From Wikipedia, the free encyclopedia
| Pharyngitis | |
|---|---|
| Other names | Acute sore throat |
 |
|
| Viral pharyngitis resulting in visible redness. | |
| Pronunciation |
|
| Specialty | Infectious disease |
| Symptoms | Sore throat, fever, runny nose, cough, headache, hoarse voice[1][2] |
| Complications | Sinusitis, acute otitis media[2] |
| Duration | 3–10 days, depending on cause[2][3] |
| Causes | Usually viral infection[2] |
| Diagnostic method | Based on symptoms, rapid antigen detection test, throat swab[2] |
| Differential diagnosis | Epiglottitis, thyroiditis, retropharyngeal abscess[2] |
| Treatment | lidocaine[2][4] |
| Frequency | ~7.5% of people in any 3-month period[5] |
Pharyngitis is inflammation of the back of the throat, known as the pharynx.[2] It typically results in a sore throat and fever.[2] Other symptoms may include a runny nose, cough, headache, difficulty swallowing, swollen lymph nodes, and a hoarse voice.[1][6] Symptoms usually last 3–5 days, but can be longer depending on cause.[2][3] Complications can include sinusitis and acute otitis media.[2] Pharyngitis is a type of upper respiratory tract infection.[7]
Most cases are caused by a viral infection.[2] Strep throat, a bacterial infection, is the cause in about 25% of children and 10% of adults.[2] Uncommon causes include other bacteria such as gonococcus, fungi, irritants such as smoke, allergies, and gastroesophageal reflux disease.[2][4] Specific testing is not recommended in people who have clear symptoms of a viral infection, such as a cold.[2] Otherwise, a rapid antigen detection test or throat swab is recommended.[2] PCR testing has become common as it is as good as taking a throat swab but gives a faster result.[8] Other conditions that can produce similar symptoms include epiglottitis, thyroiditis, retropharyngeal abscess, and occasionally heart disease.[2]
NSAIDs, such as ibuprofen, can be used to help with the pain.[2] Numbing medication, such as topical lidocaine, may also help.[4] Strep throat is typically treated with antibiotics, such as either penicillin or amoxicillin.[2] It is unclear whether steroids are useful in acute pharyngitis, other than possibly in severe cases, but a recent (2020) review found that when used in combination with antibiotics they moderately improved pain and the likelihood of resolution.[9][10]
About 7.5% of people have a sore throat in any 3-month period.[5] Two or three episodes in a year are not uncommon.[1] This resulted in 15 million physician visits in the United States in 2007.[4] Pharyngitis is the most common cause of a sore throat.[11] The word comes from the Greek word pharynx meaning «throat» and the suffix -itis meaning «inflammation».[12][13]
Classification[edit]

Pharyngitis is a type of inflammation caused by an upper respiratory tract infection. It may be classified as acute or chronic. Acute pharyngitis may be catarrhal, purulent, or ulcerative, depending on the causative agent and the immune capacity of the affected individual. Chronic pharyngitis may be catarrhal, hypertrophic, or atrophic.[citation needed]
Tonsillitis is a subtype of pharyngitis.[14] If the inflammation includes both the tonsils and other parts of the throat, it may be called pharyngotonsillitis or tonsillopharyngitis.[15] Another subclassification is nasopharyngitis (the common cold).[16]
Clergyman’s sore throat or clergyman’s throat is an archaic term formerly used for chronic pharyngitis associated with overuse of the voice as in public speaking. It was sometimes called dysphonia clericorum or chronic folliculitis sore throat.[17]
Cause[edit]
Most cases are due to an infectious organism acquired from close contact with an infected individual.[citation needed]
Viral[edit]

These comprise about 40–80% of all infectious cases and can be a feature of many different types of viral infections.[11][18]
- Adenovirus is the most common of the viral causes. Typically, the degree of neck lymph node enlargement is modest and the throat often does not appear red, although it is painful.
- The family Orthomyxoviridae which cause influenza are present with rapid onset high temperature, headache, and generalized ache. A sore throat may be associated.
- Infectious mononucleosis («glandular fever») is caused by the Epstein–Barr virus. This may cause significant lymph-node swelling and an exudative tonsillitis with marked redness and swelling of the throat. The heterophile test can be used if this is suspected.
- Herpes simplex virus can cause multiple mouth ulcers.
- Measles
- Common cold: rhinovirus, coronavirus, respiratory syncytial virus, and parainfluenza virus can cause infection of the throat, ear, and lungs causing standard cold-like symptoms and often pain.
Bacterial[edit]
A number of different bacteria can infect the human throat. The most common is group A streptococcus (Streptococcus pyogenes), but others include Streptococcus pneumoniae, Haemophilus influenzae, Bordetella pertussis, Bacillus anthracis, Corynebacterium diphtheriae, Neisseria gonorrhoeae, Chlamydophila pneumoniae, Mycoplasma pneumoniae, and Fusobacterium necrophorum.[19]
Streptococcal pharyngitis[edit]

Streptococcal pharyngitis or strep throat is caused by a group A beta-hemolytic streptococcus (GAS).[20] It is the most common bacterial cause of cases of pharyngitis (15–30%).[19] Common symptoms include fever, sore throat, and large lymph nodes. It is a contagious infection, spread by close contact with an infected individual. A definitive diagnosis is made based on the results of a throat culture. Antibiotics are useful to both prevent complications (such as rheumatic fever) and speed recovery.[21]
Fusobacterium necrophorum[edit]
Fusobacterium necrophorum is a normal inhabitant of the oropharyngeal flora and can occasionally create a peritonsillar abscess. In one out of 400 untreated cases, Lemierre’s syndrome occurs.[22]
Diphtheria[edit]
Diphtheria is a potentially life-threatening upper respiratory infection caused by Corynebacterium diphtheriae, which has been largely eradicated in developed nations since the introduction of childhood vaccination programs, but is still reported in the Third World and increasingly in some areas in Eastern Europe. Antibiotics are effective in the early stages, but recovery is generally slow.[citation needed]
Others[edit]
A few other causes are rare, but possibly fatal, and include parapharyngeal space infections: peritonsillar abscess («quinsy abscess»), submandibular space infection (Ludwig’s angina), and epiglottitis.[23][24][25]
Fungal[edit]
Some cases of pharyngitis are caused by fungal infection, such as Candida albicans, causing oral thrush.[26]
Noninfectious[edit]
Pharyngitis may also be caused by mechanical, chemical, or thermal irritation, for example cold air or acid reflux. Some medications may produce pharyngitis, such as pramipexole and antipsychotics.[27][28]
Diagnosis[edit]
| Points | Probability of Strep | Management |
|---|---|---|
| 1 or less | <10% | No antibiotic or culture needed |
| 2 | 11–17% | Antibiotic based on culture or rapid antigen detection test |
| 3 | 28–35% | |
| 4 or 5 | 52% | Empiric antibiotics |
Differentiating a viral and a bacterial cause of a sore throat based on symptoms alone is difficult.[29] Thus, a throat swab often is done to rule out a bacterial cause.[30]
The modified Centor criteria may be used to determine the management of people with pharyngitis. Based on five clinical criteria, it indicates the probability of a streptococcal infection.[21]
One point is given for each of the criteria:[21]
- Absence of a cough
- Swollen and tender cervical lymph nodes
- Temperature more than 38.0 °C (100.4 °F)
- Tonsillar exudate or swelling
- Age less than 15 (a point is subtracted if age is more than 44)
The Infectious Disease Society of America recommends against empirical treatment and considers antibiotics only appropriate following positive testing.[29] Testing is not needed in children under three, as both group A strep and rheumatic fever are rare, except if they have a sibling with the disease.[29]
Management[edit]
The majority of the time, treatment is symptomatic. Specific treatments are effective for bacterial, fungal, and herpes simplex infections.
Medications[edit]
- Pain medication, such as NSAIDs and acetaminophen (paracetamol), can help reduce the pain associated with a sore throat. Aspirin may be used in adults, but is not recommended in children due to the risk of Reye syndrome.[31]
- Steroids (such as dexamethasone) may be useful for severe pharyngitis.[32][10] Their general use, however, is poorly supported.[9]
- Viscous lidocaine relieves pain by numbing the mucous membranes.[33]
- Antibiotics are useful if a bacterial infection is the cause of the sore throat.[34][35] For viral infections, antibiotics have no effect. In the United States, they are used in 25% of people before a bacterial infection has been detected.[36]
- Oral analgesic solutions, the active ingredient is usually phenol, but also less commonly benzocaine, cetylpyridinium chloride, and/or menthol. Chloraseptic and Cepacol are two examples of brands of these kinds of analgesics.[citation needed]
Alternative[edit]
Gargling salt water is often suggested, but there is no evidence to support or discourage this practice.[4] Alternative medicines are promoted and used for the treatment of sore throats.[37] However, they are poorly supported by evidence.[37]
Epidemiology[edit]
Acute pharyngitis is the most common cause of a sore throat and, together with cough, it is diagnosed in more than 1.9 million people a year in the United States.[11]
References[edit]
- ^ a b c Rutter, Paul Professor; Newby, David (2015). Community Pharmacy ANZ: Symptoms, Diagnosis and Treatment. Elsevier Health Sciences. p. 19. ISBN 9780729583459. Archived from the original on 8 September 2017.
- ^ a b c d e f g h i j k l m n o p q r s Hildreth, AF; Takhar, S; Clark, MA; Hatten, B (September 2015). «Evidence-Based Evaluation And Management Of Patients With Pharyngitis In The Emergency Department». Emergency Medicine Practice. 17 (9): 1–16, quiz 16–7. PMID 26276908.
