| Spirometry | |
|---|---|
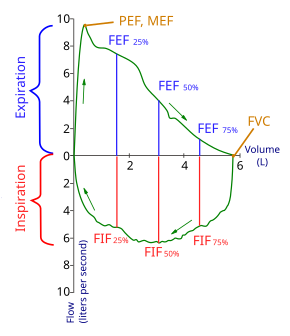
Flow-Volume loop showing successful FVC maneuver. Positive values represent expiration, negative values represent inspiration. At the start of the test both flow and volume are equal to zero (representing the volume in the spirometer rather than the lung). The trace moves clockwise for expiration followed by inspiration. After the starting point the curve rapidly mounts to a peak (the peak expiratory flow). (Note the FEV1 value is arbitrary in this graph and just shown for illustrative purposes; these values must be calculated as part of the procedure). |
|
| MeSH | D013147 |
| OPS-301 code | 1-712 |
 |
|
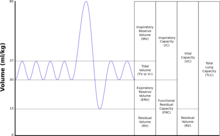
| TLC | Total lung capacity: the volume in the lungs at maximal inflation, the sum of VC and RV. |
|---|---|
| TV | Tidal volume: that volume of air moved into or out of the lungs during quiet breathing (TV indicates a subdivision of the lung; when tidal volume is precisely measured, as in gas exchange calculation, the symbol TV or VT is used.) |
| RV | Residual volume: the volume of air remaining in the lungs after a maximal exhalation |
| ERV | Expiratory reserve volume: the maximal volume of air that can be exhaled from the end-expiratory position |
| IRV | Inspiratory reserve volume: the maximal volume that can be inhaled from the end-inspiratory level |
| IC | Inspiratory capacity: the sum of IRV and TV |
| IVC | Inspiratory vital capacity: the maximum volume of air inhaled from the point of maximum expiration |
| VC | Vital capacity: the volume of air breathed out after the deepest inhalation. |
| VT | Tidal volume: that volume of air moved into or out of the lungs during quiet breathing (VT indicates a subdivision of the lung; when tidal volume is precisely measured, as in gas exchange calculation, the symbol TV or VT is used.) |
| FRC | Functional residual capacity: the volume in the lungs at the end-expiratory position |
| RV/TLC% | Residual volume expressed as percent of TLC |
| VA | Alveolar gas volume |
| VL | Actual volume of the lung including the volume of the conducting airway. |
| FVC | Forced vital capacity: the determination of the vital capacity from a maximally forced expiratory effort |
| FEVt | Forced expiratory volume (time): a generic term indicating the volume of air exhaled under forced conditions in the first t seconds |
| FEV1 | Volume that has been exhaled at the end of the first second of forced expiration |
| FEFx | Forced expiratory flow related to some portion of the FVC curve; modifiers refer to amount of FVC already exhaled |
| FEFmax | The maximum instantaneous flow achieved during a FVC maneuver |
| FIF | Forced inspiratory flow: (Specific measurement of the forced inspiratory curve is denoted by nomenclature analogous to that for the forced expiratory curve. For example, maximum inspiratory flow is denoted FIFmax. Unless otherwise specified, volume qualifiers indicate the volume inspired from RV at the point of measurement.) |
| PEF | Peak expiratory flow: The highest forced expiratory flow measured with a peak flow meter |
| MVV | Maximal voluntary ventilation: volume of air expired in a specified period during repetitive maximal effort |
|

Spirometry (meaning the measuring of breath) is the most common of the pulmonary function tests (PFTs). It measures lung function, specifically the amount (volume) and/or speed (flow) of air that can be inhaled and exhaled. Spirometry is helpful in assessing breathing patterns that identify conditions such as asthma, pulmonary fibrosis, cystic fibrosis, and COPD. It is also helpful as part of a system of health surveillance, in which breathing patterns are measured over time.[1]
Spirometry generates pneumotachographs, which are charts that plot the volume and flow of air coming in and out of the lungs from one inhalation and one exhalation.
Indications[edit]
Spirometry is indicated for the following reasons:
- to diagnose or manage asthma[2][3][4]
- to detect respiratory disease in patients presenting with symptoms of breathlessness, and to distinguish respiratory from cardiac disease as the cause[5]
- to measure bronchial responsiveness in patients suspected of having asthma[5]
- to diagnose and differentiate between obstructive lung disease and restrictive lung disease[5]
- to follow the natural history of disease in respiratory conditions[5]
- to assess of impairment from occupational asthma[5]
- to identify those at risk from pulmonary barotrauma while scuba diving[5]
- to conduct pre-operative risk assessment before anaesthesia or cardiothoracic surgery[5]
- to measure response to treatment of conditions which spirometry detects[5]
- to diagnose the vocal cord dysfunction.
Contraindications[edit]
Forced expiratory maneuvers may aggravate some medical conditions.[6] Spirometry should not be performed when the individual presents with:
- Hemoptysis of unknown origin
- Pneumothorax
- Unstable cardiovascular status (angina, recent myocardial infarction, etc.)
- Thoracic, abdominal, or cerebral aneurysms
- Cataracts or recent eye surgery
- Recent thoracic or abdominal surgery
- Nausea, vomiting, or acute illness
- Recent or current viral infection
- Undiagnosed hypertension
Spirometry testing[edit]

A modern USB PC-based spirometer.

Device for spirometry. The patient places his or her lips around the blue mouthpiece. The teeth go between the nubs and the shield, and the lips go over the shield. A noseclip guarantees that breath will flow only through the mouth.

Screen for spirometry readouts at right. The chamber can also be used for body plethysmography.
Spirometer[edit]
The spirometry test is performed using a device called a spirometer,[7] which comes in several different varieties. Most spirometers display the following graphs, called spirograms:
- a volume-time curve, showing volume (litres) along the Y-axis and time (seconds) along the X-axis
- a flow-volume loop, which graphically depicts the rate of airflow on the Y-axis and the total volume inspired or expired on the X-axis
Procedure[edit]
The basic forced volume vital capacity (FVC) test varies slightly depending on the equipment used, either closed circuit or open circuit, but should follow the ATS/ERS Standardisation of Spirometry.
Generally, the patient is asked to take the deepest breath they can, and then exhale into the sensor as hard as possible, for as long as possible, preferably at least 6 seconds. It is sometimes directly followed by a rapid inspiration, (inhalation) in particular when assessing possible upper airway obstruction. Sometimes, the test will be preceded by a period of quiet breathing in and out from the sensor (tidal volume), or the rapid breath in (forced inspiratory part) will come before the forced expiration.
During the test, soft nose clips may be used to prevent air escaping through the nose. Filter mouthpieces may be used to prevent the spread of microorganisms.
Limitations of test[edit]
The maneuver is highly dependent on patient cooperation and effort, and is normally repeated at least three times to ensure reproducibility. Since results are dependent on patient cooperation, FVC can only be underestimated, never overestimated.
Due to the patient cooperation required, spirometry can only be used on children old enough to comprehend and follow the instructions given (6 years old or more), and only on patients who are able to understand and follow instructions — thus, this test is not suitable for patients who are unconscious, heavily sedated, or have limitations that would interfere with vigorous respiratory efforts. Other types of lung function tests are available for infants and unconscious persons.
Another major limitation is the fact that many intermittent or mild asthmatics have normal spirometry between acute exacerbation, limiting spirometry’s usefulness as a diagnostic. It is more useful as a monitoring tool: a sudden decrease in FEV1 or other spirometric measure in the same patient can signal worsening control, even if the raw value is still normal. Patients are encouraged to record their personal best measures.

Example of a modern PC-based spirometer printout.
[edit]
Spirometry can also be part of a bronchial challenge test, used to determine bronchial hyperresponsiveness to either rigorous exercise, inhalation of cold/dry air, or with a pharmaceutical agent such as methacholine or histamine.
Sometimes, to assess the reversibility of a particular condition, a bronchodilator is administered before performing another round of tests for comparison. This is commonly referred to as a reversibility test, or a post bronchodilator test (Post BD), and is an important part in diagnosing asthma versus COPD.
Other complementary lung functions tests include plethysmography and nitrogen washout.
Parameters[edit]
The most common parameters measured in spirometry are Vital capacity (VC), Forced vital capacity (FVC), Forced expiratory volume (FEV) at timed intervals of 0.5, 1.0 (FEV1), 2.0, and 3.0 seconds, forced expiratory flow 25–75% (FEF 25–75) and maximal voluntary ventilation (MVV),[8] also known as Maximum breathing capacity.[9] Other tests may be performed in certain situations.
Results are usually given in both raw data (litres, litres per second) and percent predicted—the test result as a percent of the «predicted values» for the patients of similar characteristics (height, age, sex, and sometimes race and weight). The interpretation of the results can vary depending on the physician and the source of the predicted values. Generally speaking, results nearest to 100% predicted are the most normal, and results over 80% are often considered normal. Multiple publications of predicted values have been published and may be calculated based on age, sex, weight and ethnicity. However, review by a doctor is necessary for accurate diagnosis of any individual situation.
A bronchodilator is also given in certain circumstances and a pre/post graph comparison is done to assess the effectiveness of the bronchodilator. See the example printout.
Functional residual capacity (FRC) cannot be measured via spirometry, but it can be measured with a plethysmograph or dilution tests (for example, helium dilution test).

Average values for forced vital capacity (FVC), forced expiratory volume in 1 second (FEV1) and forced expiratory flow 25–75% (FEF25–75%), according to a study in the United States 2007 of 3,600 subjects aged 4–80 years.[10] Y-axis is expressed in litres for FVC and FEV1, and in litres/second for FEF25–75%.

