 2011-07-20. Retrieved 2009-07-02.
- ^ «Executive Summary: Standards of medical care in diabetes – 2009». Diabetes Care. 32: S6–S12. 2009. doi:10.2337/dc09-S006. PMC 2613586. PMID 19118288.
- ^ Lehman R, Krumholz HM (2009). «Tight control of blood glucose in long standing type 2 diabetes». Br Med J. 338: b800. doi:10.1136/bmj.b800. PMID 19264821. S2CID 45188963.
- ^ Currie, Craig J; Peters, John R; Tynan, Aodán; Evans, Marc; Heine, Robert J; Bracco, Oswaldo L; Zagar, Tony; Poole, Chris D (2010). «Survival as a function of HbA1c in people with type 2 diabetes: a retrospective cohort study». The Lancet. 375 (9713): 481–489. doi:10.1016/S0140-6736(09)61969-3. PMID 20110121. S2CID 21223855.
- ^ «Advance Study Contradicts ACCORD Findings». Diabetes Self-Management. 2008-03-07. Retrieved 2013-06-10.
- ^ «The largest ever study of diabetes shows intensive glucose control reduces serious complications». Advance-trial.com. Archived from the original on 2013-01-16. Retrieved 2013-06-10.
- ^ Heller, Simon R. (2009-11-01). «A Summary of the Advance Trial». Diabetes Care. 32 (Suppl 2): S357–S361. doi:10.2337/dc09-S339. ISSN 0149-5992. PMC 2811451. PMID 19875581.
- ^ Shubrook JH, Shubrook J (2010). «Risks and benefits of attaining HbA(1c) goals: Examining the evidence». The Journal of the American Osteopathic Association. 110 (7 Suppl 7): e7–e12. PMID 20644204.
- ^ Gerstein HC, Miller ME, Byington RP, et al. (2008). «Effects of Intensive Glucose Lowering in Type 2 Diabetes». New England Journal of Medicine. 358 (24): 2545–2559. doi:10.1056/NEJMoa0802743. ISSN 0028-4793. PMC 4551392. PMID 18539917.
- ^ Kilpatrick ES, Bloomgarden ZT, Zimmet PZ (2009). «Is haemoglobin A1c a step forward for diagnosing diabetes?». BMJ. 339: b4432. doi:10.1136/bmj.b4432. PMID 19903702. S2CID 36941786.
- ^ a b Nathan DM, Kuenen J, Borg R, Zheng H, Schoenfeld D, Heine RJ (2008). «Translating the A1C assay into estimated average glucose values». Diabetes Care. 31 (8): 1473–1478. doi:10.2337/dc08-0545. PMC 2742903. PMID 18540046.
- ^ Saaddine, Jinan B.; Fagot-Campagna, Anne; Rolka, Deborah; Narayan, K. M. Venkat; Geiss, Linda; Eberhardt, Mark; Flegal, Katherine M. (2002-08-01). «Distribution of HbA(1c) levels for children and young adults in the U.S.: Third National Health and Nutrition Examination Survey». Diabetes Care. 25 (8): 1326–1330. doi:10.2337/diacare.25.8.1326. ISSN 0149-5992. PMID 12145229.
- ^ «Nationella Diabetesregistret Årsrapport 2014 års resultat» (PDF). Nationella Diabetesregistret Årsrapport 2014 års resultat (in Swedish). Nationella Diabetes Registret. Retrieved 2015-12-14.
- ^ Change to HbA1c values Archived 2014-03-01 at the Wayback Machine at Diabetes UK, 2013
- ^ «Executive summary: Standards of medical care in diabetes—2010». Diabetes Care. 33 (Suppl 1): S4–S10. January 2010. doi:10.2337/dc10-S004. PMC 2797389. PMID 20042774.
- ^ «Diagnosing Diabetes and Learning About Prediabetes». American Diabetes Association. Retrieved 2 December 2018.
- ^ American Diabetes Association (2007). «Standards of medical care in diabetes». Diabetes Care. 30 (Suppl 1): S4–S41. doi:10.2337/dc07-S004. PMID 17192377.
- ^ Dufresne, L.; Joly, J. G.; Lepage, R.; Lessard, F.; Bannon, P. (1984). «Glycated Hemoglobin in Uremic Patients as Measured by Affinity and Ion-Exchange Chromatography» (PDF). clinchem.com. pp. 485–486. doi:10.1093/clinchem/30.3.485. PMID 6697506. Retrieved 2009-08-31.
- ^ «Undetectable Glycosolated Hemoglobin in Autoimmune Hemolytic Anemia» (PDF). repository.oai.yamaguchi-u.ac.jp. Retrieved 2009-08-31.
- ^ The International Expert Committee (2009). «International expert committee report on the role of the A1C assay in the diagnosis of diabetes». Diabetes Care. 32 (7): 1327–1334. doi:10.2337/dc09-9033. PMC 2699715. PMID 19502545.
- ^ a b Sun J, Buys NJ (2016). «Glucose- and glycaemic factor-lowering effects of probiotics on diabetes: a meta-analysis of randomised placebo-controlled trials». British Journal of Nutrition. 115 (7): 1167–1177. doi:10.1017/S0007114516000076. PMID 26899960.
- ^ «Hypothyroidism Falsely Raises HbA1c and Glycated Albumin Levels». Diabetes In Control. 12 November 2010.
- ^ Kim, M. K.; Kwon, H. S.; Baek, K. H.; Lee, J. H.; Park, W. C.; Sohn, H. S.; Lee, K. W.; Song, K. H. (7 September 2010). «Effects of Thyroid Hormone on A1C and Glycated Albumin Levels in Nondiabetic Subjects With Overt Hypothyroidism». Diabetes Care. 33 (12): 2546–2548. doi:10.2337/dc10-0988. PMC 2992186. PMID 20823345.
- ^ Delack JB, Stogdale L (October 1983). «Glycosylated hemoglobin measurement in dogs and cats: implications for its utility in diabetic monitoring». Can Vet J. 24 (10): 308–311. PMC 1790442. PMID 17422317.
External links[edit]
- National Diabetes Information Clearinghouse Archived 2010-02-21 at the Wayback Machine
- American Diabetes Association Standards of Medical Care 2007
Диагноз «сахарный диабет» подтверждается при повышении уровня глюкозы. Проявление симптомов этого заболевания у человека служит поводом направить его на обследование, устанавливающее количество сахара в крови. В этих целях ВОЗ рекомендует анализ на гликированный гемоглобин – новый метод диагностики, позволяющий определить точный уровень глюкозы в кратчайшие сроки.