- ^ a b David A.Warrell; Timothy M. Cox; John D. Firth, eds. (2012). Oxford textbook of medicine infection. Oxford: Oxford University Press. pp. 280–281. ISBN 9780191631733. Archived from the original on 10 October 2016.
- ^ a b c d e Weber, R (March 2014). «Pharyngitis». Primary Care. 41 (1): 91–8. doi:10.1016/j.pop.2013.10.010. PMC 7119355. PMID 24439883.
- ^ a b Jones, Roger (2004). Oxford Textbook of Primary Medical Care. Oxford University Press. p. 674. ISBN 9780198567820. Retrieved 4 August 2016.
- ^ Neville, Brad W.; Damm, Douglas D.; Allen, Carl M.; Chi, Angela C. (2016). Oral and maxillofacial pathology (4th ed.). St. Louis, MO: Elsevier. p. 166. ISBN 9781455770526. OCLC 908336985. Archived from the original on 28 October 2021. Retrieved 17 March 2020.
- ^ «Pharyngitis». National Library of Medicine. Archived from the original on 20 May 2016. Retrieved 4 August 2016.
- ^ «Acute pharyngitis — Symptoms, diagnosis and treatment | BMJ Best Practice». bestpractice.bmj.com.
- ^ a b Principi, N; Bianchini, S; Baggi, E; Esposito, S (February 2013). «No evidence for the effectiveness of systemic corticosteroids in acute pharyngitis, community-acquired pneumonia and acute otitis media». European Journal of Clinical Microbiology & Infectious Diseases. 32 (2): 151–60. doi:10.1007/s10096-012-1747-y. PMC 7087613. PMID 22993127.
- ^ a b de Cassan, Simone; Thompson, Matthew J.; Perera, Rafael; Glasziou, Paul P.; Del Mar, Chris B.; Heneghan, Carl J.; Hayward, Gail (1 May 2020). «Corticosteroids as standalone or add-on treatment for sore throat». The Cochrane Database of Systematic Reviews. 2020 (5): CD008268. doi:10.1002/14651858.CD008268.pub3. ISSN 1469-493X. PMC 7193118. PMID 32356360.
- ^ a b c Marx, John (2010). Rosen’s emergency medicine: concepts and clinical practice (7th ed.). Philadelphia, Pennsylvania: Mosby/Elsevier. Chapter 30. ISBN 978-0-323-05472-0.
- ^ Beachey, Will (2013). Respiratory Care Anatomy and Physiology, Foundations for Clinical Practice,3: Respiratory Care Anatomy and Physiology. Elsevier Health Sciences. p. 5. ISBN 978-0323078665. Archived from the original on 8 September 2017.
- ^ Hegner, Barbara; Acello, Barbara; Caldwell, Esther (2009). Nursing Assistant: A Nursing Process Approach – Basics. Cengage Learning. p. 45. ISBN 9781111780500. Archived from the original on 8 September 2017.
- ^ «Tonsillitis». Archived from the original on 25 March 2016. Retrieved 4 August 2016.
- ^ Rafei K, Lichenstein R (2006). «Airway Infectious Disease Emergencies». Pediatric Clinics of North America. 53 (2): 215–242. doi:10.1016/j.pcl.2005.10.001. PMID 16574523.
- ^ «www.nlm.nih.gov». Archived from the original on 17 November 2015.
- ^ Broadwater, Kimberly (2021). «Clergyman’s Sore Throat». Journal of Singing. 78 (1): 113–117. doi:10.53830/CNLB1302. ISSN 2769-4046. S2CID 239663449.
- ^ Acerra JR. «Pharyngitis». eMedicine. Archived from the original on 17 March 2010. Retrieved 28 April 2010.
- ^ a b Bisno AL (January 2001). «Acute pharyngitis». N Engl J Med. 344 (3): 205–11. doi:10.1056/NEJM200101183440308. PMID 11172144.
- ^ Baltimore RS (February 2010). «Re-evaluation of antibiotic treatment of streptococcal pharyngitis». Curr. Opin. Pediatr. 22 (1): 77–82. doi:10.1097/MOP.0b013e32833502e7. PMID 19996970. S2CID 13141765.
- ^ a b c Choby BA (March 2009). «Diagnosis and treatment of streptococcal pharyngitis». Am Fam Physician. 79 (5): 383–90. PMID 19275067. Archived from the original on 8 February 2015.
- ^ Centor RM (1 December 2009). «Expand the pharyngitis paradigm for adolescents and young adults». Ann Intern Med. 151 (11): 812–5. CiteSeerX 10.1.1.669.7473. doi:10.7326/0003-4819-151-11-200912010-00011. PMID 19949147. S2CID 207535809.
- ^ «UpToDate Inc». Archived from the original on 27 June 2009. (registration required)
- ^ Reynolds SC, Chow AW (September–October 2009). «Severe soft tissue infections of the head and neck: a primer for critical care physicians». Lung. 187 (5): 271–9. doi:10.1007/s00408-009-9153-7. PMID 19653038. S2CID 9009912.
- ^ Bansal A, Miskoff J, Lis RJ (January 2003). «Otolaryngologic critical care». Crit Care Clin. 19 (1): 55–72. doi:10.1016/S0749-0704(02)00062-3. PMID 12688577.
- ^ Harvard Medical School. «Sore Throat (Pharyngitis)». Harvard Health Publishing Harvard Medical School. Harvard Health Publishing. Retrieved 3 December 2019.
- ^ «Mirapex product insert» (PDF). Boehringer Ingelheim. 2009. Archived (PDF) from the original on 14 June 2010. Retrieved 30 June 2010.
- ^ «Mosby’s Medical Dictionary, 8th edition». Elsevier. 2009. Retrieved 30 June 2010.
- ^ a b c Shulman ST, Bisno AL, Clegg HW, Gerber MA, Kaplan EL, Lee G, Martin JM, Van Beneden C (9 September 2012). «Clinical Practice Guideline for the Diagnosis and Management of Group A Streptococcal Pharyngitis: 2012 Update by the Infectious Diseases Society of America». Clinical Infectious Diseases. 55 (10): e86–102. doi:10.1093/cid/cis629. PMC 7108032. PMID 22965026.
- ^ Del Mar C (1992). «Managing sore throat: a literature review. I. Making the diagnosis». Medical Journal of Australia. 156 (8): 572–5. doi:10.5694/j.1326-5377.1992.tb121422.x. PMID 1565052.
- ^ Baltimore RS (February 2010). «Re-evaluation of antibiotic treatment of streptococcal pharyngitis». Current Opinion in Pediatrics. 22 (Curr. Opin. Pediatr. 22 (1)): 77–82. doi:10.1097/MOP.0b013e32833502e7. PMID 19996970. S2CID 13141765.
- ^ Hayward G, Thompson M, Heneghan C, Perera R, Del Mar C, Glasziou P (2009). «Corticosteroids for pain relief in sore throat: systematic review and meta-analysis». BMJ. 339: b2976. doi:10.1136/bmj.b2976. PMC 2722696. PMID 19661138.
- ^ «LIDOCAINE VISCOUS (Xylocaine Viscous) side effects, medical uses, and drug interactions». Archived from the original on 8 April 2010.
- ^ Kocher, JJ; Selby, TD (1 July 2014). «Antibiotics for sore throat». American Family Physician. 90 (1): 23–4. PMID 25077497.
- ^ Spinks, Anneliese; Glasziou, Paul P.; Del Mar, Chris B. (9 December 2021). «Antibiotics for treatment of sore throat in children and adults». The Cochrane Database of Systematic Reviews. 2021 (12): CD000023. doi:10.1002/14651858.CD000023.pub5. ISSN 1469-493X. PMC 8655103. PMID 34881426.
- ^ Urkin, J; Allenbogen, M; Friger, M; Vinker, S; Reuveni, H; Elahayani, A (November 2013). «Acute pharyngitis: low adherence to guidelines highlights need for greater flexibility in managing paediatric cases». Acta Paediatrica. 102 (11): 1075–80. doi:10.1111/apa.12364. PMID 23879261. S2CID 24465793.
- ^ a b «Sore throat: Self-care». Mayo Clinic. Archived from the original on 29 September 2007. Retrieved 17 September 2007.