Forced vital capacity (FVC)[edit]
Forced vital capacity (FVC) is the volume of air that can forcibly be blown out after full inspiration,[11] measured in liters. FVC is the most basic maneuver in spirometry tests.
Forced expiratory volume in 1 second (FEV1)[edit]
FEV1 is the volume of air that can forcibly be blown out in first 1-second, after full inspiration.[11] Average values for FEV1 in healthy people depend mainly on sex and age, according to the diagram.
Values of between 80% and 120% of the average value are considered normal.[12] Predicted normal values for FEV1 can be calculated and depend on age, sex, height, mass and ethnicity as well as the research study that they are based on.
FEV1/FVC ratio[edit]
FEV1/FVC is the ratio of FEV1 to FVC. In healthy adults this should be approximately 70–80% (declining with age).[13] In obstructive diseases (asthma, COPD, chronic bronchitis, emphysema) FEV1 is diminished because of increased airway resistance to expiratory flow; the FVC may be decreased as well, due to the premature closure of airway in expiration, just not in the same proportion as FEV1 (for instance, both FEV1 and FVC are reduced, but the former is more affected because of the increased airway resistance). This generates a reduced value (<70%, often ~45%). In restrictive diseases (such as pulmonary fibrosis) the FEV1 and FVC are both reduced proportionally and the value may be normal or even increased as a result of decreased lung compliance.
A derived value of FEV1 is FEV1% predicted (FEV1%), which is defined as FEV1 of the patient divided by the average FEV1 in the population for any person of the same age, height, gender, and race.[medical citation needed]
Forced expiratory flow (FEF)[edit]
Forced expiratory flow (FEF) is the flow (or speed) of air coming out of the lung during the middle portion of a forced expiration.
It can be given at discrete times, generally defined by what fraction of the forced vital capacity (FVC) has been exhaled.
The usual discrete intervals are 25%, 50% and 75% (FEF25, FEF50 and FEF75), or 25% and 50% of FVC that has been exhaled.
It can also be given as a mean of the flow during an interval, also generally delimited by when specific fractions remain of FVC, usually 25–75% (FEF25–75%). Average ranges in the healthy population depend mainly on sex and age, with FEF25–75% shown in diagram at left. Values ranging from 50 to 60% and up to 130% of the average are considered normal.[12] Predicted normal values for FEF can be calculated and depend on age, sex, height, mass and ethnicity as well as the research study that they are based on.
MMEF or MEF stands for maximal (mid-)expiratory flow and is the peak of expiratory flow as taken from the flow-volume curve and measured in liters per second. It should theoretically be identical to peak expiratory flow (PEF), which is, however, generally measured by a peak flow meter and given in liters per minute.[14]
Recent research suggests that FEF25-75% or FEF25-50% may be a more sensitive parameter than FEV1 in the detection of obstructive small airway disease.[15][16] However, in the absence of concomitant changes in the standard markers, discrepancies in mid-range expiratory flow may not be specific enough to be useful, and current practice guidelines recommend continuing to use FEV1, VC, and FEV1/VC as indicators of obstructive disease.[17][18]
More rarely, forced expiratory flow may be given at intervals defined by how much remains of total lung capacity. In such cases, it is usually designated as e.g. FEF70%TLC, FEF60%TLC and FEF50%TLC.[14]
Forced inspiratory flow 25–75% or 25–50%[edit]
Forced inspiratory flow 25–75% or 25–50% (FIF 25–75% or 25–50%) is similar to FEF 25–75% or 25–50% except the measurement is taken during inspiration.[medical citation needed]
Peak expiratory flow (PEF)[edit]