Что такое гликированный гемоглобин?
Гликированный, или гликозилированный гемоглобин – продукт слияния гемоглобина и глюкозы. Глюкоза проникает через мембрану эритроцита и связывается с гемоглобином в результате реакции Майяра: так называется неизбежное объединение сахара и аминокислоты, происходящее в организме.
Гликированный гемоглобин сокращённо называется гликогемоглобином.
В медицине для его обозначения используют такие сокращения:
- A1C;
- гемоглобин A1C.
В отличие от уровня свободной глюкозы в крови, уровень гликогемоглобина постоянен и не зависит от внешних факторов. Он сохраняет и показывает информацию о среднем уровне сахара в эритроцитах на протяжении всего срока их жизни.
Что показывает гликированный гемоглобин?
Гликогемоглобин – биохимический показатель крови, зависящий от среднего уровня глюкозы в крови. При его повышении слияние глюкозы и гемоглобина ускоряется, что приводит к увеличенному образованию гликированного гемоглобина.
Уровень HbA1C демонстрирует содержание сахара в крови за последние 120-125 дней: именно столько живут эритроциты, хранящие в себе информацию о количестве синтезированного гликогемоглобина.
 Это более стабильный тест, нежели исследование на глюкозотолерантность и измерение уровня глюкозы натощак. Он помогает вовремя выявить сахарный диабет и другие состояния, сопровождаемые повышенным или пониженным уровнем глюкозы в крови.
Это более стабильный тест, нежели исследование на глюкозотолерантность и измерение уровня глюкозы натощак. Он помогает вовремя выявить сахарный диабет и другие состояния, сопровождаемые повышенным или пониженным уровнем глюкозы в крови.
Нормы гликогемоглобина
Норма гликированного гемоглобина не зависит от пола или возраста: этот показатель одинаков у мужчин и у женщин, у детей и у людей преклонного возраста.
Для здорового человека используется таблица соответствия процентного соотношения гликогемоглобина в крови:
| Меньше 4.0% | Пониженный уровень гликогемоглобина. Требуется лечение. |
| От 4.0 до 5.5% | Нормальный уровень гликированного гемоглобина, риск возникновения сахарного диабета отсутствует. |
| От 5.6 до 6.0% | Риск возникновения диабета. Необходима корректировка образа жизни, питания и режима сна-бодрствования. |
| От 6.0 до 6.4% | Преддиабетное состояние. Нужна консультация эндокринолога для предотвращения появления болезни. |
| Больше 6.5% | Сахарный диабет. |
При беременности, из-за постоянных скачков гормонов и сахара, эти показатели могут отличаться. Нормой будет считаться гликированный гемоглобин не выше 6.0%. Если значение выше нормы, необходимо проконсультироваться с врачом: причина может быть в возникновении гестационного диабета.
При сахарном диабете, когда уровень гликозилированного гемоглобина повышен, норма его присутствия в крови устанавливается целевым уровнем.
Это – исчисляемое в процентах значение, указывающее оптимальное значение гликогемоглобина при разных показаниях:
| Осложнения | До 30 лет | От 30 до 50 лет | После 50 лет |
| Риск гипогликемии или серьёзных осложнений отсутствует | Меньше 6.5% | От 6.5 до 7.0% | От 7.0 до 7.5% |
| Высокий риск развития осложнений или тяжелой гипогликемии | От 6.5 до 7.0% | От 7.0 до 7.5% | От 7.5 до 8.0% |
Разделение по возрасту обусловлено опасностью гипогликемии для пожилых людей. В преклонном возрасте это заболевание может привести к летальному исходу, поэтому необходимо удерживать высокий уровень сахара в крови.
Причины отклонения от нормальных показателей
Отклонения от нормальных показателей гликогемоглобина возникают в результате различных заболеваний и патологических состояний в организме.
Самые распространённые причины:
| Повышение уровня HbA1C | |
| Сахарный диабет | Повышение уровня глюкозы в крови наблюдается при любом типе диабета. Снизить количество сахара можно при изменении образа жизни и применении инсулиновых препаратов. |
| Нарушение толерантности к глюкозе | Латентная форма сахарного диабета, возникающая в результате генетической предрасположенности, после осложненной беременности или из-за неправильного образа жизни. Если нарушение не корректировать, оно перерастает в диабет. |
| Заболевание селезёнка и спленэктомия | Селезёнка отвечает за утилизацию эритроцитов, поэтому серьёзные заболевания или удаление этого органа приводят к повышению гликогемоглобина в крови. |
| Приём лекарственных средств | Постоянное употребление стероидов, антидепрессантов, транквилизаторов и многих противозачаточных таблеток может повышать уровень глюкозы в крови. При сильном увеличении гликогемоглобина следует прекратить приём этих средств. |
| Эндокринные нарушения | Патологии эндокринной системы, провоцирующие большой выброс гормонов, нередко поднимают уровень глюкозы в крови. Эффект может быть временным или постоянным. |
| Снижение уровня HbA1C | |
| Гемолитическая анемия | При этом заболевании происходит разрушение эритроцитов, что снижает количество гемоглобина и гликогемоглобина в плазме. |
| Инсулинома | Опухоль поджелудочной железы, провоцирующая повышенный синтез инсулина. Он угнетает глюкозу и уменьшает ее количество в крови, что приводит к низкому гликированному гемоглобину. |
| Кровопотеря, переливание крови | При сильной кровопотере или во время переливания теряется часть эритроцитов, многие их которых могут содержать гликогемоглобин. Это и вызывает отклонение от нормы. |
| Длительная низкоуглеводная диета | Диета со сниженным содержанием углеводов уменьшает количество глюкозы в крови: она может синтезироваться из белков и жиров, но это происходит гораздо медленнее. В итоге гликогемоглобин падает ниже нормы. |
Как подготовиться к исследованию?
Сдача анализа на гликогемоглобин не требует особой подготовки. Его уровень не зависит от внешних факторов, поэтому перед исследованием можно есть и пить, заниматься спортом, принимать любые лекарственные препараты. Делать тест можно в любое удобное время суток, и это никак не скажется на результате.
Важно! Единственной причиной, почему предпочтительно сдавать анализ натощак, станет сгущение крови после еды. Повышения липидного уровня в плазме может сказаться на уровне гемоглобина, что слегка исказит результат диагностики.
Не стоит проводить тестирование при снижении уровня гемоглобина в крови, а также при изменении срока жизни эритроцитов.