External links[edit]
From Wikipedia, the free encyclopedia
| Pharyngitis | |
|---|---|
| Other names | Acute sore throat |
|
|
| Viral pharyngitis resulting in visible redness. | |
| Pronunciation |
|
| Specialty | Infectious disease |
| Symptoms | Sore throat, fever, runny nose, cough, headache, hoarse voice[1][2] |
| Complications | Sinusitis, acute otitis media[2] |
| Duration | 3–10 days, depending on cause[2][3] |
| Causes | Usually viral infection[2] |
| Diagnostic method | Based on symptoms, rapid antigen detection test, throat swab[2] |
| Differential diagnosis | Epiglottitis, thyroiditis, retropharyngeal abscess[2] |
| Treatment | lidocaine[2][4] |
| Frequency | ~7.5% of people in any 3-month period[5] |
Pharyngitis is inflammation of the back of the throat, known as the pharynx.[2] It typically results in a sore throat and fever.[2] Other symptoms may include a runny nose, cough, headache, difficulty swallowing, swollen lymph nodes, and a hoarse voice.[1][6] Symptoms usually last 3–5 days, but can be longer depending on cause.[2][3] Complications can include sinusitis and acute otitis media.[2] Pharyngitis is a type of upper respiratory tract infection.[7]
Most cases are caused by a viral infection.[2] Strep throat, a bacterial infection, is the cause in about 25% of children and 10% of adults.[2] Uncommon causes include other bacteria such as gonococcus, fungi, irritants such as smoke, allergies, and gastroesophageal reflux disease.[2][4] Specific testing is not recommended in people who have clear symptoms of a viral infection, such as a cold.[2] Otherwise, a rapid antigen detection test or throat swab is recommended.[2] PCR testing has become common as it is as good as taking a throat swab but gives a faster result.[8] Other conditions that can produce similar symptoms include epiglottitis, thyroiditis, retropharyngeal abscess, and occasionally heart disease.[2]
NSAIDs, such as ibuprofen, can be used to help with the pain.[2] Numbing medication, such as topical lidocaine, may also help.[4] Strep throat is typically treated with antibiotics, such as either penicillin or amoxicillin.[2] It is unclear whether steroids are useful in acute pharyngitis, other than possibly in severe cases, but a recent (2020) review found that when used in combination with antibiotics they moderately improved pain and the likelihood of resolution.[9][10]
About 7.5% of people have a sore throat in any 3-month period.[5] Two or three episodes in a year are not uncommon.[1] This resulted in 15 million physician visits in the United States in 2007.[4] Pharyngitis is the most common cause of a sore throat.[11] The word comes from the Greek word pharynx meaning «throat» and the suffix -itis meaning «inflammation».[12][13]
Classification[edit]
Pharyngitis is a type of inflammation caused by an upper respiratory tract infection. It may be classified as acute or chronic. Acute pharyngitis may be catarrhal, purulent, or ulcerative, depending on the causative agent and the immune capacity of the affected individual. Chronic pharyngitis may be catarrhal, hypertrophic, or atrophic.[citation needed]
Tonsillitis is a subtype of pharyngitis.[14] If the inflammation includes both the tonsils and other parts of the throat, it may be called pharyngotonsillitis or tonsillopharyngitis.[15] Another subclassification is nasopharyngitis (the common cold).[16]
Clergyman’s sore throat or clergyman’s throat is an archaic term formerly used for chronic pharyngitis associated with overuse of the voice as in public speaking. It was sometimes called dysphonia clericorum or chronic folliculitis sore throat.[17]
Cause[edit]
Most cases are due to an infectious organism acquired from close contact with an infected individual.[citation needed]
Viral[edit]
These comprise about 40–80% of all infectious cases and can be a feature of many different types of viral infections.[11][18]
- Adenovirus is the most common of the viral causes. Typically, the degree of neck lymph node enlargement is modest and the throat often does not appear red, although it is painful.
- The family Orthomyxoviridae which cause influenza are present with rapid onset high temperature, headache, and generalized ache. A sore throat may be associated.
- Infectious mononucleosis («glandular fever») is caused by the Epstein–Barr virus. This may cause significant lymph-node swelling and an exudative tonsillitis with marked redness and swelling of the throat. The heterophile test can be used if this is suspected.
- Herpes simplex virus can cause multiple mouth ulcers.
- Measles
- Common cold: rhinovirus, coronavirus, respiratory syncytial virus, and parainfluenza virus can cause infection of the throat, ear, and lungs causing standard cold-like symptoms and often pain.
Bacterial[edit]
A number of different bacteria can infect the human throat. The most common is group A streptococcus (Streptococcus pyogenes), but others include Streptococcus pneumoniae, Haemophilus influenzae, Bordetella pertussis, Bacillus anthracis, Corynebacterium diphtheriae, Neisseria gonorrhoeae, Chlamydophila pneumoniae, Mycoplasma pneumoniae, and Fusobacterium necrophorum.[19]
Streptococcal pharyngitis[edit]
Streptococcal pharyngitis or strep throat is caused by a group A beta-hemolytic streptococcus (GAS).[20] It is the most common bacterial cause of cases of pharyngitis (15–30%).[19] Common symptoms include fever, sore throat, and large lymph nodes. It is a contagious infection, spread by close contact with an infected individual. A definitive diagnosis is made based on the results of a throat culture. Antibiotics are useful to both prevent complications (such as rheumatic fever) and speed recovery.[21]
Fusobacterium necrophorum[edit]
Fusobacterium necrophorum is a normal inhabitant of the oropharyngeal flora and can occasionally create a peritonsillar abscess. In one out of 400 untreated cases, Lemierre’s syndrome occurs.[22]
Diphtheria[edit]
Diphtheria is a potentially life-threatening upper respiratory infection caused by Corynebacterium diphtheriae, which has been largely eradicated in developed nations since the introduction of childhood vaccination programs, but is still reported in the Third World and increasingly in some areas in Eastern Europe. Antibiotics are effective in the early stages, but recovery is generally slow.[citation needed]
Others[edit]
A few other causes are rare, but possibly fatal, and include parapharyngeal space infections: peritonsillar abscess («quinsy abscess»), submandibular space infection (Ludwig’s angina), and epiglottitis.[23][24][25]
Fungal[edit]
Some cases of pharyngitis are caused by fungal infection, such as Candida albicans, causing oral thrush.[26]
Noninfectious[edit]
Pharyngitis may also be caused by mechanical, chemical, or thermal irritation, for example cold air or acid reflux. Some medications may produce pharyngitis, such as pramipexole and antipsychotics.[27][28]
Diagnosis[edit]
| Points | Probability of Strep | Management |
|---|---|---|
| 1 or less | <10% | No antibiotic or culture needed |
| 2 | 11–17% | Antibiotic based on culture or rapid antigen detection test |
| 3 | 28–35% | |
| 4 or 5 | 52% | Empiric antibiotics |
Differentiating a viral and a bacterial cause of a sore throat based on symptoms alone is difficult.[29] Thus, a throat swab often is done to rule out a bacterial cause.[30]
The modified Centor criteria may be used to determine the management of people with pharyngitis. Based on five clinical criteria, it indicates the probability of a streptococcal infection.[21]
One point is given for each of the criteria:[21]
- Absence of a cough
- Swollen and tender cervical lymph nodes
- Temperature more than 38.0 °C (100.4 °F)
- Tonsillar exudate or swelling
- Age less than 15 (a point is subtracted if age is more than 44)
The Infectious Disease Society of America recommends against empirical treatment and considers antibiotics only appropriate following positive testing.[29] Testing is not needed in children under three, as both group A strep and rheumatic fever are rare, except if they have a sibling with the disease.[29]
Management[edit]
The majority of the time, treatment is symptomatic. Specific treatments are effective for bacterial, fungal, and herpes simplex infections.
Medications[edit]
- Pain medication, such as NSAIDs and acetaminophen (paracetamol), can help reduce the pain associated with a sore throat. Aspirin may be used in adults, but is not recommended in children due to the risk of Reye syndrome.[31]
- Steroids (such as dexamethasone) may be useful for severe pharyngitis.[32][10] Their general use, however, is poorly supported.[9]
- Viscous lidocaine relieves pain by numbing the mucous membranes.[33]
- Antibiotics are useful if a bacterial infection is the cause of the sore throat.[34][35] For viral infections, antibiotics have no effect. In the United States, they are used in 25% of people before a bacterial infection has been detected.[36]
- Oral analgesic solutions, the active ingredient is usually phenol, but also less commonly benzocaine, cetylpyridinium chloride, and/or menthol. Chloraseptic and Cepacol are two examples of brands of these kinds of analgesics.[citation needed]
Alternative[edit]
Gargling salt water is often suggested, but there is no evidence to support or discourage this practice.[4] Alternative medicines are promoted and used for the treatment of sore throats.[37] However, they are poorly supported by evidence.[37]
Epidemiology[edit]
Acute pharyngitis is the most common cause of a sore throat and, together with cough, it is diagnosed in more than 1.9 million people a year in the United States.[11]
References[edit]
- ^ a b c Rutter, Paul Professor; Newby, David (2015). Community Pharmacy ANZ: Symptoms, Diagnosis and Treatment. Elsevier Health Sciences. p. 19. ISBN 9780729583459. Archived from the original on 8 September 2017.
- ^ a b c d e f g h i j k l m n o p q r s Hildreth, AF; Takhar, S; Clark, MA; Hatten, B (September 2015). «Evidence-Based Evaluation And Management Of Patients With Pharyngitis In The Emergency Department». Emergency Medicine Practice. 17 (9): 1–16, quiz 16–7. PMID 26276908.
- ^ a b David A.Warrell; Timothy M. Cox; John D. Firth, eds. (2012). Oxford textbook of medicine infection. Oxford: Oxford University Press. pp. 280–281. ISBN 9780191631733. Archived from the original on 10 October 2016.
- ^ a b c d e Weber, R (March 2014). «Pharyngitis». Primary Care. 41 (1): 91–8. doi:10.1016/j.pop.2013.10.010. PMC 7119355. PMID 24439883.
- ^ a b Jones, Roger (2004). Oxford Textbook of Primary Medical Care. Oxford University Press. p. 674. ISBN 9780198567820. Retrieved 4 August 2016.
- ^ Neville, Brad W.; Damm, Douglas D.; Allen, Carl M.; Chi, Angela C. (2016). Oral and maxillofacial pathology (4th ed.). St. Louis, MO: Elsevier. p. 166. ISBN 9781455770526. OCLC 908336985. Archived from the original on 28 October 2021. Retrieved 17 March 2020.
- ^ «Pharyngitis». National Library of Medicine. Archived from the original on 20 May 2016. Retrieved 4 August 2016.
- ^ «Acute pharyngitis — Symptoms, diagnosis and treatment | BMJ Best Practice». bestpractice.bmj.com.
- ^ a b Principi, N; Bianchini, S; Baggi, E; Esposito, S (February 2013). «No evidence for the effectiveness of systemic corticosteroids in acute pharyngitis, community-acquired pneumonia and acute otitis media». European Journal of Clinical Microbiology & Infectious Diseases. 32 (2): 151–60. doi:10.1007/s10096-012-1747-y. PMC 7087613. PMID 22993127.