Normal values for peak expiratory flow (PEF), shown on EU scale.[19]
Peak expiratory flow (PEF) is the maximal flow (or speed) achieved during the maximally forced expiration initiated at full inspiration, measured in liters per minute or in liters per second.
Tidal volume (TV)[edit]
Tidal volume is the amount of air inhaled or exhaled normally at rest.[medical citation needed]
Total lung capacity (TLC)[edit]
Total lung capacity (TLC) is the maximum volume of air present in the lungs.[medical citation needed]
Diffusing capacity (DLCO)[edit]
Diffusing capacity (or DLCO) is the carbon monoxide uptake from a single inspiration in a standard time (usually 10 seconds). During the test the person inhales a test gas mixture that consisting of regular air that includes an inert tracer gas and CO, less than one percent. Since hemoglobin has a greater affinity to CO than oxygen the breath-hold time can be only 10 seconds, which is a sufficient amount of time for this transfer of CO to occur. Since the inhaled amount of CO is known, the exhaled CO is subtracted to determine the amount transferred during the breath-hold time. The tracer gas is analyzed simultaneously with CO to determine the distribution of the test gas mixture. This test will pick up diffusion impairments, for instance in pulmonary fibrosis.[20] This must be corrected for anemia (a low hemoglobin concentration will reduce DLCO) and pulmonary hemorrhage (excess RBC’s in the interstitium or alveoli can absorb CO and artificially increase the DLCO capacity). Atmospheric pressure and/or altitude will also affect measured DLCO, and so a correction factor is needed to adjust for standard pressure.
Maximum voluntary ventilation (MVV)[edit]
Maximum voluntary ventilation (MVV) is a measure of the maximum amount of air that can be inhaled and exhaled within one minute. For the comfort of the patient this is done over a 15-second time period before being extrapolated to a value for one minute expressed as liters/minute. Average values for males and females are 140–180 and 80–120 liters per minute respectively.[medical citation needed]
Static lung compliance (Cst)[edit]
When estimating static lung compliance, volume measurements by the spirometer needs to be complemented by pressure transducers in order to simultaneously measure the transpulmonary pressure. When having drawn a curve with the relations between changes in volume to changes in transpulmonary pressure, Cst is the slope of the curve during any given volume, or, mathematically, ΔV/ΔP.[21] Static lung compliance is perhaps the most sensitive parameter for the detection of abnormal pulmonary mechanics.[22] It is considered normal if it is 60% to 140% of the average value in the population for any person of similar age, sex and body composition.[12]
In those with acute respiratory failure on mechanical ventilation, «the static compliance of the total respiratory system is conventionally obtained by dividing the tidal volume by the difference between the ‘plateau’ pressure measured at the airway opening (PaO) during an occlusion at end-inspiration and positive end-expiratory pressure (PEEP) set by the ventilator».[23]
| Measurement | Approximate value | |
| Male | Female | |
| Forced vital capacity (FVC) | 4.8 L | 3.7 L |
| Tidal volume (Vt) | 500 mL | 390 mL |
| Total lung capacity (TLC) | 6.0 L | 4.7 L |
Others[edit]
Forced Expiratory Time (FET)
Forced Expiratory Time (FET) measures the length of the expiration in seconds.
Slow vital capacity (SVC)
Slow vital capacity (SVC) is the maximum volume of air that can be exhaled slowly after slow maximum inhalation.
Maximal pressure (Pmax and Pi)
| Spirometer — ERV in cc (cm3) average Age 20 | |
| Male | Female |
| 4320 | 3387 |
Pmax is the asymptotically maximal pressure that can be developed by the respiratory muscles at any lung volume and Pi is the maximum inspiratory pressure that can be developed at specific lung volumes.[24] This measurement also requires pressure transducers in addition. It is considered normal if it is 60% to 140% of the average value in the population for any person of similar age, sex and body composition.[12] A derived parameter is the coefficient of retraction (CR) which is Pmax/TLC .[14]
Mean transit time (MTT)
Mean transit time is the area under the flow-volume curve divided by the forced vital capacity.[25]
Maximal inspiratory pressure (MIP)
MIP, also known as negative inspiratory force (NIF), is the maximum pressure that can be generated against an occluded airway beginning at functional residual capacity (FRC). It is a marker of respiratory muscle function and strength.[26] Represented by centimeters of water pressure (cmH2O) and measured with a manometer. Maximum inspiratory pressure is an important and noninvasive index of diaphragm strength and an independent tool for diagnosing many illnesses.[27] Typical maximum inspiratory pressures in adult males can be estimated from the equation, MIP = 142 — (1.03 x Age) cmH2O, where age is in years.[28]
Technologies used in spirometers[edit]
- Volumetric Spirometers
- Water bell
- Bellows wedge
- Flow measuring Spirometers
- Fleisch-pneumotach
- Lilly (screen) pneumotach
- Turbine/Stator Rotor (normally incorrectly referred to as a turbine. Actually a rotating vane which spins because of the air flow generated by the subject. The revolutions of the vane are counted as they break a light beam)
- Pitot tube
- Hot-wire anemometer
- Ultrasound
See also[edit]
- Peak flow meter
- Nitrogen washout
References[edit]
- ^ «Spirometry». National Institute for Occupational Safety and Health (NIOSH). Retrieved 31 January 2017.
- ^ American Academy of Allergy, Asthma, and Immunology. «Five Things Physicians and Patients Should Question» (PDF). Choosing Wisely: an initiative of the ABIM Foundation. American Academy of Allergy, Asthma, and Immunology. Retrieved 14 August 2012.
{{cite web}}: CS1 maint: multiple names: authors list (link) - ^ Expert Panel Report 3: Guidelines for the Diagnosis and Management of Asthma (PDF) (NIH Publication Number 08-5846 ed.). National Institutes of Health. 2007.
- ^ Bateman, E. D.; Hurd, S. S.; Barnes, P. J.; Bousquet, J.; Drazen, J. M.; Fitzgerald, M.; Gibson, P.; Ohta, K.; O’Byrne, P.; Pedersen, S. E.; Pizzichini, E.; Sullivan, S. D.; Wenzel, S. E.; Zar, H. J. (2008). «Global strategy for asthma management and prevention: GINA executive summary». European Respiratory Journal. 31 (1): 143–178. doi:10.1183/09031936.00138707. PMID 18166595. S2CID 206960094.
- ^ a b c d e f g h Pierce, R. (2005). «Spirometry: An essential clinical measurement». Australian Family Physician. 34 (7): 535–539. PMID 15999163.
- ^ Clark, Margaret Varnell (2010). Asthma: A Clinician’s Guide (ist ed.). Burlington, Ma.: Jones & Bartlett Learning. p. 46. ISBN 978-0763778545.
- ^ «Spirometry». Cleveland Clinic. Retrieved 13 September 2020.
- ^ surgeryencyclopedia.com > Spirometry tests. Retrieved 14 March 2010.
- ^ MVV and MBC
- ^ Stanojevic S, Wade A, Stocks J, et al. (February 2008). «Reference Ranges for Spirometry Across All Ages: A New Approach». Am. J. Respir. Crit. Care Med. 177 (3): 253–60. doi:10.1164/rccm.200708-1248OC. PMC 2643211. PMID 18006882.
- ^ a b Perez, LL (March–April 2013). «Office spirometry». Osteopathic Family Physician. 5 (2): 65–69. doi:10.1016/j.osfp.2012.09.003.
- ^ a b c d LUNGFUNKTION — Practice compendium for semester 6. Department of Medical Sciences, Clinical Physiology, Academic Hospital, Uppsala, Sweden. Retrieved 2010.
- ^ Clinic, the Cleveland (2010). Current clinical medicine 2010 (2nd ed.). Philadelphia, Pa.: Saunders. p. 8. ISBN 978-1416066439.
- ^ a b c Interpretation model — compendium at Uppsala Academic Hospital. By H. Hedenström. 2009-02-04
- ^ Simon, Michael R.; Chinchilli, Vernon M.; Phillips, Brenda R.; Sorkness, Christine A.; Lemanske Jr., Robert F.; Szefler, Stanley J.; Taussig, Lynn; Bacharier, Leonard B.; Morgan, Wayne (1 September 2010). «Forced expiratory flow between 25% and 75% of vital capacity and FEV1/forced vital capacity ratio in relation to clinical and physiological parameters in asthmatic children with normal FEV1 values». Journal of Allergy and Clinical Immunology. 126 (3): 527–534.e8. doi:10.1016/j.jaci.2010.05.016. PMC 2933964. PMID 20638110.
- ^ Ciprandi, Giorgio; Cirillo, Ignazio (1 February 2011). «Forced expiratory flow between 25% and 75% of vital capacity may be a marker of bronchial impairment in allergic rhinitis». Journal of Allergy and Clinical Immunology. 127 (2): 549, discussion 550–1. doi:10.1016/j.jaci.2010.10.053. PMID 21281879.
- ^ Pellegrino R, Viegi G, Brusasco V, Crapo RO, Burgos F, Casaburi R, Coates A, van der Grinten CP, Gustafsson P, Hankinson J, Jensen R, Johnson DC, MacIntyre N, McKay R, Miller MR, Navajas D, Pedersen OF, Wanger J (November 2005). «Interpretative strategies for lung function tests». The European Respiratory Journal. 26 (5): 948–68. doi:10.1183/09031936.05.00035205. PMID 16264058. S2CID 2741306.
- ^ Kreider, Maryl. «Chapter 14.1 Pulmonary Function Testing». ACP Medicine. Decker Intellectual Properties. Retrieved 29 April 2011.
- ^ Nunn AJ, Gregg I (April 1989). «New regression equations for predicting peak expiratory flow in adults». BMJ. 298 (6680): 1068–70. doi:10.1136/bmj.298.6680.1068. PMC 1836460. PMID 2497892. Adapted by Clement Clarke for use in EU scale — see Peakflow.com ⇒ Predictive Normal Values (Nomogram, EU scale)
- ^ MedlinePlus Encyclopedia: Lung diffusion testing
- ^ George, Ronald B. (2005). Chest medicine: essentials of pulmonary and critical care medicine. Lippincott Williams & Wilkins. p. 96. ISBN 978-0-7817-5273-2.
- ^ Sud, A.; Gupta, D.; Wanchu, A.; Jindal, S. K.; Bambery, P. (2001). «Static lung compliance as an index of early pulmonary disease in systemic sclerosis». Clinical Rheumatology. 20 (3): 177–180. doi:10.1007/s100670170060. PMID 11434468. S2CID 19170708.
- ^ Rossi A, Gottfried SB, Zocchi L, et al. (May 1985). «Measurement of static compliance of the total respiratory system in patients with acute respiratory failure during mechanical ventilation. The effect of intrinsic positive end-expiratory pressure». The American Review of Respiratory Disease. 131 (5): 672–7. doi:10.1164/arrd.1985.131.5.672 (inactive 31 December 2022). PMID 4003913.
{{cite journal}}: CS1 maint: DOI inactive as of December 2022 (link) - ^ Lausted, C.; Johnson, A.; Scott, W.; Johnson, M.; Coyne, K.; Coursey, D. (2006). «Maximum static inspiratory and expiratory pressures with different lung volumes». BioMedical Engineering OnLine. 5 (1): 29. doi:10.1186/1475-925X-5-29. PMC 1501025. PMID 16677384. [1]
- ^ Borth, F. M. (1982). «The derivation of an index of ventilatory function from spirometric recordings using canonical analysis». British Journal of Diseases of the Chest. 76 (4): 400–756. doi:10.1016/0007-0971(82)90077-8. PMID 7150499.
- ^ Page 352 in: Irwin, Richard (2008). Procedures, techniques, and minimally invasive monitoring in intensive care medicine. Philadelphia: Wolters Kluwer Health/Lippincott Williams & Wilkins. ISBN 978-0781778626.
- ^ Sachs MC, Enright PL, Hinckley Stukovsky KD, Jiang R, Barr RG, Multi-Ethnic Study of Atherosclerosis Lung Study (2009). «Performance of maximum inspiratory pressure tests and maximum inspiratory pressure reference equations for 4 race/ethnic groups». Respir Care. 54 (10): 1321–8. PMC 3616895. PMID 19796411.
{{cite journal}}: CS1 maint: multiple names: authors list (link) - ^ Wilson SH, Cooke NT, Edwards RH, Spiro SG (July 1984). «Predicted normal values for maximal respiratory pressures in caucasian adults and children». Thorax. 39 (7): 535–8. doi:10.1136/thx.39.7.535. PMC 459855. PMID 6463933.
Further reading[edit]
- Miller MR, Crapo R, Hankinson J, Brusasco V, Burgos F, Casaburi R, Coates A, Enright P, van der Grinten CP, Gustafsson P, Jensen R, Johnson DC, MacIntyre N, McKay R, Navajas D, Pedersen OF, Pellegrino R, Viegi G, Wanger J (July 2005). «General considerations for lung function testing». European Respiratory Journal. 26 (1): 153–161. doi:10.1183/09031936.05.00034505. PMID 15994402. S2CID 5626417.
External links[edit]
![]()
Wikimedia Commons has media related to Spirometry.
- American Thoracic Society (ATS)
- European Respiratory Society (ERS)
| Spirometry | |
|---|---|
|
Flow-Volume loop showing successful FVC maneuver. Positive values represent expiration, negative values represent inspiration. At the start of the test both flow and volume are equal to zero (representing the volume in the spirometer rather than the lung). The trace moves clockwise for expiration followed by inspiration. After the starting point the curve rapidly mounts to a peak (the peak expiratory flow). (Note the FEV1 value is arbitrary in this graph and just shown for illustrative purposes; these values must be calculated as part of the procedure). |
|
| MeSH | D013147 |
| OPS-301 code | 1-712 |
|
|
| TLC | Total lung capacity: the volume in the lungs at maximal inflation, the sum of VC and RV. |
|---|---|
| TV | Tidal volume: that volume of air moved into or out of the lungs during quiet breathing (TV indicates a subdivision of the lung; when tidal volume is precisely measured, as in gas exchange calculation, the symbol TV or VT is used.) |
| RV | Residual volume: the volume of air remaining in the lungs after a maximal exhalation |
| ERV | Expiratory reserve volume: the maximal volume of air that can be exhaled from the end-expiratory position |
| IRV | Inspiratory reserve volume: the maximal volume that can be inhaled from the end-inspiratory level |
| IC | Inspiratory capacity: the sum of IRV and TV |
| IVC | Inspiratory vital capacity: the maximum volume of air inhaled from the point of maximum expiration |
| VC | Vital capacity: the volume of air breathed out after the deepest inhalation. |
| VT | Tidal volume: that volume of air moved into or out of the lungs during quiet breathing (VT indicates a subdivision of the lung; when tidal volume is precisely measured, as in gas exchange calculation, the symbol TV or VT is used.) |
| FRC | Functional residual capacity: the volume in the lungs at the end-expiratory position |
| RV/TLC% | Residual volume expressed as percent of TLC |
| VA | Alveolar gas volume |
| VL | Actual volume of the lung including the volume of the conducting airway. |
| FVC | Forced vital capacity: the determination of the vital capacity from a maximally forced expiratory effort |
| FEVt | Forced expiratory volume (time): a generic term indicating the volume of air exhaled under forced conditions in the first t seconds |
| FEV1 | Volume that has been exhaled at the end of the first second of forced expiration |
| FEFx | Forced expiratory flow related to some portion of the FVC curve; modifiers refer to amount of FVC already exhaled |
| FEFmax | The maximum instantaneous flow achieved during a FVC maneuver |
| FIF | Forced inspiratory flow: (Specific measurement of the forced inspiratory curve is denoted by nomenclature analogous to that for the forced expiratory curve. For example, maximum inspiratory flow is denoted FIFmax. Unless otherwise specified, volume qualifiers indicate the volume inspired from RV at the point of measurement.) |
| PEF | Peak expiratory flow: The highest forced expiratory flow measured with a peak flow meter |
| MVV | Maximal voluntary ventilation: volume of air expired in a specified period during repetitive maximal effort |
|
Spirometry (meaning the measuring of breath) is the most common of the pulmonary function tests (PFTs). It measures lung function, specifically the amount (volume) and/or speed (flow) of air that can be inhaled and exhaled. Spirometry is helpful in assessing breathing patterns that identify conditions such as asthma, pulmonary fibrosis, cystic fibrosis, and COPD. It is also helpful as part of a system of health surveillance, in which breathing patterns are measured over time.[1]
Spirometry generates pneumotachographs, which are charts that plot the volume and flow of air coming in and out of the lungs from one inhalation and one exhalation.
Indications[edit]
Spirometry is indicated for the following reasons:
- to diagnose or manage asthma[2][3][4]
- to detect respiratory disease in patients presenting with symptoms of breathlessness, and to distinguish respiratory from cardiac disease as the cause[5]
- to measure bronchial responsiveness in patients suspected of having asthma[5]
- to diagnose and differentiate between obstructive lung disease and restrictive lung disease[5]
- to follow the natural history of disease in respiratory conditions[5]
- to assess of impairment from occupational asthma[5]
- to identify those at risk from pulmonary barotrauma while scuba diving[5]
- to conduct pre-operative risk assessment before anaesthesia or cardiothoracic surgery[5]
- to measure response to treatment of conditions which spirometry detects[5]
- to diagnose the vocal cord dysfunction.
Contraindications[edit]
Forced expiratory maneuvers may aggravate some medical conditions.[6] Spirometry should not be performed when the individual presents with:
- Hemoptysis of unknown origin
- Pneumothorax
- Unstable cardiovascular status (angina, recent myocardial infarction, etc.)
- Thoracic, abdominal, or cerebral aneurysms
- Cataracts or recent eye surgery
- Recent thoracic or abdominal surgery
- Nausea, vomiting, or acute illness
- Recent or current viral infection
- Undiagnosed hypertension
Spirometry testing[edit]
A modern USB PC-based spirometer.
Device for spirometry. The patient places his or her lips around the blue mouthpiece. The teeth go between the nubs and the shield, and the lips go over the shield. A noseclip guarantees that breath will flow only through the mouth.
Screen for spirometry readouts at right. The chamber can also be used for body plethysmography.
Spirometer[edit]
The spirometry test is performed using a device called a spirometer,[7] which comes in several different varieties. Most spirometers display the following graphs, called spirograms:
- a volume-time curve, showing volume (litres) along the Y-axis and time (seconds) along the X-axis
- a flow-volume loop, which graphically depicts the rate of airflow on the Y-axis and the total volume inspired or expired on the X-axis
Procedure[edit]
The basic forced volume vital capacity (FVC) test varies slightly depending on the equipment used, either closed circuit or open circuit, but should follow the ATS/ERS Standardisation of Spirometry.
Generally, the patient is asked to take the deepest breath they can, and then exhale into the sensor as hard as possible, for as long as possible, preferably at least 6 seconds. It is sometimes directly followed by a rapid inspiration, (inhalation) in particular when assessing possible upper airway obstruction. Sometimes, the test will be preceded by a period of quiet breathing in and out from the sensor (tidal volume), or the rapid breath in (forced inspiratory part) will come before the forced expiration.
During the test, soft nose clips may be used to prevent air escaping through the nose. Filter mouthpieces may be used to prevent the spread of microorganisms.
Limitations of test[edit]
The maneuver is highly dependent on patient cooperation and effort, and is normally repeated at least three times to ensure reproducibility. Since results are dependent on patient cooperation, FVC can only be underestimated, never overestimated.
Due to the patient cooperation required, spirometry can only be used on children old enough to comprehend and follow the instructions given (6 years old or more), and only on patients who are able to understand and follow instructions — thus, this test is not suitable for patients who are unconscious, heavily sedated, or have limitations that would interfere with vigorous respiratory efforts. Other types of lung function tests are available for infants and unconscious persons.
Another major limitation is the fact that many intermittent or mild asthmatics have normal spirometry between acute exacerbation, limiting spirometry’s usefulness as a diagnostic. It is more useful as a monitoring tool: a sudden decrease in FEV1 or other spirometric measure in the same patient can signal worsening control, even if the raw value is still normal. Patients are encouraged to record their personal best measures.
Example of a modern PC-based spirometer printout.
[edit]
Spirometry can also be part of a bronchial challenge test, used to determine bronchial hyperresponsiveness to either rigorous exercise, inhalation of cold/dry air, or with a pharmaceutical agent such as methacholine or histamine.
Sometimes, to assess the reversibility of a particular condition, a bronchodilator is administered before performing another round of tests for comparison. This is commonly referred to as a reversibility test, or a post bronchodilator test (Post BD), and is an important part in diagnosing asthma versus COPD.
Other complementary lung functions tests include plethysmography and nitrogen washout.
Parameters[edit]
The most common parameters measured in spirometry are Vital capacity (VC), Forced vital capacity (FVC), Forced expiratory volume (FEV) at timed intervals of 0.5, 1.0 (FEV1), 2.0, and 3.0 seconds, forced expiratory flow 25–75% (FEF 25–75) and maximal voluntary ventilation (MVV),[8] also known as Maximum breathing capacity.[9] Other tests may be performed in certain situations.
Results are usually given in both raw data (litres, litres per second) and percent predicted—the test result as a percent of the «predicted values» for the patients of similar characteristics (height, age, sex, and sometimes race and weight). The interpretation of the results can vary depending on the physician and the source of the predicted values. Generally speaking, results nearest to 100% predicted are the most normal, and results over 80% are often considered normal. Multiple publications of predicted values have been published and may be calculated based on age, sex, weight and ethnicity. However, review by a doctor is necessary for accurate diagnosis of any individual situation.
A bronchodilator is also given in certain circumstances and a pre/post graph comparison is done to assess the effectiveness of the bronchodilator. See the example printout.
Functional residual capacity (FRC) cannot be measured via spirometry, but it can be measured with a plethysmograph or dilution tests (for example, helium dilution test).
Average values for forced vital capacity (FVC), forced expiratory volume in 1 second (FEV1) and forced expiratory flow 25–75% (FEF25–75%), according to a study in the United States 2007 of 3,600 subjects aged 4–80 years.[10] Y-axis is expressed in litres for FVC and FEV1, and in litres/second for FEF25–75%.
Forced vital capacity (FVC)[edit]
Forced vital capacity (FVC) is the volume of air that can forcibly be blown out after full inspiration,[11] measured in liters. FVC is the most basic maneuver in spirometry tests.
Forced expiratory volume in 1 second (FEV1)[edit]
FEV1 is the volume of air that can forcibly be blown out in first 1-second, after full inspiration.[11] Average values for FEV1 in healthy people depend mainly on sex and age, according to the diagram.
Values of between 80% and 120% of the average value are considered normal.[12] Predicted normal values for FEV1 can be calculated and depend on age, sex, height, mass and ethnicity as well as the research study that they are based on.
FEV1/FVC ratio[edit]
FEV1/FVC is the ratio of FEV1 to FVC. In healthy adults this should be approximately 70–80% (declining with age).[13] In obstructive diseases (asthma, COPD, chronic bronchitis, emphysema) FEV1 is diminished because of increased airway resistance to expiratory flow; the FVC may be decreased as well, due to the premature closure of airway in expiration, just not in the same proportion as FEV1 (for instance, both FEV1 and FVC are reduced, but the former is more affected because of the increased airway resistance). This generates a reduced value (<70%, often ~45%). In restrictive diseases (such as pulmonary fibrosis) the FEV1 and FVC are both reduced proportionally and the value may be normal or even increased as a result of decreased lung compliance.
A derived value of FEV1 is FEV1% predicted (FEV1%), which is defined as FEV1 of the patient divided by the average FEV1 in the population for any person of the same age, height, gender, and race.[medical citation needed]
Forced expiratory flow (FEF)[edit]
Forced expiratory flow (FEF) is the flow (or speed) of air coming out of the lung during the middle portion of a forced expiration.
It can be given at discrete times, generally defined by what fraction of the forced vital capacity (FVC) has been exhaled.
The usual discrete intervals are 25%, 50% and 75% (FEF25, FEF50 and FEF75), or 25% and 50% of FVC that has been exhaled.
It can also be given as a mean of the flow during an interval, also generally delimited by when specific fractions remain of FVC, usually 25–75% (FEF25–75%). Average ranges in the healthy population depend mainly on sex and age, with FEF25–75% shown in diagram at left. Values ranging from 50 to 60% and up to 130% of the average are considered normal.[12] Predicted normal values for FEF can be calculated and depend on age, sex, height, mass and ethnicity as well as the research study that they are based on.
MMEF or MEF stands for maximal (mid-)expiratory flow and is the peak of expiratory flow as taken from the flow-volume curve and measured in liters per second. It should theoretically be identical to peak expiratory flow (PEF), which is, however, generally measured by a peak flow meter and given in liters per minute.[14]
Recent research suggests that FEF25-75% or FEF25-50% may be a more sensitive parameter than FEV1 in the detection of obstructive small airway disease.[15][16] However, in the absence of concomitant changes in the standard markers, discrepancies in mid-range expiratory flow may not be specific enough to be useful, and current practice guidelines recommend continuing to use FEV1, VC, and FEV1/VC as indicators of obstructive disease.[17][18]
More rarely, forced expiratory flow may be given at intervals defined by how much remains of total lung capacity. In such cases, it is usually designated as e.g. FEF70%TLC, FEF60%TLC and FEF50%TLC.[14]
Forced inspiratory flow 25–75% or 25–50%[edit]
Forced inspiratory flow 25–75% or 25–50% (FIF 25–75% or 25–50%) is similar to FEF 25–75% or 25–50% except the measurement is taken during inspiration.[medical citation needed]
Peak expiratory flow (PEF)[edit]
Normal values for peak expiratory flow (PEF), shown on EU scale.[19]
Peak expiratory flow (PEF) is the maximal flow (or speed) achieved during the maximally forced expiration initiated at full inspiration, measured in liters per minute or in liters per second.
Tidal volume (TV)[edit]
Tidal volume is the amount of air inhaled or exhaled normally at rest.[medical citation needed]
Total lung capacity (TLC)[edit]
Total lung capacity (TLC) is the maximum volume of air present in the lungs.[medical citation needed]
Diffusing capacity (DLCO)[edit]
Diffusing capacity (or DLCO) is the carbon monoxide uptake from a single inspiration in a standard time (usually 10 seconds). During the test the person inhales a test gas mixture that consisting of regular air that includes an inert tracer gas and CO, less than one percent. Since hemoglobin has a greater affinity to CO than oxygen the breath-hold time can be only 10 seconds, which is a sufficient amount of time for this transfer of CO to occur. Since the inhaled amount of CO is known, the exhaled CO is subtracted to determine the amount transferred during the breath-hold time. The tracer gas is analyzed simultaneously with CO to determine the distribution of the test gas mixture. This test will pick up diffusion impairments, for instance in pulmonary fibrosis.[20] This must be corrected for anemia (a low hemoglobin concentration will reduce DLCO) and pulmonary hemorrhage (excess RBC’s in the interstitium or alveoli can absorb CO and artificially increase the DLCO capacity). Atmospheric pressure and/or altitude will also affect measured DLCO, and so a correction factor is needed to adjust for standard pressure.
Maximum voluntary ventilation (MVV)[edit]
Maximum voluntary ventilation (MVV) is a measure of the maximum amount of air that can be inhaled and exhaled within one minute. For the comfort of the patient this is done over a 15-second time period before being extrapolated to a value for one minute expressed as liters/minute. Average values for males and females are 140–180 and 80–120 liters per minute respectively.[medical citation needed]
Static lung compliance (Cst)[edit]
When estimating static lung compliance, volume measurements by the spirometer needs to be complemented by pressure transducers in order to simultaneously measure the transpulmonary pressure. When having drawn a curve with the relations between changes in volume to changes in transpulmonary pressure, Cst is the slope of the curve during any given volume, or, mathematically, ΔV/ΔP.[21] Static lung compliance is perhaps the most sensitive parameter for the detection of abnormal pulmonary mechanics.[22] It is considered normal if it is 60% to 140% of the average value in the population for any person of similar age, sex and body composition.[12]
In those with acute respiratory failure on mechanical ventilation, «the static compliance of the total respiratory system is conventionally obtained by dividing the tidal volume by the difference between the ‘plateau’ pressure measured at the airway opening (PaO) during an occlusion at end-inspiration and positive end-expiratory pressure (PEEP) set by the ventilator».[23]
| Measurement | Approximate value | |
| Male | Female | |
| Forced vital capacity (FVC) | 4.8 L | 3.7 L |
| Tidal volume (Vt) | 500 mL | 390 mL |
| Total lung capacity (TLC) | 6.0 L | 4.7 L |
Others[edit]
Forced Expiratory Time (FET)
Forced Expiratory Time (FET) measures the length of the expiration in seconds.
Slow vital capacity (SVC)
Slow vital capacity (SVC) is the maximum volume of air that can be exhaled slowly after slow maximum inhalation.
Maximal pressure (Pmax and Pi)
| Spirometer — ERV in cc (cm3) average Age 20 | |
| Male | Female |
| 4320 | 3387 |
Pmax is the asymptotically maximal pressure that can be developed by the respiratory muscles at any lung volume and Pi is the maximum inspiratory pressure that can be developed at specific lung volumes.[24] This measurement also requires pressure transducers in addition. It is considered normal if it is 60% to 140% of the average value in the population for any person of similar age, sex and body composition.[12] A derived parameter is the coefficient of retraction (CR) which is Pmax/TLC .[14]
Mean transit time (MTT)
Mean transit time is the area under the flow-volume curve divided by the forced vital capacity.[25]
Maximal inspiratory pressure (MIP)
MIP, also known as negative inspiratory force (NIF), is the maximum pressure that can be generated against an occluded airway beginning at functional residual capacity (FRC). It is a marker of respiratory muscle function and strength.[26] Represented by centimeters of water pressure (cmH2O) and measured with a manometer. Maximum inspiratory pressure is an important and noninvasive index of diaphragm strength and an independent tool for diagnosing many illnesses.[27] Typical maximum inspiratory pressures in adult males can be estimated from the equation, MIP = 142 — (1.03 x Age) cmH2O, where age is in years.[28]
Technologies used in spirometers[edit]
- Volumetric Spirometers
- Water bell
- Bellows wedge
- Flow measuring Spirometers
- Fleisch-pneumotach
- Lilly (screen) pneumotach
- Turbine/Stator Rotor (normally incorrectly referred to as a turbine. Actually a rotating vane which spins because of the air flow generated by the subject. The revolutions of the vane are counted as they break a light beam)
- Pitot tube
- Hot-wire anemometer
- Ultrasound
See also[edit]
- Peak flow meter
- Nitrogen washout
References[edit]
- ^ «Spirometry». National Institute for Occupational Safety and Health (NIOSH). Retrieved 31 January 2017.
- ^ American Academy of Allergy, Asthma, and Immunology. «Five Things Physicians and Patients Should Question» (PDF). Choosing Wisely: an initiative of the ABIM Foundation. American Academy of Allergy, Asthma, and Immunology. Retrieved 14 August 2012.
{{cite web}}: CS1 maint: multiple names: authors list (link) - ^ Expert Panel Report 3: Guidelines for the Diagnosis and Management of Asthma (PDF) (NIH Publication Number 08-5846 ed.). National Institutes of Health. 2007.
- ^ Bateman, E. D.; Hurd, S. S.; Barnes, P. J.; Bousquet, J.; Drazen, J. M.; Fitzgerald, M.; Gibson, P.; Ohta, K.; O’Byrne, P.; Pedersen, S. E.; Pizzichini, E.; Sullivan, S. D.; Wenzel, S. E.; Zar, H. J. (2008). «Global strategy for asthma management and prevention: GINA executive summary». European Respiratory Journal. 31 (1): 143–178. doi:10.1183/09031936.00138707. PMID 18166595. S2CID 206960094.
- ^ a b c d e f g h Pierce, R. (2005). «Spirometry: An essential clinical measurement». Australian Family Physician. 34 (7): 535–539. PMID 15999163.
- ^ Clark, Margaret Varnell (2010). Asthma: A Clinician’s Guide (ist ed.). Burlington, Ma.: Jones & Bartlett Learning. p. 46. ISBN 978-0763778545.
- ^ «Spirometry». Cleveland Clinic. Retrieved 13 September 2020.
- ^ surgeryencyclopedia.com > Spirometry tests. Retrieved 14 March 2010.
- ^ MVV and MBC
- ^ Stanojevic S, Wade A, Stocks J, et al. (February 2008). «Reference Ranges for Spirometry Across All Ages: A New Approach». Am. J. Respir. Crit. Care Med. 177 (3): 253–60. doi:10.1164/rccm.200708-1248OC. PMC 2643211. PMID 18006882.
- ^ a b Perez, LL (March–April 2013). «Office spirometry». Osteopathic Family Physician. 5 (2): 65–69. doi:10.1016/j.osfp.2012.09.003.
- ^ a b c d LUNGFUNKTION — Practice compendium for semester 6. Department of Medical Sciences, Clinical Physiology, Academic Hospital, Uppsala, Sweden. Retrieved 2010.
- ^ Clinic, the Cleveland (2010). Current clinical medicine 2010 (2nd ed.). Philadelphia, Pa.: Saunders. p. 8. ISBN 978-1416066439.
- ^ a b c Interpretation model — compendium at Uppsala Academic Hospital. By H. Hedenström. 2009-02-04
- ^ Simon, Michael R.; Chinchilli, Vernon M.; Phillips, Brenda R.; Sorkness, Christine A.; Lemanske Jr., Robert F.; Szefler, Stanley J.; Taussig, Lynn; Bacharier, Leonard B.; Morgan, Wayne (1 September 2010). «Forced expiratory flow between 25% and 75% of vital capacity and FEV1/forced vital capacity ratio in relation to clinical and physiological parameters in asthmatic children with normal FEV1 values». Journal of Allergy and Clinical Immunology. 126 (3): 527–534.e8. doi:10.1016/j.jaci.2010.05.016. PMC 2933964. PMID 20638110.
- ^ Ciprandi, Giorgio; Cirillo, Ignazio (1 February 2011). «Forced expiratory flow between 25% and 75% of vital capacity may be a marker of bronchial impairment in allergic rhinitis». Journal of Allergy and Clinical Immunology. 127 (2): 549, discussion 550–1. doi:10.1016/j.jaci.2010.10.053. PMID 21281879.
- ^ Pellegrino R, Viegi G, Brusasco V, Crapo RO, Burgos F, Casaburi R, Coates A, van der Grinten CP, Gustafsson P, Hankinson J, Jensen R, Johnson DC, MacIntyre N, McKay R, Miller MR, Navajas D, Pedersen OF, Wanger J (November 2005). «Interpretative strategies for lung function tests». The European Respiratory Journal. 26 (5): 948–68. doi:10.1183/09031936.05.00035205. PMID 16264058. S2CID 2741306.
- ^ Kreider, Maryl. «Chapter 14.1 Pulmonary Function Testing». ACP Medicine. Decker Intellectual Properties. Retrieved 29 April 2011.
- ^ Nunn AJ, Gregg I (April 1989). «New regression equations for predicting peak expiratory flow in adults». BMJ. 298 (6680): 1068–70. doi:10.1136/bmj.298.6680.1068. PMC 1836460. PMID 2497892. Adapted by Clement Clarke for use in EU scale — see Peakflow.com ⇒ Predictive Normal Values (Nomogram, EU scale)
- ^ MedlinePlus Encyclopedia: Lung diffusion testing
- ^ George, Ronald B. (2005). Chest medicine: essentials of pulmonary and critical care medicine. Lippincott Williams & Wilkins. p. 96. ISBN 978-0-7817-5273-2.
- ^ Sud, A.; Gupta, D.; Wanchu, A.; Jindal, S. K.; Bambery, P. (2001). «Static lung compliance as an index of early pulmonary disease in systemic sclerosis». Clinical Rheumatology. 20 (3): 177–180. doi:10.1007/s100670170060. PMID 11434468. S2CID 19170708.
- ^ Rossi A, Gottfried SB, Zocchi L, et al. (May 1985). «Measurement of static compliance of the total respiratory system in patients with acute respiratory failure during mechanical ventilation. The effect of intrinsic positive end-expiratory pressure». The American Review of Respiratory Disease. 131 (5): 672–7. doi:10.1164/arrd.1985.131.5.672 (inactive 31 December 2022). PMID 4003913.
{{cite journal}}: CS1 maint: DOI inactive as of December 2022 (link) - ^ Lausted, C.; Johnson, A.; Scott, W.; Johnson, M.; Coyne, K.; Coursey, D. (2006). «Maximum static inspiratory and expiratory pressures with different lung volumes». BioMedical Engineering OnLine. 5 (1): 29. doi:10.1186/1475-925X-5-29. PMC 1501025. PMID 16677384. [1]
- ^ Borth, F. M. (1982). «The derivation of an index of ventilatory function from spirometric recordings using canonical analysis». British Journal of Diseases of the Chest. 76 (4): 400–756. doi:10.1016/0007-0971(82)90077-8. PMID 7150499.
- ^ Page 352 in: Irwin, Richard (2008). Procedures, techniques, and minimally invasive monitoring in intensive care medicine. Philadelphia: Wolters Kluwer Health/Lippincott Williams & Wilkins. ISBN 978-0781778626.
- ^ Sachs MC, Enright PL, Hinckley Stukovsky KD, Jiang R, Barr RG, Multi-Ethnic Study of Atherosclerosis Lung Study (2009). «Performance of maximum inspiratory pressure tests and maximum inspiratory pressure reference equations for 4 race/ethnic groups». Respir Care. 54 (10): 1321–8. PMC 3616895. PMID 19796411.
{{cite journal}}: CS1 maint: multiple names: authors list (link) - ^ Wilson SH, Cooke NT, Edwards RH, Spiro SG (July 1984). «Predicted normal values for maximal respiratory pressures in caucasian adults and children». Thorax. 39 (7): 535–8. doi:10.1136/thx.39.7.535. PMC 459855. PMID 6463933.
Further reading[edit]
- Miller MR, Crapo R, Hankinson J, Brusasco V, Burgos F, Casaburi R, Coates A, Enright P, van der Grinten CP, Gustafsson P, Jensen R, Johnson DC, MacIntyre N, McKay R, Navajas D, Pedersen OF, Pellegrino R, Viegi G, Wanger J (July 2005). «General considerations for lung function testing». European Respiratory Journal. 26 (1): 153–161. doi:10.1183/09031936.05.00034505. PMID 15994402. S2CID 5626417.
External links[edit]
![]()
Wikimedia Commons has media related to Spirometry.
- American Thoracic Society (ATS)
- European Respiratory Society (ERS)
спирометрия
- спирометрия
- спироме́трия, -и
Русское словесное ударение. — М.: ЭНАС.
.
2001.
Смотреть что такое «спирометрия» в других словарях:
-
спирометрия — спирометрия … Орфографический словарь-справочник
-
СПИРОМЕТРИЯ — СПИРОМЕТРИЯ, СПИРОМЕТР (от лат. spiro дую и греч. metron мера). Спирометр и я измерение количества воздуха, перемещаемого дыхательным аппаратом человека (см. Дыхание, дыхательный аппарат); спирометрия входит в комплекс антропометрических… … Большая медицинская энциклопедия
-
СПИРОМЕТРИЯ — (от лат. spiro дую дышу и …метрия), измерение жизненной емкости легких с помощью специального прибора спирометра … Большой Энциклопедический словарь
-
спирометрия — и; ж. [от лат. spirare дышать и и греч. metreō измеряю] Измерение жизненной ёмкости лёгких с помощью спирометра. * * * спирометрия (от лат. spiro дую, дышу и …метрия), измерение жизненной ёмкости лёгких с помощью специального прибора … … Энциклопедический словарь
-
Спирометрия — Портативный спирометр Cпирометрия, метод исследования функции внешнего дыхания, включающий в себя измерение объёмных и скоростных показателей дыхания. Выполняются следующие виды спирометрических пр … Википедия
-
спирометрия — (лат. spirare дышать, выдыхать + …метрия) метод исследования жизненной емкости легких измерением объема выдыхаемого воздуха с помощью прибора спирометра. Новый словарь иностранных слов. by EdwART, , 2009. спирометрия и, мн. нет, ж. ( … Словарь иностранных слов русского языка
-
спирометрия — rus спирометрия (ж) eng spirometry fra spirométrie (f) deu Spirometrie (f) spa espirometría (f) … Безопасность и гигиена труда. Перевод на английский, французский, немецкий, испанский языки
-
спирометрия — spirometrija statusas T sritis Standartizacija ir metrologija apibrėžtis Plaučių įkvepiamo ir iškvepiamo oro tūrio matavimas. atitikmenys: angl. spirometry vok. Spirometrie, f rus. спирометрия, f pranc. spirométrie, f … Penkiakalbis aiškinamasis metrologijos terminų žodynas
-
спирометрия — spirometrija statusas T sritis Kūno kultūra ir sportas apibrėžtis Gyvybinės plaučių talpos matavimas specialiu prietaisu – spirometru. kilmė lot. spiro – kvėpuoju + gr. metreō – matuoju atitikmenys: angl. spirometry vok. Spirometrie, f rus.… … Sporto terminų žodynas
-
спирометрия — (спиро + греч. metreo измерять) измерение жизненной емкости легких и других легочных объемов при помощи спирометра … Большой медицинский словарь
-
Спирометрия — (от лат. spiro дую, дышу и …метрия (См. …метрия)) метод измерения жизненной ёмкости лёгких. С. предложена в 1846 английским учёным Дж. Хатчисоном. Жизненная ёмкость (см. Лёгочные объёмы) складывается из дыхательного воздуха,… … Большая советская энциклопедия
Общие сведения
В медицине известны различные методы исследования функции внешнего дыхания. Такие исследования играют большую роль при комплексном обследовании пациентов с заболеваниями бронхов и легких. Благодаря им можно определить наличие дыхательной недостаточности у больного задолго до проявления первых клинических симптомов. Современная медицина позволяет выявить характер, тип, степень выраженности и динамику развития тех или иных патологических изменений, проследить эффективность лечения.
Что такое спирография и как ее проводят? Спирография (спирометрия) — это метод определения функции внешнего дыхания, основной способ диагностики и оценки функционального состояния легких. Метод широко применяется в пульмонологии и терапии, считается наиболее информативным.
Что показывает?
Что такое спирометрия в медицине и что это исследование показывает? Во время проведения обследования врач определяет следующие показатели:
- объем вдыхаемого и выдыхаемого воздуха – дыхательный объем легких;
- жизненную емкость легких – максимальное кол-во воздуха, который пациент может глубоко вдохнуть;
- форсированную жизненную емкость легких – разницу объемов в самом начале и в конце полного выдоха;
- функциональную остаточную емкость – оставшийся воздух после спокойного выдоха;
- остаточный объем после максимального выдоха;
- общую емкость;
- объем форсированного выдоха за первую секунду форсированного выдоха;
- пиковую объемную скорость;
- мгновенную объемную скорость;
- минутный объем дыхания;
- максимальную вентиляцию легких.
С помощью спирографа удается получить наиболее достоверные и информативные результаты и соответственно провести точную диагностику.
При проведении компьютерной спирометрии можно выявить:
- нарушения проходимости дыхательных путей;
- степень тяжести того или иного заболевания;
- симптомы ХОБЛ и бронхиальной астмы;
- скрытый спазм бронхов;
- оптимальную тактику лечения;
- эффективность текущей терапии в динамике.
Классификация
Существуют разные виды исследования:
- при спокойном дыхании для определения жизненной емкости легких;
- для определения максимальной вентиляции;
- при форсированном выдохе;
- функциональные пробы (спирография с бронхолитиком, провокационные пробы и другие).
Показания
Данный метод активно применяется в терапии и пульмонологии по следующим показаниям:
- долго не проходящий, затяжной кашель без причины, на протяжении 3-4 недель и более, часто – после простуды, ОРВИ или бронхита;
- чувство давления и «заложенности» в грудной клетке, одышка;
- если пациенту сложно делать вдох и выдох;
- «свистящее» или «сипящее» дыхание при вдохе;
- многолетний стаж курения;
- пациент страдает от частых обострений бронхита, одышки, ему не хватает воздуха;
- при отягощенной наследственности, если есть родственники с заболеваниями дыхательной системы и аллергическими заболеваниями;
- необходимо скорректировать лечение бронхиальной астмы;
- работа на вредном производстве.
Важные данные для разработки дальнейшей тактики лечения можно получить, если пройти спирограмму при бронхиальной астме, хронической обструктивной болезни легких, после и во время проведения разных медицинских мероприятий.
Противопоказания
Список противопоказаний к данному исследованию достаточно небольшой. Но, тем не менее, спирографию не следует проводить:
- после перенесенного недавно инфаркта, инсульта;
- при аневризме аорты, гипертонии;
- пациентам с пневмотораксом, при кровотечении;
- если пациент недавно перенес хирургическое вмешательство на грудной или брюшной полости;
- при острой сердечной недостаточности.
Спирометрия внесена в список обязательных профилактических обследований, которые должны проводиться ежегодно.
Подготовка к исследованию
На результаты могут существенно повлиять некоторые факторы, которые нельзя не учитывать.
 Обследование проводят с утра, натощак. После последнего приема пищи должно пройти минимум 6-8 часов. Допустимо выпить немного теплой воды и съесть один легкий крекер. В день исследования нельзя курить, пить крепкий чай или кофе.
Обследование проводят с утра, натощак. После последнего приема пищи должно пройти минимум 6-8 часов. Допустимо выпить немного теплой воды и съесть один легкий крекер. В день исследования нельзя курить, пить крепкий чай или кофе.
Перед началом не рекомендуется проводить лечебные процедуры, утреннюю гимнастику. Одежду на прием лучше надеть свободную, не стесняющую грудную клетку. Перед спирометрией лучше спокойной посидеть в течение 20 минут.
Также следует сделать перерыв в приеме некоторых лекарственных средств. Например, бронхолитических препаратов:
- Сальбутамола, Беродуала, Вентолина — за 6 часов;
- Серетида, Симбикорта, Фостера, Серевента, Форадила и препарата Оксис — за 12 часов;
- пролонгированных теофиллинов (Спирива) – за сутки.
Диета перед спирометрией
Перед спирографией не рекомендуется есть тяжелую пищу, пить кофе, чай, энергетические напитки, алкоголь. Обследование проводится утром натощак.
Как проводится спирометрия
До того, как широкое распространение приобрела цифровая техника, врачи использовали механические спирометры, обычно – водяные. В аппарате для исследования выдыхаемый пациентом воздух проникал в цилиндр, расположенный в сосуде с водой. Во время выдоха цилиндр двигался вверх и записывающее устройство, с ним соединенное, оставляло на движущейся бумаге график. График отражал изменение объема со временем. К сожалению, обследования на такого вида приборах были достаточно трудоемкими и предполагали дополнительный ручной расчет необходимых параметров.