Это может происходить:
- при кровопотере, в т.ч. во время менструации;
- при анемии: железодефицитной и гемолитической;
- после переливания крови;
- при тяжелой почечной недостаточности;
- при отравлении алкоголем или свинцом.
Также результат теста может искажаться при пониженном уровне гормонов щитовидной железы.

Как сдавать анализ
В зависимости от типа чувствительного анализатора, используемого в лаборатории, забор крови может производиться из вены или из пальца. В большинстве лабораторий для тестирования берут биоматериал из локтевой вены: считается, что этот метод демонстрирует более точный результат.
Объём забираемого материала составляет 3-3.5 мл, у некоторых пациентах при сдаче такого количество крови могут наблюдаться недомогания:
- тошнота;
- головокружение;
- изредка – потеря сознания.

Если вы плохо переносите сдачу венозной крови, необходимо заранее предупредить об этом лаборанта. Лучшим выходом из ситуации будет найти лабораторию, использующую для тестирования кровь из пальца.
Расшифровка анализа производится в течение 3-4 суток. Более точный срок зависит от конкретной лаборатории и её оборудования.
Как нормализовать гликированный гемоглобин
Чтобы понизить или повысить уровень глюкозы в крови, возвращая его к нормальным значениям, необходимо строго следовать предписаниям эндокринолога. Помимо консервативного лечения, на помощь придет смена образа жизни: подходящая диета, спорт и
Правильное питание
При диабете 2 типа и повышенном уровне гликогемоглобина пациенту рекомендуется лечебный стол №9. Диета ограничивает присутствие сахаросодержащих продуктов в рационе, заменяя их глюкозоподавляющими. Запрещены к употреблению белый хлеб, макароны и картофель, сладкие напитки и сахар. Разрешены овощи, жиры и мясные продукты.

При пониженном гликогемоглобине нужно потреблять больше протеинов и сложных углеводов. Рекомендуются орехи и бобовые, овощи, цельнозерновой хлеб, различные фрукты, нежирные мясные и молочные продукты. Не стоит употреблять кофеин, напитки с газом и блюда с высоким содержанием жира.
Если питаться правильно, уровень глюкозы быстро вернётся в норму.
Физические нагрузки
При высоком уровне глюкозы нужно включать в режим дня умеренные физические нагрузки, помогающие тратить больше глюкозы и поддерживающие тело в тонусе. Следует заниматься ходьбой и медленным бегом, плаванием, ездой на велосипеде, допустимы игры с мячом. Экстремальных видов спорта следует избегать.
При сниженном уровне гликогемоглобина следует воздержаться от спорта: даже небольшие нагрузки в таком состоянии могут навредить организму. 
Эмоциональное состояние
Кратковременное повышение уровня глюкозы в крови может происходить из-за стрессовых состояний, повышенной тревожности, расстройства, страха и депрессии. Также на количество сахара может влиять прием антидепрессантов.

Чтобы нормализовать эмоциональное состояние и решить психологические проблемы, провоцирующие увеличение сахара в крови, следует обратиться к психологу.
Анализ на гликогемоглобин – эффективный способ установления количества сахара. Он гораздо удобнее стандартных методов, потому что не зависит от внешних факторов и отображает средний уровень глюкозы за длительный срок.
Напоминаем вам, что самостоятельная интерпретация результатов недопустима, и приводимая ниже информация носит исключительно справочный характер.
Гликированный гемоглобин: показания к назначению, правила подготовки к сдаче анализа, расшифровка результатов и показатели нормы.
Показания для назначения исследования
Исследование на гликированный гемоглобин назначают с целью мониторинга течения и контроля эффективности лечения больных сахарным диабетом для определения степени компенсации заболевания. Уровень гликированного гемоглобина используют для оценки риска развития осложнений диабета.

Подготовка к процедуре
Специальной подготовки к процедуре не требуется. Исследование не проводится у детей до 6 месяцев. Исследование нецелесообразно проводить после кровотечений, гемотрансфузий (переливания крови).
Срок исполнения
1 рабочий день (указанный срок не включает день взятия биоматериала).
Что может повлиять на результаты
Результаты теста на гликированный гемоглобин при гемоглобинопатии, включая серповидно-клеточную анемию, во время беременности (второго и третьего триместров) и послеродового периода, при ВИЧ, недавних кровотечениях или переливании крови, терапии эритропоэтином, а также у пациентов, находящихся на гемодиализе, могут не отражать истинного содержания глюкозы.
Для диагностики диабета в этих ситуациях следует использовать только критерии уровня глюкозы в плазме крови.
Интерпретация результата может быть затруднена присутствием вариантных форм гемоглобина: гемоглобина А2, повышающегося при бета-талассемии (генетическом заболевании), и фетального гемоглобина (гемоглобина плода), высокое содержание которого сохраняется до 6 месяцев после рождения.
Гликированный гемоглобин
Для исследования берется кровь из вены.
Сдать анализ на Гликированный гемоглобин можно в ближайшем медицинском офисе ИНВИТРО. Список офисов, где принимается биоматериал для лабораторного исследования, представлен в разделе «Адреса».
Референсные значения представлены в таблице
| Гликированный гемоглобин, % | Интерпретация |
| < 6,0 | нормальный уровень |
| ≥ 6,5 | диагностический критерий сахарного диабета |
|
6,0 – 6,5 (5,7 – 6,4) |
повышенный риск развития диабета и его осложнений по данным ВОЗ (по данным ADA, American Diabetes Association) |
Гемоглобин – это переносящий кислород белок эритроцитов. В зависимости от структуры различают:
- нормальный гемоглобин (обозначают HbA), который составляет 85-95% от общего гемоглобина;
- гемоглобин А2 (HbA2), который составляет менее 3,5% от общего содержания гемоглобина;
- фетальный гемоглобин (HbF) — у взрослого человека составляет менее 1%.
Кислород, присоединяясь к гемоглобину, находящемуся в эритроцитах, доставляется к органам и тканям организма, где он нужен для их нормального функционирования.
При различных заболеваниях происходит химическое изменение структуры гемоглобина. Так, при сахарном диабете (заболевании, связанном с нарушением усвоения глюкозы, в результате чего развивается гипергликемия – стойкое увеличение содержания глюкозы в крови) к гемоглобину присоединяется глюкоза с образованием гликированного гемоглобина (обозначается HbA1c). И чем выше уровень глюкозы в крови, тем больше гемоглобина модифицируется в гликированный гемоглобин.