- ^ a b de Cassan, Simone; Thompson, Matthew J.; Perera, Rafael; Glasziou, Paul P.; Del Mar, Chris B.; Heneghan, Carl J.; Hayward, Gail (1 May 2020). «Corticosteroids as standalone or add-on treatment for sore throat». The Cochrane Database of Systematic Reviews. 2020 (5): CD008268. doi:10.1002/14651858.CD008268.pub3. ISSN 1469-493X. PMC 7193118. PMID 32356360.
- ^ a b c Marx, John (2010). Rosen’s emergency medicine: concepts and clinical practice (7th ed.). Philadelphia, Pennsylvania: Mosby/Elsevier. Chapter 30. ISBN 978-0-323-05472-0.
- ^ Beachey, Will (2013). Respiratory Care Anatomy and Physiology, Foundations for Clinical Practice,3: Respiratory Care Anatomy and Physiology. Elsevier Health Sciences. p. 5. ISBN 978-0323078665. Archived from the original on 8 September 2017.
- ^ Hegner, Barbara; Acello, Barbara; Caldwell, Esther (2009). Nursing Assistant: A Nursing Process Approach – Basics. Cengage Learning. p. 45. ISBN 9781111780500. Archived from the original on 8 September 2017.
- ^ «Tonsillitis». Archived from the original on 25 March 2016. Retrieved 4 August 2016.
- ^ Rafei K, Lichenstein R (2006). «Airway Infectious Disease Emergencies». Pediatric Clinics of North America. 53 (2): 215–242. doi:10.1016/j.pcl.2005.10.001. PMID 16574523.
- ^ «www.nlm.nih.gov». Archived from the original on 17 November 2015.
- ^ Broadwater, Kimberly (2021). «Clergyman’s Sore Throat». Journal of Singing. 78 (1): 113–117. doi:10.53830/CNLB1302. ISSN 2769-4046. S2CID 239663449.
- ^ Acerra JR. «Pharyngitis». eMedicine. Archived from the original on 17 March 2010. Retrieved 28 April 2010.
- ^ a b Bisno AL (January 2001). «Acute pharyngitis». N Engl J Med. 344 (3): 205–11. doi:10.1056/NEJM200101183440308. PMID 11172144.
- ^ Baltimore RS (February 2010). «Re-evaluation of antibiotic treatment of streptococcal pharyngitis». Curr. Opin. Pediatr. 22 (1): 77–82. doi:10.1097/MOP.0b013e32833502e7. PMID 19996970. S2CID 13141765.
- ^ a b c Choby BA (March 2009). «Diagnosis and treatment of streptococcal pharyngitis». Am Fam Physician. 79 (5): 383–90. PMID 19275067. Archived from the original on 8 February 2015.
- ^ Centor RM (1 December 2009). «Expand the pharyngitis paradigm for adolescents and young adults». Ann Intern Med. 151 (11): 812–5. CiteSeerX 10.1.1.669.7473. doi:10.7326/0003-4819-151-11-200912010-00011. PMID 19949147. S2CID 207535809.
- ^ «UpToDate Inc». Archived from the original on 27 June 2009. (registration required)
- ^ Reynolds SC, Chow AW (September–October 2009). «Severe soft tissue infections of the head and neck: a primer for critical care physicians». Lung. 187 (5): 271–9. doi:10.1007/s00408-009-9153-7. PMID 19653038. S2CID 9009912.
- ^ Bansal A, Miskoff J, Lis RJ (January 2003). «Otolaryngologic critical care». Crit Care Clin. 19 (1): 55–72. doi:10.1016/S0749-0704(02)00062-3. PMID 12688577.
- ^ Harvard Medical School. «Sore Throat (Pharyngitis)». Harvard Health Publishing Harvard Medical School. Harvard Health Publishing. Retrieved 3 December 2019.
- ^ «Mirapex product insert» (PDF). Boehringer Ingelheim. 2009. Archived (PDF) from the original on 14 June 2010. Retrieved 30 June 2010.
- ^ «Mosby’s Medical Dictionary, 8th edition». Elsevier. 2009. Retrieved 30 June 2010.
- ^ a b c Shulman ST, Bisno AL, Clegg HW, Gerber MA, Kaplan EL, Lee G, Martin JM, Van Beneden C (9 September 2012). «Clinical Practice Guideline for the Diagnosis and Management of Group A Streptococcal Pharyngitis: 2012 Update by the Infectious Diseases Society of America». Clinical Infectious Diseases. 55 (10): e86–102. doi:10.1093/cid/cis629. PMC 7108032. PMID 22965026.
- ^ Del Mar C (1992). «Managing sore throat: a literature review. I. Making the diagnosis». Medical Journal of Australia. 156 (8): 572–5. doi:10.5694/j.1326-5377.1992.tb121422.x. PMID 1565052.
- ^ Baltimore RS (February 2010). «Re-evaluation of antibiotic treatment of streptococcal pharyngitis». Current Opinion in Pediatrics. 22 (Curr. Opin. Pediatr. 22 (1)): 77–82. doi:10.1097/MOP.0b013e32833502e7. PMID 19996970. S2CID 13141765.
- ^ Hayward G, Thompson M, Heneghan C, Perera R, Del Mar C, Glasziou P (2009). «Corticosteroids for pain relief in sore throat: systematic review and meta-analysis». BMJ. 339: b2976. doi:10.1136/bmj.b2976. PMC 2722696. PMID 19661138.
- ^ «LIDOCAINE VISCOUS (Xylocaine Viscous) side effects, medical uses, and drug interactions». Archived from the original on 8 April 2010.
- ^ Kocher, JJ; Selby, TD (1 July 2014). «Antibiotics for sore throat». American Family Physician. 90 (1): 23–4. PMID 25077497.
- ^ Spinks, Anneliese; Glasziou, Paul P.; Del Mar, Chris B. (9 December 2021). «Antibiotics for treatment of sore throat in children and adults». The Cochrane Database of Systematic Reviews. 2021 (12): CD000023. doi:10.1002/14651858.CD000023.pub5. ISSN 1469-493X. PMC 8655103. PMID 34881426.
- ^ Urkin, J; Allenbogen, M; Friger, M; Vinker, S; Reuveni, H; Elahayani, A (November 2013). «Acute pharyngitis: low adherence to guidelines highlights need for greater flexibility in managing paediatric cases». Acta Paediatrica. 102 (11): 1075–80. doi:10.1111/apa.12364. PMID 23879261. S2CID 24465793.
- ^ a b «Sore throat: Self-care». Mayo Clinic. Archived from the original on 29 September 2007. Retrieved 17 September 2007.
External links[edit]
Фарингитом называется воспаление слизистой оболочки задней стенки зева (воспаление глотки). Глотка – это верхняя часть горла. Глотка состоит из трёх частей:
- носоглотка – начинается от задней части полости носа. При осмотре горла её не видно, так как она скрыта мягким нёбом;
- ротоглотка – это как раз тот отдел глотки, который мы наблюдаем при рассматривании горла;
- гортаноглотка – нижний отдел глотки.
В целом глотка принадлежит сразу двум системам организма. Она входит в состав как дыхательных, так и пищевых путей. Эта её особенность играет важную роль в развитии и проявлениях фарингита.
Есть вопросы?
Оставьте телефон –
и мы Вам перезвоним

Причины фарингита
В норме человек дышит носом. Нос человека устроен таким образом, чтобы подготавливать вдыхаемый воздух к его дальнейшему перемещению внутри организма. Носовые ходы имеют достаточный объём, чтобы вдыхаемый воздух поступал далее с некоторой задержкой; это позволяет ему согреваться и увлажняться – за счёт взаимодействия со слизистой оболочкой носовой полости. В носу воздух также очищается от пыли, частички которой задерживаются на слизистой и растущих на ней ресничках.
Ротовое дыхание – это запасной вариант, заложенный в наш организм на случай, если дыхание через нос невозможно. При этом в горло поступает неподготовленный воздух, сохраняющий свойства внешней среды. Он может быть холодным, сухим, содержать пыль, возбудителей инфекции и т.д.

Поэтому основной фактор, способствующий развитию фарингита, это нарушение носового дыхания. Если у человека заложен нос (а это может произойти по многим причинам, – например, вследствие разрастания аденоидов, полипов в носу, насморка), то он вынужден дышать ртом. В этом случае слизистая оболочка ротоглотки, подвергшаяся прямому воздействию атмосферного воздуха, быстро пересыхает, легко переохлаждается и может быть инфицирована патогенными микроорганизмами, всегда присутствующими в воздухе.
Довольно часто фарингит возникает на фоне насморка, вызванного вирусной инфекцией (ОРВИ). Это происходит, потому что слизь, стекающая при насморке по носоглотке, содержит вирус – возбудитель заболевания, и способствует расширению очага воспаления.
Но одного ротового дыхания для возникновения фарингита не достаточно. Многое зависит от общего состояния организма. Если организм ослаблен в результате перенесённых заболеваний, переутомления, недостатка витаминов, плохого питания, он становится более уязвим для инфекции.
Также факторами, способствующими развитию фарингита, являются курение и злоупотребление алкоголем, авитаминоз, сахарный диабет, неблагоприятные условия внешней среды (длительное воздействие пыли, горячего и сухого воздуха, задымления, химических испарений и т.п.).
Наиболее часто встречается фарингит вирусного происхождения, более редко – бактериальный, грибковый, аллергический и травматический фарингиты.
Формы фарингита

Различают острый и хронический фарингит.
Для острого фарингита характерны следующие симптомы:
- сухость и першение в горле;
- болезненность при глотании, особенно при сглатывании слюны (так называемый «пустой глоток»);
- иногда наблюдаются подъём температуры до 37,5-38°C и общая слабость.