Разновидности современных цифровых спирометров
Сейчас широкое применение имеют цифровые аппараты для исследования дыхательной функции – цифровые спирометры, спирографы. Аппарат фиксирует данные пациента в режиме спокойного дыхания, максимальной вентиляции легких и форсированного выдоха. Также проводят разные функциональные пробы, с бронходилататорами, провокационные и так далее.
Как проводится спирография? Врач или специалист, проводящий исследование обычно использует дополнительные программы, облегчающие расчёт необходимых параметров. Могут понадобиться данные о весе, росте и возрасте пациента, сопутствующих хронических заболеваниях и принимаемых препаратах.
После самой спирометрии рассчитывается таблица с индивидуальными показателями для пациента, значениями необходимых параметров и графическим изображением воздушного потока — спирограмма. При нарушениях в спирограмме врач может назначить дополнительные обследования. Например, с применением бронхолитиков. Процедура достаточно комфортная и безболезненная.
Методика проведения:
- пациент, плотно прижав губы к мундштуку спирографа, спокойно дышит в течение 10 секунд;
- врач командует, когда нужно максимально глубоко вдохнуть, чтобы легкие максимально заполнились воздухом;
- пациент делает выдох максимальной силы в трубку датчика.
У детей
Данную процедуру можно проводить у детей, начиная с 5-летнего возраста. Обычно исследование не вызывает никаких проблем и детям не требуется специальной подготовки. Чаще всего процедура проводится в игровой форме.
Расшифровка результатов спирографии
Расшифровкой результатов спирометрии занимается врач, он же ставит диагноз, дает рекомендации по поводу лечения и дальнейших обследований.
Во время расшифровки спирограммы легких специалист определяет ключевые значения, необходимые для постановки диагноза. На графике ниже изображена спирограмма форсированного выдоха с ключевыми параметрами:
- ФЖЕЛ – форсированная жизненная емкость легких;
- ОФВ1 – объем форсированного выдоха за 1 секунду;
- СОС25-75 – средняя скорость форсированного экспираторного потока, соответствующая 25 — 75% ФЖЕЛ.