Образование гликированного гемоглобина необратимо (то есть гликированный гемоглобин не может обратно стать нормальным гемоглобином), и его концентрация в крови зависит как от продолжительности жизни эритроцитов (до 120 дней), так и от концентрации глюкозы в крови. Поскольку скорость образования гликированного гемоглобина тем выше, чем выше уровень глюкозы в крови, то по его концентрации можно судить о среднем содержании глюкозы в крови за последние 8–12 недель перед исследованием. При этом содержание гликированного гемоглобина не зависит от ежедневных и часовых колебаний глюкозы, от физических нагрузок и приема пищи непосредственно перед взятием образца крови.
Проведение исследования на гликированный гемоглобин рекомендуется всем людям старше 45 лет для своевременной оценки риска развития диабета и его осложнений (не реже 1 раза в три года).
Если присутствует хотя бы один из факторов риска развития диабета (избыточный вес, сердечно-сосудистые заболевания, гипертония (АД ≥ 140/90 мм.рт.ст.), родственники, страдающие диабетом, нарушение обмена холестерина (уровень ЛПВП (липопротеинов высокой плотности) < 0,9 ммоль/л) или уровень триглицеридов > 2,82 ммоль/л) необходимо контролировать уровень глюкозы, исследуя гликированный гемоглобин не реже 1 раза в год.
Пациентам с установленным диагнозом «сахарный диабет» исследование концентрации гликированного гемоглобина рекомендовано делать каждые три месяца для контроля эффективности лечения и оценки риска развития осложнений:
- ретинопатии (поражения сетчатки глаза, которое в тяжелых случаях может заканчиваться слепотой);
- нефропатии (поражения почек);
- полинейропатии (поражения нервных волокон, которое может приводить к атрофии (истощению) мышц);
- артериальной гипертензии (повышенного давления);
- атеросклероза (отложения холестерина в стенке сосудов);
- ИБС (ишемической болезни сердца).
Причины повышения гликированного гемоглобина в крови:
- Сахарный диабет.
- Ложное завышение при железодефицитной анемии.
- Ложное завышение после спленэктомии (удаления селезенки).
Причины снижения гликированного гемоглобина в крови:
- Гипогликемия (низкое содержание глюкозы в крови).
- Нормализация уровня глюкозы у пациентов с диабетом (эффективное лечение).
- Ложное занижение при гемолитической анемии.
- Ложное занижение после кровотечения, гемотрансфузии (переливания крови).
Источники:
- Classification and Diagnosis of Diabetes: Standards of Medical Care in Diabetes—2021 American Diabetes Association Diabetes Care Jan 2021, 44 (Supplement 1) S15-S33; DOI:10.2337/dc21-S002
- Клинические рекомендации «Сахарный диабет 1 типа у взрослых». Разраб.: Российская ассоциация эндокринологов. – 2019.
- Клинические рекомендации «Сахарный диабет 1 типа у детей». Разраб.: Российская ассоциация эндокринологов. – 2019.
- Клинические рекомендации «Сахарный диабет 2 типа у взрослых». Разраб.: Российская ассоциация эндокринологов. – 2019.
ВАЖНО!
Информацию из данного раздела нельзя использовать для самодиагностики и самолечения. В случае боли или иного обострения заболевания диагностические исследования должен назначать только лечащий врач. Для постановки диагноза и правильного назначения лечения следует обращаться к Вашему лечащему врачу.
Для корректной оценки результатов ваших анализов в динамике предпочтительно делать исследования в одной и той же лаборатории, так как в разных лабораториях для выполнения одноименных анализов могут применяться разные методы исследования и единицы измерения.
Анализ крови на гликированный гемоглобин

- Врачи
- Статья обновлена: 18 июня 2020
Сахарный диабет — это заболевание, от которого никто не вправе считать себя защищённым, даже если диагноз ещё не поставлен.
Сахарный диабет — это заболевание, от которого никто не вправе считать себя защищённым, даже если диагноз ещё не поставлен. По данным Международной Диабетической Федерации на 2015 год, в мире 415 миллионов диабетиков. В России их 12 миллионов, по некоторым данным — 17, то есть каждый десятый. К 2040 году ожидается увеличение количества больных в полтора раза. Каждый из нас может оказаться в их числе.
Симптомы сахарного диабета
Если у Вас возникли подозрения, Вы заметили три тревожных симптома — «три П» (полидипсия — неестественно сильная жажда, полифагия — неутолимый голод и полиурия — выделение более 2 литров в мочи в сутки), задумайтесь, не пора ли к врачу.
Диагностика
Самый точный из доступных нам методов контроля — анализ на гликированный гемоглобин. Для него не нужна подготовка, и этот анализ надёжнее определения уровня сахара в крови.
Что такое гликированный гемоглобин?
Гликированным, или гликозилированным, называется гемоглобин, связанный с глюкозой (сокращенно «гликогемоглобин»). Как известно, гемоглобин содержится в красных кровяных тельцах — эритроцитах. Сахара проникают через мембрану эритроцита и взаимодействуют с гемоглобином, при этом получается гликогемоглобин. В отличие от уровня свободной, несвязанной с гемоглобином глюкозы, уровень гликированного гемоглобина остаётся в крови относительно постоянным, потому что в норме гемоглобин внутри эритроцитов стабилен. Отработав 4 месяца на транспортировке кислорода и углекислого газа, эритроциты разрушаются в красной пульпе селезёнки. Их гемоглобин и гликогемоглобин распадаются в селезёнке и печени. Конечный продукт распада гемоглобина — билирубин — с сахаром не связывается.
Как раз потому, что эритроциты крови живут 4 месяца, уровень гликогемоглобина сохраняется постоянным 120 дней. На него не влияет время суток, физические нагрузки, приём пищи, эмоциональное состояние.
О чём говорит этот показатель?
Содержание гликированного гемоглобина пропорционально содержанию сахара в крови — гликемии. Чем выше её уровень, тем больше гемоглобина свяжется с глюкозой и тем сильнее поднимется уровень гликированного гемоглобина. И для диабетиков, и для тех, кто не болен, повышение уровня гликогемоглобина — это повод обратиться к врачу. Пациентам назначают терапию или рекомендуют вовремя изменить образ жизни. Для предупреждения заболевания назначают низкоуглеводную диету.