Хронический фарингит обычно протекает при нормальной температуре. Довольно часто наблюдается сухой кашель, возникает постоянное желание прокашляться, «прочистить» горло. Больному приходится всё время сглатывать слизь, что вызывает болезненные ощущения. В результате повышается раздражительность, снижается внимание и работоспособность, нарушается сон.
Течение фарингита и его возможные осложнения
Острый фарингит, как правило, не представляет опасности. Однако лечение его должно быть соответствующим и своевременным. Если фарингит не лечить или лечить неправильно, он способен преподнести сюрпризы.
Во-первых, он может принять хроническую форму, при которой истончается слизистая, а боль в горле и кашель то пропадают, то возвращаются снова. Во-вторых, воспалительный процесс может, как говорится, «спуститься ниже», то есть перейти на гортань (в ларингит) и трахею (трахеит). Возможно формирование абсцессов (скоплений гноя) вокруг миндалин, под задней стенкой горла, в жировой ткани. А самое главное – человек, решивший, что у него фарингит, может легко ошибиться и пропустить начальную стадию более тяжелого заболевания, например, ангины.
Поэтому очень важно своевременно обратиться к врачу для установления точного диагноза и назначения курса лечения. Ангина вызывается бактериями, и для её лечения могут быть назначены антибиотики. Фарингит же обычно имеет вирусную природу, и антибиотики при фарингите будут только вредны – полезную микрофлору они уничтожат, а развитие болезни не остановят. С другой стороны, встречаются фарингиты, вызванные, как и ангина, стрептококковой инфекцией. Осложнения, которые они могут вызвать, столь же опасны. Это – аутоиммунные реакции, в числе которых ревматизм суставов и клапанов сердца, а также поражение почек (гломерулонефрит).
Симптомы фарингита
Фарингит, как правило, проявляется следующими симптомами:
Ощущение кома в горле
Ощущение кома в горле – довольно характерный для фарингита симптом. Сначала горло пересыхает, потом возникает ощущение дискомфорта, как будто что-то мешает сделать глоток.
Боль в горле
Развитие заболевания приводит к тому, что ощущение дискомфорта в горле переходит в боль. При осмотре видно, что горло покраснело. Слизистая горла может быть покрыта пленкой или гнойными выделениями. Язык может быть обложен (покрыт белым налетом).
Кашель
Кашель при фарингите обычно начинается с першения в горле. Хочется постоянно прокашляться. Развитие заболевания приводит к возникновению стойкого и долго сохраняющегося кашля. Кашель при фарингите может быть разным – сухим, горловым, бронхиальным. Довольно часто кашель усиливается ночью Самая распространённая форма кашля при фарингите – сухой кашель.
Подробнее о симптоме
Температура
Повышение температуры типично при остром фарингите и может не наблюдаться при хронической форме заболевания. При остром фарингите температура может подниматься до 38°C.
Подробнее о симптоме
Методы диагностики фарингита
С жалобами, соответствующими симптомам фарингита, Вы можете обратиться к врачу общей практики (семейному врачу или терапевту) или к профильному специалисту – отоларингологу (ЛОРу).
Детский приём ведут квалифицированные врачи-педиатры и детские ЛОР-врачи.
Для диагностики фарингита используются следующие методы:
Фарингоскопия
Фарингоскопия – визуальное исследование слизистой оболочки горла. При фарингите проводится орофарингоскопия – осмотр ротовой части горла. С помощью фарингоскопии врач обнаруживает факт воспаления — покраснение горла и нёбных дужек; видны отдельные воспаленные лимфоидные гранулы. Для врача важно убедиться, что несмотря на воспалительный процесс в горле, нёбные миндалины не имеют признаков воспаления, характерных для ангины, то есть имеет место именно фарингит.
Подробнее о методе диагностики
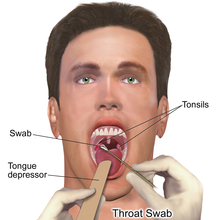
Мазок из зева
Мазок нужен для того, чтобы определить, какая инфекция вызвала воспаление – вирусная или бактериальная. На основании опроса больного и фарингоскопии это сделать нельзя.
Записаться на диагностику
Чтобы точно продиагностировать заболевание, запишитесь на прием к специалистам сети «Семейный доктор».
Методы лечения фарингита

Лечение фарингита обычно осуществляется в домашних условиях, однако если с симптомами фарингита самостоятельно быстро справиться не получается, следует обратиться к врачу. Не стоит доводить дело до хронической формы фарингита.
Выбор курса лечения фарингита зависит от того, какая причина вызвала заболевание. При инфекционной природе фарингита основой лечения становится подавление активности микроорганизмов-возбудителей.
Также важно устранить факторы, способствовавшие развитию фарингита (прежде всего, исключить курение на период лечения). Обязательно следует предпринять действия, направленные на укрепление иммунитета.
При хроническом фарингите важно убедиться, что выздоровление действительно состоялось. Поэтому по окончании курса лечения Вам могут быть назначена повторная сдача анализов. Если этого не сделать, есть вероятность, что активность возбудителя инфекции просто подавлена принимаемыми медикаментами, и после окончания приёма лекарств болезнь вернётся снова.
Антибактериальная терапия
В лечении фарингита могут применяться антибиотики. Антибиотики при фарингите действенны только в случае бактериальной инфекции, поэтому применению антибиотиков должен предшествовать бактериологический анализ.
Профилактика фарингита
В целях профилактики фарингита врачи «Семейного доктора» советуют:
- следить, чтобы дыхание было по преимуществу носовым. При выявлении аденоидов, полипов в носу, искривлённой носовой перегородки причину ротового дыхания желательно устранить;
- укреплять иммунитет, закаливать организм;
- увлажнять воздух в помещении. Нормальная влажность составляет 50-60%;
- чаще менять зубную щётку. Зубная щётка может накапливать вредные микроорганизмы;
- при появлении насморка или других признаков ОРЗ, сразу же начинать лечение.
Записаться на прием
Не занимайтесь самолечением. Обратитесь к нашим специалистам, которые правильно поставят диагноз и назначат лечение.
Оцените, насколько был полезен материал
Похожие заболевания
Все заболевания
From Wikipedia, the free encyclopedia
| Pharyngitis | |
|---|---|
| Other names | Acute sore throat |
|
|
| Viral pharyngitis resulting in visible redness. | |
| Pronunciation |
|
| Specialty | Infectious disease |
| Symptoms | Sore throat, fever, runny nose, cough, headache, hoarse voice[1][2] |
| Complications | Sinusitis, acute otitis media[2] |
| Duration | 3–10 days, depending on cause[2][3] |
| Causes | Usually viral infection[2] |
| Diagnostic method | Based on symptoms, rapid antigen detection test, throat swab[2] |
| Differential diagnosis | Epiglottitis, thyroiditis, retropharyngeal abscess[2] |
| Treatment | lidocaine[2][4] |
| Frequency | ~7.5% of people in any 3-month period[5] |
Pharyngitis is inflammation of the back of the throat, known as the pharynx.[2] It typically results in a sore throat and fever.[2] Other symptoms may include a runny nose, cough, headache, difficulty swallowing, swollen lymph nodes, and a hoarse voice.[1][6] Symptoms usually last 3–5 days, but can be longer depending on cause.[2][3] Complications can include sinusitis and acute otitis media.[2] Pharyngitis is a type of upper respiratory tract infection.[7]
Most cases are caused by a viral infection.[2] Strep throat, a bacterial infection, is the cause in about 25% of children and 10% of adults.[2] Uncommon causes include other bacteria such as gonococcus, fungi, irritants such as smoke, allergies, and gastroesophageal reflux disease.[2][4] Specific testing is not recommended in people who have clear symptoms of a viral infection, such as a cold.[2] Otherwise, a rapid antigen detection test or throat swab is recommended.[2] PCR testing has become common as it is as good as taking a throat swab but gives a faster result.[8] Other conditions that can produce similar symptoms include epiglottitis, thyroiditis, retropharyngeal abscess, and occasionally heart disease.[2]
NSAIDs, such as ibuprofen, can be used to help with the pain.[2] Numbing medication, such as topical lidocaine, may also help.[4] Strep throat is typically treated with antibiotics, such as either penicillin or amoxicillin.[2] It is unclear whether steroids are useful in acute pharyngitis, other than possibly in severe cases, but a recent (2020) review found that when used in combination with antibiotics they moderately improved pain and the likelihood of resolution.[9][10]
About 7.5% of people have a sore throat in any 3-month period.[5] Two or three episodes in a year are not uncommon.[1] This resulted in 15 million physician visits in the United States in 2007.[4] Pharyngitis is the most common cause of a sore throat.[11] The word comes from the Greek word pharynx meaning «throat» and the suffix -itis meaning «inflammation».[12][13]
Classification[edit]
Pharyngitis is a type of inflammation caused by an upper respiratory tract infection. It may be classified as acute or chronic. Acute pharyngitis may be catarrhal, purulent, or ulcerative, depending on the causative agent and the immune capacity of the affected individual. Chronic pharyngitis may be catarrhal, hypertrophic, or atrophic.[citation needed]
Tonsillitis is a subtype of pharyngitis.[14] If the inflammation includes both the tonsils and other parts of the throat, it may be called pharyngotonsillitis or tonsillopharyngitis.[15] Another subclassification is nasopharyngitis (the common cold).[16]
Clergyman’s sore throat or clergyman’s throat is an archaic term formerly used for chronic pharyngitis associated with overuse of the voice as in public speaking. It was sometimes called dysphonia clericorum or chronic folliculitis sore throat.[17]
Cause[edit]
Most cases are due to an infectious organism acquired from close contact with an infected individual.[citation needed]
Viral[edit]
These comprise about 40–80% of all infectious cases and can be a feature of many different types of viral infections.[11][18]
- Adenovirus is the most common of the viral causes. Typically, the degree of neck lymph node enlargement is modest and the throat often does not appear red, although it is painful.