Спирограмма форсированного выдоха
Некоторые показатели нормы спирометрии:
- ЧД — частота дыхательных движений, которые пациент совершил в течение минуты. В норме – от 16 до 18 единиц.
- МОД — объем дыхания в минуту. Весь воздух, которые прошел через легкие пациента в течение минуты. Зависит от множества факторов.
- ДО — дыхательный объем. Вся воздушная масса, попадающая в легочную ткань во время одного обычного вдоха. В норме – от 500 до 800 мл.
- СОС — средняя объемная скорость. Скорость форсированного выдоха в середине дыхательного движения. С ее помощью определяют обструктивные патологии.
Ниже приведена таблица нормальных показателей спирометрии. Следует отметить, что оценка результатов данного функционального исследования проводится специалистом и должна содержать точные данные, быть краткой и информативной. Кроме обычной констатации фактов, что те или иные показатели находятся в норме, а эти – нет, в результате исследования должны учитываться принципы клинического принятия решения, где вероятность заболевания после проведенного исследования рассчитывается с учетом вероятности заболевания до проведения исследования. Также учитывается качество проведенной процедуры, вероятность ложно-отрицательной и –положительной интерпретации, точность результатов и ключевых значений.
| Параметры | Обозначения | Нормальное значение | Единицы | |
| Мужчины | Женщины | |||
| Общая емкость легких | TLC | 7,0 | 6,2 | л |
| Жизненная емкость легких | VC | 5,6 | 5,0 | л |
| Форсированная жизненная емкость легких | FVC | 5,6 | 5,0 | л |
| Остаточный объем | RV | 1,4 | 1,2 | л |
| Функциональная остаточная емкость | FRC | 3,2 | 2,8 | л |
| Односекундная емкость | FEV1 | 4,5 | 4,0 | л |
| Максимальные экспираторные силы дыхательного потока | V*Emax | 10 | л/с | |
| Значение дыхательной границы (при частоте в 1/за мин) | 110 | 100 | л/мин | |
| Compliance дыхательного аппарата (легкие + грудная клетка) | CTl+Th | 1,3 | л/к Па-1 | |
| Compliance грудной клетки | CTh | 2,6 | л/к Па-1 | |
| Compliance легких | CTl | 2,6 | л/к Па-1 | |
| Сопротивление дыхательных путей | RL | 0,13 | кПа/л*с |
Важное диагностическое значение после спирометрии также имеет петля «поток-объем», график которой изображен ниже. По вертикальной оси отображена скорость потока, а по горизонтальной – величина легочного объема. Современные спирометры строят ее автоматически.