Соответствие показателей гликированного гемоглобина (HbA1C) и среднего уровня глюкозы в крови за 3 месяца
| HbA1C, % | Глюкоза, ммоль/л | Что это значит |
|---|---|---|
| 4 | 3,8 | Обмен углеводов протекает нормально, риск диабета минимальный |
| 4,5 | 4,6 | |
| 5 | 5,4 | |
| 5,5-5,7 | 6,5 | |
| 5,7-6,0 | 6,5-7,0 | Повышенный риск сахарного диабета. Желательно ограничить употребление сладкого и обратиться к врачу-эндокринологу. |
| 6,1-6,4 | 7,0-7,8 | Высокий риск диабета. Необходимо обратиться к врачу-эндокринологу. |
| 6,5 и более | 7,9 и более | Диагноз «сахарный диабет» ставится предварительно. Для подтверждения или опровержения нужны дополнительные тесты. |
Недостатки показателя
Единственное уязвимое место метода — случай, когда с кровью пациента проводятся манипуляции. Переливания крови искажают картину, потому что показатели гликозилированного гемоглобина донора и реципиента различаются. Но это проявляется и при обычной работе с глюкометром. Кровотечения или гемолиз (разрушение эритроцитов крови) вызывают ложное снижение результата, а при железодефицитной анемии ожидайте ложное повышение.
Назначение метода
Анализ на гликированный гемоглобин разрешит сомнения тех, чей уровень глюкозы в крови — на грани нормы, и покажет истинную картину, если пациент не придерживался диеты последние 3-4 месяца, а за неделю до очередных анализов прекратил употреблять в пищу сладкое в надежде, что никто не узнает о несоблюдении им рекомендаций врача.
Частота измерений
Если диагноз уже поставлен, то обращение к специалисту поможет узнать, с какой регулярностью лучше сдавать анализ для контроля лечения. При отсутствии жалоб сроки посещения эндокринолога устанавливает врач. Срок жизни эритроцита устанавливает частоту анализа, с которой нужно сдавать кровь — 3 раза в год. При отсутствии и жалоб и негативной динамики чаще обращаться к эндокринологу не нужно.
Алина Петяева
Источники
- Ribeiro de Lima JG., Abud GF., Freitas EC., Bueno Júnior CR. Effects of the COVID-19 pandemic on the global health of women aged 50 to 70 years. // Exp Gerontol — 2021 — Vol150 — NNULL — p.111349; PMID:33892133
- Manaer T., Yu L., Nabi XH., Dilidaxi D., Liu L., Sailike J. The beneficial effects of the composite probiotics from camel milk on glucose and lipid metabolism, liver and renal function and gut microbiota in db/db mice. // BMC Complement Med Ther — 2021 — Vol21 — N1 — p.127; PMID:33888105
- Mani Deepthi D., Vaikkakara S., Patil A., Ganta S., Sachan A., Raghavendra K., Kiranmayi VS., Chowhan AK. Effect of Correction of Hyperthyroidism with Anti-thyroid Drugs on the Glycated Hemoglobin in Non-diabetic Patients with Primary Hyperthyroidism. // Int J Endocrinol Metab — 2021 — Vol19 — N1 — p.e105751; PMID:33815517
- Pohanka M. Glycated Hemoglobin and Methods for Its Point of Care Testing. // Biosensors (Basel) — 2021 — Vol11 — N3 — p.; PMID:33806493
- Hu X., Deng H., Zhang Y., Guo X., Cai M., Ling C., Li K. Efficacy and Safety of a Decision Support Intervention for Basal Insulin Self-Titration Assisted by the Nurse in Outpatients with T2DM: A Randomized Controlled Trial. // Diabetes Metab Syndr Obes — 2021 — Vol14 — NNULL — p.1315-1327; PMID:33790599
- Okamoto T., Shima H., Noma Y., Komatsu M., Azuma H., Miya K., Tashiro M., Inoue T., Masaki C., Tada H., Takamatsu N., Minakuchi J. Hereditary spherocytosis diagnosed with extremely low glycated hemoglobin compared to plasma glucose levels. // Diabetol Int — 2021 — Vol12 — N2 — p.229-233; PMID:33786277
- Mazahery H., Gammon CS., Lawgun D., Conlon CA., Beck KL., von Hurst PR. Pre-diabetes prevalence and associated factors in New Zealand school children: a cross-sectional study. // N Z Med J — 2021 — Vol134 — N1531 — p.76-90; PMID:33767489
- Abbas E., Ahmed Siddiqui I., Khan MS., Perveen K., Butt A., Fawwad A. Fasting Glucagon Level in Type 2 Diabetes and Impaired Glucose Tolerance and Its Association With Diabetes-Associated Clinical Parameters: A Study From Karachi, Pakistan. // Cureus — 2021 — Vol13 — N2 — p.e13430; PMID:33758717
- Alkethiri K., Almtroudi T., Jurays AB., Abanumay F., Aldammas M., AlKhodheer M., Iqbal M., Habib SS., Bashir S. The relationship between type 2 diabetes mellitus with cognitive functions. // Heliyon — 2021 — Vol7 — N3 — p.e06358; PMID:33748460
- Jaber H., Issa K., Eid A., Saleh FA. The therapeutic effects of adipose-derived mesenchymal stem cells on obesity and its associated diseases in diet-induced obese mice. // Sci Rep — 2021 — Vol11 — N1 — p.6291; PMID:33737713
Консультация врача-кардиолога, к.м.н., первичная 6 240 руб.
Консультация врача-кардиолога, к.м.н., повторная 4 360 руб.
Консультация врача-кардиолога, д.м.н./профессора 9 990 руб.
Дуплексное сканирование брюшной аорты и ее висцеральных ветвей (УЗИ брюшной аорты и ее ветвей (триплексное сканирование аорты и ее ветвей) 4 400 руб.
Дуплексное сканирование нижней полой вены и вен портальной системы (УЗИ нижней полой вены и ее притоков (выполненное д.м.н., профессором) 6 600 руб.
Дуплексное сканирование нижней полой вены и вен портальной системы (УЗИ нижней полой вены и ее притоков) 4 400 руб.
Дуплексное сканирование артерий верхних конечностей (УЗИ артерий нижних конечностей (УЗТГ- измерение давления на одной в/к и лодыжечного давления на обеих н/к при ультразвуковой допплерографии; ТС – триплексное сканирование артерий н/к.) (выполненное д.м. 11 000 руб.
Консультация врача-гастроэнтеролога, к.м.н., первичная 6 240 руб.
Консультация врача-гастроэнтеролога, к.м.н., повторная 4 360 руб.