- The family Orthomyxoviridae which cause influenza are present with rapid onset high temperature, headache, and generalized ache. A sore throat may be associated.
- Infectious mononucleosis («glandular fever») is caused by the Epstein–Barr virus. This may cause significant lymph-node swelling and an exudative tonsillitis with marked redness and swelling of the throat. The heterophile test can be used if this is suspected.
- Herpes simplex virus can cause multiple mouth ulcers.
- Measles
- Common cold: rhinovirus, coronavirus, respiratory syncytial virus, and parainfluenza virus can cause infection of the throat, ear, and lungs causing standard cold-like symptoms and often pain.
Bacterial[edit]
A number of different bacteria can infect the human throat. The most common is group A streptococcus (Streptococcus pyogenes), but others include Streptococcus pneumoniae, Haemophilus influenzae, Bordetella pertussis, Bacillus anthracis, Corynebacterium diphtheriae, Neisseria gonorrhoeae, Chlamydophila pneumoniae, Mycoplasma pneumoniae, and Fusobacterium necrophorum.[19]
Streptococcal pharyngitis[edit]
Streptococcal pharyngitis or strep throat is caused by a group A beta-hemolytic streptococcus (GAS).[20] It is the most common bacterial cause of cases of pharyngitis (15–30%).[19] Common symptoms include fever, sore throat, and large lymph nodes. It is a contagious infection, spread by close contact with an infected individual. A definitive diagnosis is made based on the results of a throat culture. Antibiotics are useful to both prevent complications (such as rheumatic fever) and speed recovery.[21]
Fusobacterium necrophorum[edit]
Fusobacterium necrophorum is a normal inhabitant of the oropharyngeal flora and can occasionally create a peritonsillar abscess. In one out of 400 untreated cases, Lemierre’s syndrome occurs.[22]
Diphtheria[edit]
Diphtheria is a potentially life-threatening upper respiratory infection caused by Corynebacterium diphtheriae, which has been largely eradicated in developed nations since the introduction of childhood vaccination programs, but is still reported in the Third World and increasingly in some areas in Eastern Europe. Antibiotics are effective in the early stages, but recovery is generally slow.[citation needed]
Others[edit]
A few other causes are rare, but possibly fatal, and include parapharyngeal space infections: peritonsillar abscess («quinsy abscess»), submandibular space infection (Ludwig’s angina), and epiglottitis.[23][24][25]
Fungal[edit]
Some cases of pharyngitis are caused by fungal infection, such as Candida albicans, causing oral thrush.[26]
Noninfectious[edit]
Pharyngitis may also be caused by mechanical, chemical, or thermal irritation, for example cold air or acid reflux. Some medications may produce pharyngitis, such as pramipexole and antipsychotics.[27][28]
Diagnosis[edit]
| Points | Probability of Strep | Management |
|---|---|---|
| 1 or less | <10% | No antibiotic or culture needed |
| 2 | 11–17% | Antibiotic based on culture or rapid antigen detection test |
| 3 | 28–35% | |
| 4 or 5 | 52% | Empiric antibiotics |
Differentiating a viral and a bacterial cause of a sore throat based on symptoms alone is difficult.[29] Thus, a throat swab often is done to rule out a bacterial cause.[30]
The modified Centor criteria may be used to determine the management of people with pharyngitis. Based on five clinical criteria, it indicates the probability of a streptococcal infection.[21]
One point is given for each of the criteria:[21]
- Absence of a cough
- Swollen and tender cervical lymph nodes
- Temperature more than 38.0 °C (100.4 °F)
- Tonsillar exudate or swelling
- Age less than 15 (a point is subtracted if age is more than 44)
The Infectious Disease Society of America recommends against empirical treatment and considers antibiotics only appropriate following positive testing.[29] Testing is not needed in children under three, as both group A strep and rheumatic fever are rare, except if they have a sibling with the disease.[29]
Management[edit]
The majority of the time, treatment is symptomatic. Specific treatments are effective for bacterial, fungal, and herpes simplex infections.
Medications[edit]
- Pain medication, such as NSAIDs and acetaminophen (paracetamol), can help reduce the pain associated with a sore throat. Aspirin may be used in adults, but is not recommended in children due to the risk of Reye syndrome.[31]
- Steroids (such as dexamethasone) may be useful for severe pharyngitis.[32][10] Their general use, however, is poorly supported.[9]
- Viscous lidocaine relieves pain by numbing the mucous membranes.[33]
- Antibiotics are useful if a bacterial infection is the cause of the sore throat.[34][35] For viral infections, antibiotics have no effect. In the United States, they are used in 25% of people before a bacterial infection has been detected.[36]
- Oral analgesic solutions, the active ingredient is usually phenol, but also less commonly benzocaine, cetylpyridinium chloride, and/or menthol. Chloraseptic and Cepacol are two examples of brands of these kinds of analgesics.[citation needed]
Alternative[edit]
Gargling salt water is often suggested, but there is no evidence to support or discourage this practice.[4] Alternative medicines are promoted and used for the treatment of sore throats.[37] However, they are poorly supported by evidence.[37]
Epidemiology[edit]
Acute pharyngitis is the most common cause of a sore throat and, together with cough, it is diagnosed in more than 1.9 million people a year in the United States.[11]
References[edit]
- ^ a b c Rutter, Paul Professor; Newby, David (2015). Community Pharmacy ANZ: Symptoms, Diagnosis and Treatment. Elsevier Health Sciences. p. 19. ISBN 9780729583459. Archived from the original on 8 September 2017.
- ^ a b c d e f g h i j k l m n o p q r s Hildreth, AF; Takhar, S; Clark, MA; Hatten, B (September 2015). «Evidence-Based Evaluation And Management Of Patients With Pharyngitis In The Emergency Department». Emergency Medicine Practice. 17 (9): 1–16, quiz 16–7. PMID 26276908.
- ^ a b David A.Warrell; Timothy M. Cox; John D. Firth, eds. (2012). Oxford textbook of medicine infection. Oxford: Oxford University Press. pp. 280–281. ISBN 9780191631733. Archived from the original on 10 October 2016.
- ^ a b c d e Weber, R (March 2014). «Pharyngitis». Primary Care. 41 (1): 91–8. doi:10.1016/j.pop.2013.10.010. PMC 7119355. PMID 24439883.
- ^ a b Jones, Roger (2004). Oxford Textbook of Primary Medical Care. Oxford University Press. p. 674. ISBN 9780198567820. Retrieved 4 August 2016.
- ^ Neville, Brad W.; Damm, Douglas D.; Allen, Carl M.; Chi, Angela C. (2016). Oral and maxillofacial pathology (4th ed.). St. Louis, MO: Elsevier. p. 166. ISBN 9781455770526. OCLC 908336985. Archived from the original on 28 October 2021. Retrieved 17 March 2020.
- ^ «Pharyngitis». National Library of Medicine. Archived from the original on 20 May 2016. Retrieved 4 August 2016.
- ^ «Acute pharyngitis — Symptoms, diagnosis and treatment | BMJ Best Practice». bestpractice.bmj.com.
- ^ a b Principi, N; Bianchini, S; Baggi, E; Esposito, S (February 2013). «No evidence for the effectiveness of systemic corticosteroids in acute pharyngitis, community-acquired pneumonia and acute otitis media». European Journal of Clinical Microbiology & Infectious Diseases. 32 (2): 151–60. doi:10.1007/s10096-012-1747-y. PMC 7087613. PMID 22993127.
- ^ a b de Cassan, Simone; Thompson, Matthew J.; Perera, Rafael; Glasziou, Paul P.; Del Mar, Chris B.; Heneghan, Carl J.; Hayward, Gail (1 May 2020). «Corticosteroids as standalone or add-on treatment for sore throat». The Cochrane Database of Systematic Reviews. 2020 (5): CD008268. doi:10.1002/14651858.CD008268.pub3. ISSN 1469-493X. PMC 7193118. PMID 32356360.
- ^ a b c Marx, John (2010). Rosen’s emergency medicine: concepts and clinical practice (7th ed.). Philadelphia, Pennsylvania: Mosby/Elsevier. Chapter 30. ISBN 978-0-323-05472-0.
- ^ Beachey, Will (2013). Respiratory Care Anatomy and Physiology, Foundations for Clinical Practice,3: Respiratory Care Anatomy and Physiology. Elsevier Health Sciences. p. 5. ISBN 978-0323078665. Archived from the original on 8 September 2017.
- ^ Hegner, Barbara; Acello, Barbara; Caldwell, Esther (2009). Nursing Assistant: A Nursing Process Approach – Basics. Cengage Learning. p. 45. ISBN 9781111780500. Archived from the original on 8 September 2017.
- ^ «Tonsillitis». Archived from the original on 25 March 2016. Retrieved 4 August 2016.
- ^ Rafei K, Lichenstein R (2006). «Airway Infectious Disease Emergencies». Pediatric Clinics of North America. 53 (2): 215–242. doi:10.1016/j.pcl.2005.10.001. PMID 16574523.
- ^ «www.nlm.nih.gov». Archived from the original on 17 November 2015.
- ^ Broadwater, Kimberly (2021). «Clergyman’s Sore Throat». Journal of Singing. 78 (1): 113–117. doi:10.53830/CNLB1302. ISSN 2769-4046. S2CID 239663449.