Нормальный вид петли «поток-объем»
При беременности
Проведение спирометрии во время беременности возможно. Но, рекомендуется проконсультироваться с врачом.
Отзывы
Отзывы пациентов, которые прошли данное исследование в основном хорошие. Они отмечают, что спирометрия обладает высокой информативностью, процедура не дорогая, но при этом простая и финансово доступная.
- «… Проходил эту процедуру и перед, и во время и после лечения. Каждый раз наглядно на графике было видно, что не так и что меняет в лучшую сторону. Один раз делали с применением Сальбутамола. Но у меня, к сожалению, оказалась на него аллергия. А сама процедура простая и полезная».
- «… Обследование проходила моя дочь. Процедура нужная, проходить ее легко, организму никак не вредит и стоит дешево, результат – сразу наглядно. Правда, возникли проблемы с тем, что дочка кашляла, и не всегда могла точно выполнять команды врача. Но вроде справились».
- «… Спирометрию проходила несколько раз во время проф. осмотров во время учебы. Иногда пересдавала тесты по несколько раз, в итоге все оказывалось в норме».
Цена
Стоимость исследования функции внешнего дыхания может различаться, в зависимости от региона, города и клиники, в которой ее проводят. Примерная цена – около 1000-1500 рублей.
Цены в клиниках
Спирометрия — диагностический метод, позволяющий определить функцию внешнего дыхания с помощью специального прибора. Процедура назначается пациентам, если требуется оценить объем вдыхаемого и выдыхаемого ими воздуха, а также определить скорость его прохождения по дыхательным путям в состоянии покоя и при нагрузке.