Прием (осмотр, консультация) врача-пульмонолога, д.м.н./профессора 17 010 руб.
Прием (осмотр, консультация) врача-пульмонолога, к.м.н., первичный 6 240 руб.
Консультация врача-ревматолога, д.м.н./профессора 9 990 руб.
Консилиумное экспертное решение (для пациентов, нуждающихся в проведении хирургического лечения сердца и сосудов) (в составе сердечно-сосудистого хирурга, эндоваскулярного хирурга, сосудистого хирурга, кардиолога, эндокринолога и пр.) 13 200 руб.
Запись и расшифровка ЭКГ с использованием 12-ти канального электрокардиографа 2 550 руб.
Холтеровское мониторирование сердечного ритма (Холтер) (Суточное мониторирование ЭКГ до 24 часов при непрерывной записи) 5 790 руб.
Холтеровское мониторирование сердечного ритма (Холтер) (48-часовое ЭКГ-мониторирование) 7 700 руб.
Холтеровское мониторирование сердечного ритма (Холтер) (24-часовое ЭКГ мониторирование + дыхание) 6 600 руб.
Холтеровское мониторирование сердечного ритма (Холтер) (48-часовое ЭКГ мониторирование + дыхание) 9 900 руб.
Холтеровское мониторирование сердечного ритма (Холтер) (72-часовое ЭКГ мониторирование + дыхание) 13 200 руб.
Холтеровское мониторирование сердечного ритма (Холтер) (120-часовое ЭКГ-мониторирование + дыхание) 17 600 руб.
Холтеровское мониторирование сердечного ритма (Холтер) (24-часовое ЭКГ-мониторирование (12 отведений) 8 800 руб.
Суточное мониторирование артериального давления (СМАД) (Суточное мониторирование АД до 24 часов при непрерывной записи) 5 430 руб.
Эхокардиография (ЭхоКГ/УЗИ сердца) 6 600 руб.
Эхокардиография с физической нагрузкой (Стресс-электрокардиография (Тредмил-тест с ЭКГ) 7 700 руб.
Эхокардиография с физической нагрузкой (Стресс-эхокардиография с тредмил-тестом и эхокардиографией по короткому протоколу) 11 000 руб.
Эхокардиография с физической нагрузкой (Стресс-эхокардиография с тредмил-тестом и эхокардиографией по расширенному протоколу) 16 500 руб.
Дуплексное сканирование вен или артерий (Ультразвуковая допплерография артерий или вен 2-х конечностей (выполненное д.м.н., профессором)) 8 470 руб.
Дуплексное сканирование вен или артерий (Ультразвуковая допплерография артерий или вен 2-х конечностей) 6 270 руб.
Дуплексное сканирование брюшной аорты и ее висцеральных ветвей (УЗИ брюшной аорты и ее ветвей (триплексное сканирование аорты и ее ветвей) (выполненное д.м.н., профессором) 6 600 руб.
Дуплексное сканирование артерий верхних конечностей (УЗИ артерий нижних конечностей (УЗТГ- измерение давления на одной в/к и лодыжечного давления на обеих н/к при ультразвуковой допплерографии; ТС – триплексное сканирование артерий н/к.) 7 700 руб.
Дуплексное сканирование брахиоцефальных артерий и вен (УЗТС брахиоцефальных артерий и вен (УЗДГ-измерение АД и ВД на обеих в/к, пробы с отведением в/к при УЗДГ; ТС Б/Ц артерий и вен шеи с функциональными пробами; ТКДГ артерий и вен с функциональными проба 11 000 руб.
Дуплексное сканирование брахиоцефальных артерий и вен (УЗТС брахиоцефальных артерий и вен (УЗДГ-измерение АД и ВД на обеих в/к, пробы с отведением в/к при УЗДГ; ТС Б/Ц артерий и вен шеи с функциональными пробами; ТКДГ артерий и вен с функциональными проба 8 800 руб.
Консультация врача-ревматолога, к.м.н., первичная 6 240 руб.
Консультация врача-ревматолога, к.м.н., повторная 4 360 руб.
Боли в суставах: расширенное обследование (АСЛ-О, С-реактивный белок,ревматоидный фактор,Остеокальцин,Дезоксипиридинолин (моча),Паратиреоидный гормон, АТ класса IgA, IgG к антигенам 18 220 руб.
Антитела к ревматоидному фактору (RF) IgM, качественное определение 2 300 руб.
Ревматоидный фактор, IgA (РФ IgA, Rheumatoid Factor, RF, IgA) 2 090 руб.
Дифференциальная диагностика СКВ и других ревматических заболеваний 4 440 руб.
Ревматоидный фактор (РФ, Rheumatoid factor, RF) 1 060 руб.
Ревматоидный фактор (Rheumatoid factor) 1 130 руб.
Исследование функции внешнего дыхания 4 530 руб.
Функция внешнего дыхания и газы крови 6 000 руб.
Исследование функции внешнего дыхания с бронхолитиком 7 550 руб.
Гастроскопия «во сне» 14 470 руб.
Гастроскопия + Колоноскопия «во сне» 24 150 руб.
Гастропанель (Пепсиноген-I, пепсиноген-II, гастрин-17 базальный, anti-Helicobacter pylori IgG) 10 890 руб.
Опубликовано: 16.04.2012 Обновлено: 12.10.2022 Просмотров: 299240

Очень важно при ведении больных сахарным диабетом добиться оптимального содержания глюкозы в крови. Контроль уровня глюкозы в крови больной может проводить самостоятельно (портативными глюкометрами) или в лаборатории.
Результат единичного определения глюкозы в крови показывает концентрацию глюкозы на момент взятия, поэтому сделать какие-либо предположения о состоянии углеводного обмена больного между измерениями не представляется возможным. Оценить углеводный обмен у больного за длительный период времени можно, только измеряя концентрацию гликозилированного гемоглобина в крови, согласно рекомендациям Комитета по контролю за диабетом и его клиническими осложнениями (DCCT).
По данным исследований, проводимых DCCT, было показано, что риск развития и прогрессирования отдаленных осложнений диабета 1 типа тесно связан со степенью эффективности контроля уровня гликемии, выраженного в содержании гликозилированного гемоглобина в крови [10]. Специалистами из Великобритании было показано, что снижение содержания глюкозы в крови пациента, оцененное по концентрацииHbA1с, уменьшает частоту микроангиопатий при сахарном диабете 2 типа [4].