- ^ Acerra JR. «Pharyngitis». eMedicine. Archived from the original on 17 March 2010. Retrieved 28 April 2010.
- ^ a b Bisno AL (January 2001). «Acute pharyngitis». N Engl J Med. 344 (3): 205–11. doi:10.1056/NEJM200101183440308. PMID 11172144.
- ^ Baltimore RS (February 2010). «Re-evaluation of antibiotic treatment of streptococcal pharyngitis». Curr. Opin. Pediatr. 22 (1): 77–82. doi:10.1097/MOP.0b013e32833502e7. PMID 19996970. S2CID 13141765.
- ^ a b c Choby BA (March 2009). «Diagnosis and treatment of streptococcal pharyngitis». Am Fam Physician. 79 (5): 383–90. PMID 19275067. Archived from the original on 8 February 2015.
- ^ Centor RM (1 December 2009). «Expand the pharyngitis paradigm for adolescents and young adults». Ann Intern Med. 151 (11): 812–5. CiteSeerX 10.1.1.669.7473. doi:10.7326/0003-4819-151-11-200912010-00011. PMID 19949147. S2CID 207535809.
- ^ «UpToDate Inc». Archived from the original on 27 June 2009. (registration required)
- ^ Reynolds SC, Chow AW (September–October 2009). «Severe soft tissue infections of the head and neck: a primer for critical care physicians». Lung. 187 (5): 271–9. doi:10.1007/s00408-009-9153-7. PMID 19653038. S2CID 9009912.
- ^ Bansal A, Miskoff J, Lis RJ (January 2003). «Otolaryngologic critical care». Crit Care Clin. 19 (1): 55–72. doi:10.1016/S0749-0704(02)00062-3. PMID 12688577.
- ^ Harvard Medical School. «Sore Throat (Pharyngitis)». Harvard Health Publishing Harvard Medical School. Harvard Health Publishing. Retrieved 3 December 2019.
- ^ «Mirapex product insert» (PDF). Boehringer Ingelheim. 2009. Archived (PDF) from the original on 14 June 2010. Retrieved 30 June 2010.
- ^ «Mosby’s Medical Dictionary, 8th edition». Elsevier. 2009. Retrieved 30 June 2010.
- ^ a b c Shulman ST, Bisno AL, Clegg HW, Gerber MA, Kaplan EL, Lee G, Martin JM, Van Beneden C (9 September 2012). «Clinical Practice Guideline for the Diagnosis and Management of Group A Streptococcal Pharyngitis: 2012 Update by the Infectious Diseases Society of America». Clinical Infectious Diseases. 55 (10): e86–102. doi:10.1093/cid/cis629. PMC 7108032. PMID 22965026.
- ^ Del Mar C (1992). «Managing sore throat: a literature review. I. Making the diagnosis». Medical Journal of Australia. 156 (8): 572–5. doi:10.5694/j.1326-5377.1992.tb121422.x. PMID 1565052.
- ^ Baltimore RS (February 2010). «Re-evaluation of antibiotic treatment of streptococcal pharyngitis». Current Opinion in Pediatrics. 22 (Curr. Opin. Pediatr. 22 (1)): 77–82. doi:10.1097/MOP.0b013e32833502e7. PMID 19996970. S2CID 13141765.
- ^ Hayward G, Thompson M, Heneghan C, Perera R, Del Mar C, Glasziou P (2009). «Corticosteroids for pain relief in sore throat: systematic review and meta-analysis». BMJ. 339: b2976. doi:10.1136/bmj.b2976. PMC 2722696. PMID 19661138.
- ^ «LIDOCAINE VISCOUS (Xylocaine Viscous) side effects, medical uses, and drug interactions». Archived from the original on 8 April 2010.
- ^ Kocher, JJ; Selby, TD (1 July 2014). «Antibiotics for sore throat». American Family Physician. 90 (1): 23–4. PMID 25077497.
- ^ Spinks, Anneliese; Glasziou, Paul P.; Del Mar, Chris B. (9 December 2021). «Antibiotics for treatment of sore throat in children and adults». The Cochrane Database of Systematic Reviews. 2021 (12): CD000023. doi:10.1002/14651858.CD000023.pub5. ISSN 1469-493X. PMC 8655103. PMID 34881426.
- ^ Urkin, J; Allenbogen, M; Friger, M; Vinker, S; Reuveni, H; Elahayani, A (November 2013). «Acute pharyngitis: low adherence to guidelines highlights need for greater flexibility in managing paediatric cases». Acta Paediatrica. 102 (11): 1075–80. doi:10.1111/apa.12364. PMID 23879261. S2CID 24465793.
- ^ a b «Sore throat: Self-care». Mayo Clinic. Archived from the original on 29 September 2007. Retrieved 17 September 2007.
External links[edit]
From Wikipedia, the free encyclopedia
| Pharyngitis | |
|---|---|
| Other names | Acute sore throat |
|
|
| Viral pharyngitis resulting in visible redness. | |
| Pronunciation |
|
| Specialty | Infectious disease |
| Symptoms | Sore throat, fever, runny nose, cough, headache, hoarse voice[1][2] |
| Complications | Sinusitis, acute otitis media[2] |
| Duration | 3–10 days, depending on cause[2][3] |
| Causes | Usually viral infection[2] |
| Diagnostic method | Based on symptoms, rapid antigen detection test, throat swab[2] |
| Differential diagnosis | Epiglottitis, thyroiditis, retropharyngeal abscess[2] |
| Treatment | lidocaine[2][4] |
| Frequency | ~7.5% of people in any 3-month period[5] |
Pharyngitis is inflammation of the back of the throat, known as the pharynx.[2] It typically results in a sore throat and fever.[2] Other symptoms may include a runny nose, cough, headache, difficulty swallowing, swollen lymph nodes, and a hoarse voice.[1][6] Symptoms usually last 3–5 days, but can be longer depending on cause.[2][3] Complications can include sinusitis and acute otitis media.[2] Pharyngitis is a type of upper respiratory tract infection.[7]
Most cases are caused by a viral infection.[2] Strep throat, a bacterial infection, is the cause in about 25% of children and 10% of adults.[2] Uncommon causes include other bacteria such as gonococcus, fungi, irritants such as smoke, allergies, and gastroesophageal reflux disease.[2][4] Specific testing is not recommended in people who have clear symptoms of a viral infection, such as a cold.[2] Otherwise, a rapid antigen detection test or throat swab is recommended.[2] PCR testing has become common as it is as good as taking a throat swab but gives a faster result.[8] Other conditions that can produce similar symptoms include epiglottitis, thyroiditis, retropharyngeal abscess, and occasionally heart disease.[2]
NSAIDs, such as ibuprofen, can be used to help with the pain.[2] Numbing medication, such as topical lidocaine, may also help.[4] Strep throat is typically treated with antibiotics, such as either penicillin or amoxicillin.[2] It is unclear whether steroids are useful in acute pharyngitis, other than possibly in severe cases, but a recent (2020) review found that when used in combination with antibiotics they moderately improved pain and the likelihood of resolution.[9][10]
About 7.5% of people have a sore throat in any 3-month period.[5] Two or three episodes in a year are not uncommon.[1] This resulted in 15 million physician visits in the United States in 2007.[4] Pharyngitis is the most common cause of a sore throat.[11] The word comes from the Greek word pharynx meaning «throat» and the suffix -itis meaning «inflammation».[12][13]
Classification[edit]
Pharyngitis is a type of inflammation caused by an upper respiratory tract infection. It may be classified as acute or chronic. Acute pharyngitis may be catarrhal, purulent, or ulcerative, depending on the causative agent and the immune capacity of the affected individual. Chronic pharyngitis may be catarrhal, hypertrophic, or atrophic.[citation needed]
Tonsillitis is a subtype of pharyngitis.[14] If the inflammation includes both the tonsils and other parts of the throat, it may be called pharyngotonsillitis or tonsillopharyngitis.[15] Another subclassification is nasopharyngitis (the common cold).[16]
Clergyman’s sore throat or clergyman’s throat is an archaic term formerly used for chronic pharyngitis associated with overuse of the voice as in public speaking. It was sometimes called dysphonia clericorum or chronic folliculitis sore throat.[17]
Cause[edit]
Most cases are due to an infectious organism acquired from close contact with an infected individual.[citation needed]
Viral[edit]
These comprise about 40–80% of all infectious cases and can be a feature of many different types of viral infections.[11][18]
- Adenovirus is the most common of the viral causes. Typically, the degree of neck lymph node enlargement is modest and the throat often does not appear red, although it is painful.
- The family Orthomyxoviridae which cause influenza are present with rapid onset high temperature, headache, and generalized ache. A sore throat may be associated.
- Infectious mononucleosis («glandular fever») is caused by the Epstein–Barr virus. This may cause significant lymph-node swelling and an exudative tonsillitis with marked redness and swelling of the throat. The heterophile test can be used if this is suspected.
- Herpes simplex virus can cause multiple mouth ulcers.
- Measles
- Common cold: rhinovirus, coronavirus, respiratory syncytial virus, and parainfluenza virus can cause infection of the throat, ear, and lungs causing standard cold-like symptoms and often pain.