- Для чего назначается спирометрия?
- Подготовка к процедуре и ее проведение
- Результаты, показатели, норма для мужчин и женщин
- Есть ли противопоказания к спирографии?
Для чего назначается спирометрия?
Процедура проводится, если у пациента есть жалобы на проблемы с дыханием.
Показаниями к ней являются:
- продолжительный кашель (более 3–4 недель);
- сильная одышка;
- давящие боли в грудной клетке;
- наличие у пациента острых и хронических заболеваний респираторных органов, которые оказывают влияние на объем и качество дыхания;
- частые обострения бронхита.
Обследование обязательно назначают курильщикам со стажем, людям, которые проживают в регионах с сильно загрязненным воздухом (например, в крупных промышленных городах), а также тем, кто работает в условиях сильного запыления помещений. Лицам с наследственной предрасположенностью к респираторным патологиям также назначают спирометрию минимум 1–2 раза в год.

При помощи этого исследования специалист может:
- оценить общее состояние дыхательных органов пациента, а также сердечно-сосудистой системы;
- выявить заболевания, обусловленные профессиональной деятельностью;
- диагностировать хронические заболевания легких, различные пульмонологические и бронхиальные отклонения, а также
- оценить степень их тяжести и характер течения;
- оценить эффективность проводимой терапии;
- определить риски хирургического вмешательства.
Спирометрия проводится с применением специального прибора — спирометра. Он измеряет объем воздуха, который выходит из легких при наибольшем выдохе после наибольшего вдоха. Также этот прибор позволяет определить следующие показатели:
- жизненную емкость легких, то есть максимальное количество воздуха, которое пациент может глубоко вдохнуть;
- форсированную емкость легких (разница в объемах в начале и конце полного выдоха);
- функциональную остаточную емкость (объем воздуха, который остается в легких после спокойного выдоха);
- минутный объем дыхания;
- максимальную вентиляцию легких.

Подготовка к процедуре и ее проведение
Пациентам, которым назначили спирометрию, необходимо правильно подготовиться к исследованию, чтобы получить максимально достоверные результаты.
Процедуру проводят натощак, утром,
поэтому с момента последнего приема пищи должно пройти не менее 8 часов.
Другие рекомендации по подготовке к спирометрии:
- отказ от тяжелых физических нагрузок за сутки до назначенного мероприятия;
- отказ от курения минимум за 4 часа до исследования;
- отказ от крепкого чая и кофе в день проведения спирометрии;
- ограничение в приеме некоторых лекарственных препаратов за несколько дней до назначенного исследования (предварительно необходимо проконсультироваться с врачом).
Планируя поход на процедуру, нужно надеть одежду,
не оказывающую давления на грудную клетку.
30 минут до начала исследования
нужно провести в состоянии покоя, расслабиться.
- Спирометрию проводят, используя специальный аппарат, оснащенный датчиком для восприятия воздушного потока и устройством, преобразующим значения в цифровой формат для расчета необходимых показателей.
- Во время процедуры пациент сидит в кресле. На нос надевают зажим, в ротовой полости располагают одноразовый мундштук, который необходимо плотно обхватить губами и слегка прижать зубами.
- К мундштуку подсоединяют спирометр и включают его. Пациент в течение некоторого времени делает глубокие вдохи, затем выполняет указания врача: делает максимально возможные вдохи и выдохи, дышит через определенные промежутки времени.
- При необходимости врач может попросить пациента во время процедуры встать, изменить ритм дыхания, выполнить какие-либо другие действия.
Чтобы исключить погрешности в измерениях, пробы проводят несколько раз и учитывают средний показатель.
Иногда исследование проводится с использованием специальных препаратов. Это могут быть бронхолитики или метахолин. В первом случае выявляют бронхоспазм, во втором — астму.