Характеристика показателя
Гликозилированный гемоглобин (употребляется также термин «гликированный гемоглобин») образуется в результате неферментативного присоединения глюкозы к N-концевым участкам β-цепей глобина гемоглобина А1 и обозначается как HbA1c. Концентрация HbA1c прямо пропорциональна средней концентрации глюкозы в крови. У здоровых концентрация HbA1c в крови от 4,80 до 5,90%, у больных сахарным диабетом его уровень в 2-3 раза выше (в зависимости от степени гипергликемии).
Образовавшийся HbA1 cаккумулируется внутри эритроцитов и сохраняется в течение всего срока жизни эритроцита. Полупериод циркуляции эритроцита в кровяном русле составляет 60 суток, таким образом, концентрация HbA1c отражает уровень гликемии пациента за 60-90 дней до исследования [2, 3].
Огромное число исследований с использованием традиционных методов измерения содержания глюкозы подтвердило взаимосвязь HbA1c и уровня гликемии пациента [12-14]. Результаты исследований, проведенных DCCT в 90-х годах, послужили основанием для подтверждения гипотезы о том, что уровень HbA1c отражает уровень глюкозы в крови и является эффективным критерием при мониторинге больных сахарным диабетом.
Стандартизация методов исследования гликозилированного гемоглобина
В начале 90-х годов не существовало межлабораторной стандартизации методов измерения гликозилированного гемоглобина, что снижало клиническую эффективность использования данного теста [15-17]. В связи с этим Американская Ассоциация клинической химии в 1993 году сформировала подкомитет по стандартизации методов измерения гликозилированного гемоглобина. В результате его работы была разработана Национальная программа по стандартизации исследований гликозилированного гемоглобина (NGSP). Производителей тест-систем для измерения гликозилированного гемоглобина обязали проходить строжайшую проверку на соответствие результатов с данными, полученными референсными методами DCCT. В случае положительного результата проверки производителю выдается «сертификат соответствия DCCT». Американская Диабетическая Ассоциация рекомендует всем лабораториям пользоваться только тестами, сертифицированными NGSP [7].
Методов исследования гликозилированного гемоглобина в настоящее время существует много:
- жидкостная хроматография;
- аффинная хроматография;
- электрофорез;
- колоночные методики;
- иммунологические методики.
При выборе лабораторией анализатора для исследования гликозилированного гемоглобина преимущество должно отдаваться анализаторам на основе референсного метода DCCT, каким является жидкостная хроматография. Использование стандартизированных методов исследования дает лаборатории возможность получать результаты, которые можно сравнивать с данными, полученными с помощью референсных методов и опубликованными DCCT. Такое сравнение максимально повышает достоверность результатов исследований.
Чрезвычайно важно, чтобы лечащий врач использовал в своей работе результаты исследований, полученные только в тех лабораториях, которые проводят исследование гликозилированного гемоглобина методами сертифицированными NGSP.
Исследование концентрации HbA1c в лабораториях Ассоциации «Ситилаб»
Концентрация гликозилированного гемоглобина (HbA1c) в лабораториях Ассоциации «Ситилаб» определяется референсным методом (DCCT) высокоэффективной жидкостной хроматографии (ВЭЖК), (метод сертифицирован NGSP), на анализаторах D 10 фирмы «Bio-Rad», которая является мировым лидером в производстве анализаторов гликозилированного гемоглобина. Это исследование 23-10-002 — Гликозилированный гемоглобин.
Оценка среднего содержания глюкозы в крови
Исследовательская группа при DCCT продемонстрировала клиническую значимость показателя HbA1c, как оценку средней концентрации глюкозы в крови (за 60-90 дней). В этих исследованиях у пациентов раз в 3 месяца регистрировали дневной профиль содержания глюкозы (по семи измерениям ежедневно). Полученный профиль сопоставляли с уровнемHbA1c. В течение 9 лет было проведено более 36 000 исследований. Эмпирически была получена линейная зависимость среднего содержания глюкозы и уровня HbA1c:
Средняя концентрация глюкозы (мг/100 мл)=30,9 х (HbA1c)-60,6, где:
HbA1c — концентрация гликозилированного гемоглобина.
Проще говоря, изменение HbA1c на 1% соответствует изменению среднего содержания глюкозы на 30 мг/100 мл (1,7 ммоль/л).
Примечание: Указанная взаимосвязь была получена при исследовании концентрации глюкозы в капиллярной крови. Концентрация глюкозы в сыворотке крови приблизительно на 15% выше.
Для интерпретации результатов исследований HbA1c может быть использована диаграмма (рис. 1) [11].

Рис. 1. Диаграмма контроля углеводного обмена у больных сахарным диабетом
Примечание: Концентрация глюкозы указана в ммоль/л, в скобках в мг/100 мл, 1 — Высокий риск развития отдаленных осложнений, таких как ретинопатия, нефропатия и нейропатия. 2 — Повышенный риск возникновения гипогликемических реакций для пациентов с диабетом 1 или 2 типа при приеме инсулина или пероральных сахароснижающих препаратов.
Для пересчета концентрации глюкозы в мг/100 мл в единицы СИ (ммоль/л) используется следующая формула:
Глюкоза (мг/100 мл) х 0,0555 = Глюкоза (ммоль/л)
Рекомендуемая частота проведения исследования
Американская Диабетическая Ассоциация рекомендует для пациентов, чья терапия была успешной (стабильный уровень углеводного обмена), проводить исследование HbA1c не реже 2-х раз в год, тогда как в случае изменения диеты или лечения следует увеличить частоту обследования до 4-х раз в год [7]. В Российской Федерации, согласно Целевой Федеральной программе «Сахарный диабет», исследование HbA1c должно проводиться 4 раза в год при любом типе диабета [1].
Согласно рекомендациям Американской Диабетической Ассоциации, женщины, больные сахарным диабетом, в период предшествующий беременности, нуждаются в специальном режиме мониторинга. Рекомендуется снизить уровень HbA1c для создания в организме будущей матери оптимальных условий для зачатия и развития плода. В начале HbA1cнеобходимо исследовать ежемесячно. Когда при соответствующей терапии углеводный обмен стабилизируется, исследование HbA1c необходимо проводить с интервалом 6-8 недель до момента зачатия [5, 6].
Современные исследования показали, что многие пациенты не соблюдают рекомендованный интервал между исследованиями [8], однако эксперты пришли к общему мнению, что регулярные исследования содержания HbA1c существенно снижают риск развития осложнений у больных сахарным диабетом.