Результаты, показатели, норма для мужчин и женщин
При проведении спирометрии специалист определяет несколько параметров, для которых существуют свои нормы. Это:
- ЧД (частота дыхательных движений за минуту). Показатель оценивается в состоянии покоя. В норме у здорового человека ЧД составляет 15-18 единиц.
- ДО (дыхательный объем, то есть то количество воздуха, которое попадает в легкие за один произведенный пациентом вдох). Показатели нормы довольно широкие: у мужчин — от 300 до 1200 мл, у женщин — от 250 до 800 мл.
- МОД (объем дыхания за минуту, то есть тот объем воздуха, который проходит по легким, за минуту). Этот показатель измеряют в состоянии покоя, а также при максимальной физической нагрузке. В первом случае норма составит 6-8 л/мин, во втором — 50-60 л/мин.
- ЖЕЛ (показатель жизненной емкости легочной ткани). Параметр позволяет определить объем воздуха, поступающий в легкие во время предельно выполненного вдоха после пикового выдоха. Для мужчин норма такого показателя находится в пределах 3,5-4,5 л, для женщин — 2,5-4 л.
- ФЖЕЛ (форсированный показатель жизненной емкости легочной ткани). Показатель определяет количество воздуха, которое выдыхается при глубоком выдохе после максимально глубокого вдоха. В норме этот параметр варьируется от 2,5 до 7,5 л.
- ОФВ1 (объем форсированного выдоха за секунду). Этот параметр определяет максимальный объем воздуха, выдыхаемый из легких за указанный промежуток времени при усиленном выдохе после максимально глубокого вдоха. Показатель нормы зависит от пола и возраста. В норме он находится в пределах между 70 и 85% от параметра ЖЕЛ.
- Индекс Тиффно. Параметр рассчитывается в процентах. Его определяют, поделив показатель ОФВ1 на ФЖЕЛ. У здорового человека индекс Тиффно составляет 75-85%. С возрастом это значение снижается.
Результаты спирографического исследования определяют путем сопоставления полученных величин с нормативными показателями. У здоровых людей параметры ЖЕЛ, ФЖЕЛ, ОФВ1 и индекса Тиффно составляют более 80%, но не более 120% от нормативных показателей. Если значение составляет 70% от нормы, то это указывает на наличие патологии. Чтобы определить точный диагноз, специалист назначает дополнительные исследования.
Нужно учитывать, что на функции дыхания влияют не только проблемы со здоровьем респираторных органов, но и некоторые другие факторы и системы организма. Это сутулость и сколиоз, не позволяющие легким раскрываться в полной мере, заболевания позвоночника, системные заболевания крови.

Есть ли противопоказания к спирографии?
Несмотря на простоту и безопасность процедуры, есть ряд противопоказаний к ее проведению. Это:
- туберкулез;
- недавно проведенные хирургические вмешательства в области брюшной полости или загрудинного пространства;
- расслаивающаяся аневризма аорты;
- пневмоторакс;
- психические расстройства;
- инсульт или инфаркт, перенесенные пациентом в течение последнего полугодия;
- острая сердечная недостаточность;
- эпилепсия;
- общее тяжелое состояние пациента.
Спирография не проводится детям в возрасте до 5 лет.
Спирометрия или спирография – функциональный метод диагностики, который помогает провести исследование функции внешнего дыхания с помощью специального устройства (спирометра или спирографа). Процедура абсолютно безболезненна, не имеет особых противопоказаний, выполняется амбулаторно без специфической подготовки.
Врачи центра «СМ-клиника» рассказывают, что такое спирометрия, как проводится эта процедура и что можно определить с помощью методики.
Общая информация об исследовании
Спирометрия выполняется с использованием специального медицинского прибора, который состоит из высокочувствительного датчика, реагирующего на воздушный поток, и электронно-вычислительных систем. В процессе исследования устройство фиксирует все необходимые параметры, преобразует данные в цифровой вид и выводит информацию на экран монитора.
Спирометрия показывает величину объема воздуха, проходящего через дыхательные пути после максимального вдоха и максимально возможного выдоха, что помогает врачу оценить функцию легких. Оцениваются показатели:
- общего объема легких;
- величины резервного вдоха и выдоха;
- жизненной емкости легких.
Для взрослых пациентов существуют определенные нормы показателей спирометрии, рассчитанные по возрасту у взрослых мужчин и женщин. Отклонения от этих цифр далеко не всегда являются признаком патологии, рассматривать полученные данные необходимо в комплексе с жалобами пациента, клинической симптоматикой и с учетом многих других критериев.
Показания к спирографии
Основаниями для назначения исследования могут послужить:
- длительный кашель;
- одышка;
- синдром гипервентиляции легких;
- острые и хронические патологии респираторного характера, влияющие на качество и объем дыхания.
Другими показаниями для проведения спирометрии выступают:
- курение, особенно на протяжении 5 и более лет;
- острые аллергические реакции, сопряженные с нарушением дыхательных функций;
- нервно-мышечные патологии;
- механические травмы грудной клетки;
- врожденные аномалии развития органов дыхания.
Спирометрия также показана для определения общего физического статуса пациента в рамках оценки трудоспособности, выявления возможных патологий, вызванных профессиональной деятельностью и неблагоприятными условиями труда/окружающей обстановки. Методика помогает оценить риски хирургического лечения, проконтролировать течение болезни и назначенную терапию по поводу хронических обструктивных болезней легких.
Возможные противопоказания
Вероятными ограничениями для проведения любых типов спирометрии могут стать:
- туберкулез легких в острой фазе;
- недавние оперативные вмешательства;
- тяжелое общее состояние пациента;
- психические нарушения у больного, которые не позволяют ему выполнять указания врача во время исследования.
Методика не показана также детям младше 5 лет.
Преимущества спирографии
Ключевыми достоинствами методики считаются:
- высокая степень достоверности результатов;
- безопасность для здоровья пациента;
- отсутствие болезненности во время выполнения;
- минимальное количество противопоказаний;
- широкие диагностические возможности.
Кроме того, спирометрия позволяет оценивать не структурные и анатомические особенности дыхательных путей, как большинство визуализирующих способов диагностики, а функциональные параметры.
Подготовка и техника выполнения исследования
Для максимально точного результата спирометрии от пациента требуется:
- воздержаться от курения минимум за 3 часа до исследования;
- не есть, не пить за 1,5–2 часа до визита в клинику;
- накануне исследования отказаться от употребления любого алкоголя и средств, способных привести к возбудимости нервной системы, в том числе крепкого кофе, энергетиков и тонизирующих напитков;
- в день исследования исключить любые физические нагрузки и оставаться в состоянии покоя минимум за 30 минут до проведения теста.
Специалисты перед исследованием могут посоветовать временно отказаться от приема некоторых лекарственных препаратов, которые могут исказить результаты теста, в частности, сальбутамола, теофиллина и др.
Спирометрия выполняется в кабинете функциональной диагностики, оборудованном необходимой аппаратурой и приспособлениями. Пациента усаживают на стул или кушетку, зажимают нос специальным зажимом, выдают наконечник с загубником, который нужно плотно сжать губами.
Исследуемому необходимо сидеть с прямой спиной и слегка приподнятой головой. Диагностика проводится поэтапно с соблюдением определенного протокола. Врач, выполняя необходимые замеры и манипуляции, может попросить пациента встать, задержать или изменить ритм дыхания, выполнить какие-либо иные действия.
После окончания исследования пациент некоторое время отдыхает. При необходимости оценка дыхательных функций может проводиться неоднократно.
По времени тестирование занимает не более 30 минут. Результаты, как правило, выдаются почти сразу после проведения исследования.

Расшифровкой результатов спирометрии занимается врач, назначивший исследование. Важно понимать, что указанные в бланке референсные значения являются усредненными цифрами, и отклонения от них не могут свидетельствовать о наличии какой-либо патологии без других признаков болезни (жалоб, результатов иных обследований, клинических проявлений).
Узнать больше о технике выполнения спирографии, пройти исследование и получить квалифицированную консультацию опытных специалистов можно в центре «СМ-Клиника». Мы работаем ежедневно: записаться на прием можно круглосуточно по телефону или с помощью формы обратной связи прямо на сайте клиники.
Мнение врача
Спирометрия – современный и безопасный способ диагностики и контроля болезней легких и патологий сердечно-сосудистой системы. Он позволяет без вреда для здоровья и самочувствия пациента быстро определять объем дыхания и оценивать отдельные параметры, что имеет огромное диагностическое значение в пульмонологии и кардиологии.
Вопрос-ответ
Мне назначили спирометрию с бронхолитиком, зачем это нужно?
Исследование с использованием дополнительных препаратов в Вашем случае поможет выявить наличие бронхоспазмов. В некоторых под наблюдением врача ситуациях вместо бронхолитиков перед процедурой пациенту вводят метахолин.
Сколько вдохов делает взрослый здоровый человек?
В течение одной минуты взрослый человек без каких-либо явных или скрытых сердечно-легочных патологий делает 16–18 дыхательных движений, то есть выполняет поочередно вдох и выдох.
Источники
- Стручков, П. В. Спирометрия: руководство для врачей / П. В. Стручков, Д. В. Дроздов, О. Ф. Лукина. — 2-е изд., испр и доп. Москва: ГЭОТАР-Медиа, 2018.
- Спирометрия в повседневной врачебной практике. Чикина С.Ю., Черняк А.В., 2007 г.