Интерпретация результатов исследования
Задачей сахароснижающей терапии при сахарном диабете является нормализация уровня глюкозы в крови. Исследования в рамках DCCT показали, что интенсивное лечение предохраняет пациента от развития отдаленных осложнений, таких как ретинопатия, нефропатия и нейропатия, или значительно отодвигает срок их клинического проявления. Если пациенты строго придерживаются режима, направленного на нормализацию углеводного обмена, частота возникновения ретинопатии снижается на 75%, нефропатии — на 35-36%, на 60% уменьшается риск полинейропатий [10].
Ниже представлены терапевтические цели при лечении сахарного диабета по данным Целевой Федеральной программы «Сахарный диабет».
Таблица 1.
Терапевтические цели при лечении сахарного диабета 1 типа [1, 18]
|
Наименование исследования |
Референсные значения |
Адекватный уровень |
Неадекватный уровень |
|
|
Самоконтроль глюкозы крови, ммоль/л (мг%) |
натощак |
4,0 — 5,0 (70 — 90) |
5,1 — 6,5 (91 — 117) |
>6,5 (>117) |
|
через 2 часа после еды |
4,0 — 7,5 (70 — 135) |
7,6 — 9,0 (136 — 162) |
>9,0 (>162) |
|
|
перед сном |
4,0 — 5,0 (70 — 90) |
6,0 — 7,5 (110 — 135) |
>7,5 (>135) |
|
|
HbA1c |
<6 |
6,1 — 7,5 |
> 7,5 |
Таблица 2.
Терапевтические цели при лечении сахарного диабета 2 типа [1, 19]
|
Наименование исследования |
Низкий риск ангиопатий |
Риск макроангиопатий |
Риск микроангиопатий |
|
|
Самоконтроль глюкозы крови, ммоль/л (мг%) |
натощак |
<5,5 (<100) |
>5,5 (>100) |
>6,0 (>110) |
|
через 2 часа после еды |
<7,5 (<135) |
>7,5 (>135) |
>9,0 (>160) |
|
|
HbA1c |
<6,5 |
>6,5 |
>7,5 |
Примечание: В скобках указаны значения глюкозы в мг/100 мл.
Федеральной целевой программой «Сахарный диабет» [1], были приняты значения, рекомендованные Европейской Рекомендательной Комиссией по Диабету [18, 19].
При оценке результатов лечения у пациентов с сопутствующими заболеваниями, лиц младшего возраста, пожилых людей, беременных женщин и больных с необычной картиной течения сахарного диабета необходимо применять другие критерии стабилизации углеводного обмена.
При неадекватном уровне углеводного обмена у пациента необходимы дополнительные меры, которые зависят от клинической картины заболевания пациента, такие меры могут включать в себя:
- расширенное обучение пациентов самоконтролю уровня глюкозы;
- организацию групп взаимоподдержки пациентов;
- регулярное обследование у эндокринолога;
- изменения в медикаментозной терапии;
- более частое исследование концентрации глюкозы и HbA1c.
Выводы
- Исследование HbA1c позволяет оценить уровень гликемии у больного сахарным диабетом за 60-90 дней предшествующих исследованию.
- Данное исследование дает возможность проводить мониторинг течения заболевания и контролировать адекватность проводимого лечения.
- Исследование HbA1c необходимо проводить для оценки риска развития осложнений у больного сахарным диабетом.
Используемая литература
- Дедов И.И., Шестакова М.В., Максимова М.А. Федеральная целевая программа «Сахарный диабет». // Москва, 2002, 84 С.
- Питерс — Хармел Э., Матур Р. Сахарный диабет. Диагностика и лечение. // Практика, 2008.
- Попова Ю.С. Сахарный диабет. // Крылов, 2008.
- ADA. Implications of the United Kingdom Prospective Diabetes Study (Position Statement). // Diabetes Care 1999, (SI), 27-31.
- ADA. Standards of Medical Care for Patients With Diabetes Mellitus (Position Statement). // Diabetes Care 1999, (SI), 32-41.
- ADA. Preconception Care of Women With Diabetes (Position Statement). // Diabetes Care 1999, (SI), 62-63.
- ADA. Tests of Glycemia in Diabetes (Position Statement). // Diabetes Care 1999, (SI), 77-79.
- Auxter S. Another Study Shows Laboratory Tests are Underutilized. // Clin Lab News 1998, 24(9): 24-5.
- Bodor G., Little R., Garrett N. et al. Standardization of Glycohemoglobin Determinations in the Clinical Laboratory: Three Years Experience. // Clin Chem 1992; 38: 2414-18.
- DCCT Research Group. The Effect of Intensive Treatment of Diabetes on the Development and Progression of Long — Term Complications in Insulin — Dependent Diabetes Mellitus. // Engl J Med 1993; 329: 977-86.
- Goldstein D.E., Little R.R. Bringing Order to Chaos: Standardizing the Hemoglobin A1c Assay. // Contemp Int Med 1997; 9(5): 27-32/
- Gonen B.A., Rubinstein A.H., Rochman H. et al. Hemoglobin A1: An Indicator of the Metabolic Control of Diabetic Patients. // The Lancet 1977, Oct 8; 2(804): 734-7.
- Koenig R.J., Peterson C.M., Kilo C. et al. Hemoglobin A1c as an Indicator of the Degree of Glucose Intolerance in Diabetes. // Diabetes 1976, 25(3): 230-2.
- Koenig R.J., Peterson C.M., Jones R.L. et al. Correlation of Glucose Regulation and Hemoglobin A1c in Diabetes Mellitus. // Engl J Med 1976, 295(8): 417-20.
- Little R.R., England J.D., Wiedmeyer H.M. et al. Interlaboratory Standardization of Glycated Hemoglobin Determinations. // Clin Chem 1986; 32: 358-60.
- Little R.R., England J.D., Wiedmeyer H.M. et al. Interlaboratory Comparison of Glycated Hemoglobin Results: College of American Pathologists (CAP) Survey Data. // Clin Chem 1991; 37: 1725-29.
- Little R.R., England J.D., Wiedmeyer H.M. et al. Interlaboratory Standardization of Measurements of Glycohemoglobin. // Clin Chem 1992; 38: 2472-78.
- European Diabetes Policy Group. Guidelines for a desktop guide to Type 1 (insulindependent) Diabetes Mellitus. — International Diabetes Federation European Region. — 1998.
- European Diabetes Policy Group. Guidelines for a desktop guide to Type 2 Diabetes Mellitus. — International Diabetes Federation European Region. — 1998 — 1999.