Bacterial[edit]
A number of different bacteria can infect the human throat. The most common is group A streptococcus (Streptococcus pyogenes), but others include Streptococcus pneumoniae, Haemophilus influenzae, Bordetella pertussis, Bacillus anthracis, Corynebacterium diphtheriae, Neisseria gonorrhoeae, Chlamydophila pneumoniae, Mycoplasma pneumoniae, and Fusobacterium necrophorum.[19]
Streptococcal pharyngitis[edit]
Streptococcal pharyngitis or strep throat is caused by a group A beta-hemolytic streptococcus (GAS).[20] It is the most common bacterial cause of cases of pharyngitis (15–30%).[19] Common symptoms include fever, sore throat, and large lymph nodes. It is a contagious infection, spread by close contact with an infected individual. A definitive diagnosis is made based on the results of a throat culture. Antibiotics are useful to both prevent complications (such as rheumatic fever) and speed recovery.[21]
Fusobacterium necrophorum[edit]
Fusobacterium necrophorum is a normal inhabitant of the oropharyngeal flora and can occasionally create a peritonsillar abscess. In one out of 400 untreated cases, Lemierre’s syndrome occurs.[22]
Diphtheria[edit]
Diphtheria is a potentially life-threatening upper respiratory infection caused by Corynebacterium diphtheriae, which has been largely eradicated in developed nations since the introduction of childhood vaccination programs, but is still reported in the Third World and increasingly in some areas in Eastern Europe. Antibiotics are effective in the early stages, but recovery is generally slow.[citation needed]
Others[edit]
A few other causes are rare, but possibly fatal, and include parapharyngeal space infections: peritonsillar abscess («quinsy abscess»), submandibular space infection (Ludwig’s angina), and epiglottitis.[23][24][25]
Fungal[edit]
Some cases of pharyngitis are caused by fungal infection, such as Candida albicans, causing oral thrush.[26]
Noninfectious[edit]
Pharyngitis may also be caused by mechanical, chemical, or thermal irritation, for example cold air or acid reflux. Some medications may produce pharyngitis, such as pramipexole and antipsychotics.[27][28]
Diagnosis[edit]
| Points | Probability of Strep | Management |
|---|---|---|
| 1 or less | <10% | No antibiotic or culture needed |
| 2 | 11–17% | Antibiotic based on culture or rapid antigen detection test |
| 3 | 28–35% | |
| 4 or 5 | 52% | Empiric antibiotics |
Differentiating a viral and a bacterial cause of a sore throat based on symptoms alone is difficult.[29] Thus, a throat swab often is done to rule out a bacterial cause.[30]
The modified Centor criteria may be used to determine the management of people with pharyngitis. Based on five clinical criteria, it indicates the probability of a streptococcal infection.[21]
One point is given for each of the criteria:[21]
- Absence of a cough
- Swollen and tender cervical lymph nodes
- Temperature more than 38.0 °C (100.4 °F)
- Tonsillar exudate or swelling
- Age less than 15 (a point is subtracted if age is more than 44)
The Infectious Disease Society of America recommends against empirical treatment and considers antibiotics only appropriate following positive testing.[29] Testing is not needed in children under three, as both group A strep and rheumatic fever are rare, except if they have a sibling with the disease.[29]
Management[edit]
The majority of the time, treatment is symptomatic. Specific treatments are effective for bacterial, fungal, and herpes simplex infections.
Medications[edit]
- Pain medication, such as NSAIDs and acetaminophen (paracetamol), can help reduce the pain associated with a sore throat. Aspirin may be used in adults, but is not recommended in children due to the risk of Reye syndrome.[31]
- Steroids (such as dexamethasone) may be useful for severe pharyngitis.[32][10] Their general use, however, is poorly supported.[9]
- Viscous lidocaine relieves pain by numbing the mucous membranes.[33]
- Antibiotics are useful if a bacterial infection is the cause of the sore throat.[34][35] For viral infections, antibiotics have no effect. In the United States, they are used in 25% of people before a bacterial infection has been detected.[36]
- Oral analgesic solutions, the active ingredient is usually phenol, but also less commonly benzocaine, cetylpyridinium chloride, and/or menthol. Chloraseptic and Cepacol are two examples of brands of these kinds of analgesics.[citation needed]
Alternative[edit]
Gargling salt water is often suggested, but there is no evidence to support or discourage this practice.[4] Alternative medicines are promoted and used for the treatment of sore throats.[37] However, they are poorly supported by evidence.[37]
Epidemiology[edit]
Acute pharyngitis is the most common cause of a sore throat and, together with cough, it is diagnosed in more than 1.9 million people a year in the United States.[11]
References[edit]
- ^ a b c Rutter, Paul Professor; Newby, David (2015). Community Pharmacy ANZ: Symptoms, Diagnosis and Treatment. Elsevier Health Sciences. p. 19. ISBN 9780729583459. Archived from the original on 8 September 2017.
- ^ a b c d e f g h i j k l m n o p q r s Hildreth, AF; Takhar, S; Clark, MA; Hatten, B (September 2015). «Evidence-Based Evaluation And Management Of Patients With Pharyngitis In The Emergency Department». Emergency Medicine Practice. 17 (9): 1–16, quiz 16–7. PMID 26276908.
- ^ a b David A.Warrell; Timothy M. Cox; John D. Firth, eds. (2012). Oxford textbook of medicine infection. Oxford: Oxford University Press. pp. 280–281. ISBN 9780191631733. Archived from the original on 10 October 2016.
- ^ a b c d e Weber, R (March 2014). «Pharyngitis». Primary Care. 41 (1): 91–8. doi:10.1016/j.pop.2013.10.010. PMC 7119355. PMID 24439883.
- ^ a b Jones, Roger (2004). Oxford Textbook of Primary Medical Care. Oxford University Press. p. 674. ISBN 9780198567820. Retrieved 4 August 2016.
- ^ Neville, Brad W.; Damm, Douglas D.; Allen, Carl M.; Chi, Angela C. (2016). Oral and maxillofacial pathology (4th ed.). St. Louis, MO: Elsevier. p. 166. ISBN 9781455770526. OCLC 908336985. Archived from the original on 28 October 2021. Retrieved 17 March 2020.
- ^ «Pharyngitis». National Library of Medicine. Archived from the original on 20 May 2016. Retrieved 4 August 2016.
- ^ «Acute pharyngitis — Symptoms, diagnosis and treatment | BMJ Best Practice». bestpractice.bmj.com.
- ^ a b Principi, N; Bianchini, S; Baggi, E; Esposito, S (February 2013). «No evidence for the effectiveness of systemic corticosteroids in acute pharyngitis, community-acquired pneumonia and acute otitis media». European Journal of Clinical Microbiology & Infectious Diseases. 32 (2): 151–60. doi:10.1007/s10096-012-1747-y. PMC 7087613. PMID 22993127.
- ^ a b de Cassan, Simone; Thompson, Matthew J.; Perera, Rafael; Glasziou, Paul P.; Del Mar, Chris B.; Heneghan, Carl J.; Hayward, Gail (1 May 2020). «Corticosteroids as standalone or add-on treatment for sore throat». The Cochrane Database of Systematic Reviews. 2020 (5): CD008268. doi:10.1002/14651858.CD008268.pub3. ISSN 1469-493X. PMC 7193118. PMID 32356360.
- ^ a b c Marx, John (2010). Rosen’s emergency medicine: concepts and clinical practice (7th ed.). Philadelphia, Pennsylvania: Mosby/Elsevier. Chapter 30. ISBN 978-0-323-05472-0.
- ^ Beachey, Will (2013). Respiratory Care Anatomy and Physiology, Foundations for Clinical Practice,3: Respiratory Care Anatomy and Physiology. Elsevier Health Sciences. p. 5. ISBN 978-0323078665. Archived from the original on 8 September 2017.
- ^ Hegner, Barbara; Acello, Barbara; Caldwell, Esther (2009). Nursing Assistant: A Nursing Process Approach – Basics. Cengage Learning. p. 45. ISBN 9781111780500. Archived from the original on 8 September 2017.
- ^ «Tonsillitis». Archived from the original on 25 March 2016. Retrieved 4 August 2016.
- ^ Rafei K, Lichenstein R (2006). «Airway Infectious Disease Emergencies». Pediatric Clinics of North America. 53 (2): 215–242. doi:10.1016/j.pcl.2005.10.001. PMID 16574523.
- ^ «www.nlm.nih.gov». Archived from the original on 17 November 2015.
- ^ Broadwater, Kimberly (2021). «Clergyman’s Sore Throat». Journal of Singing. 78 (1): 113–117. doi:10.53830/CNLB1302. ISSN 2769-4046. S2CID 239663449.
- ^ Acerra JR. «Pharyngitis». eMedicine. Archived from the original on 17 March 2010. Retrieved 28 April 2010.
- ^ a b Bisno AL (January 2001). «Acute pharyngitis». N Engl J Med. 344 (3): 205–11. doi:10.1056/NEJM200101183440308. PMID 11172144.
- ^ Baltimore RS (February 2010). «Re-evaluation of antibiotic treatment of streptococcal pharyngitis». Curr. Opin. Pediatr. 22 (1): 77–82. doi:10.1097/MOP.0b013e32833502e7. PMID 19996970. S2CID 13141765.
- ^ a b c Choby BA (March 2009). «Diagnosis and treatment of streptococcal pharyngitis». Am Fam Physician. 79 (5): 383–90. PMID 19275067. Archived from the original on 8 February 2015.
- ^ Centor RM (1 December 2009). «Expand the pharyngitis paradigm for adolescents and young adults». Ann Intern Med. 151 (11): 812–5. CiteSeerX 10.1.1.669.7473. doi:10.7326/0003-4819-151-11-200912010-00011. PMID 19949147. S2CID 207535809.
- ^ «UpToDate Inc». Archived from the original on 27 June 2009. (registration required)
- ^ Reynolds SC, Chow AW (September–October 2009). «Severe soft tissue infections of the head and neck: a primer for critical care physicians». Lung. 187 (5): 271–9. doi:10.1007/s00408-009-9153-7. PMID 19653038. S2CID 9009912.
- ^ Bansal A, Miskoff J, Lis RJ (January 2003). «Otolaryngologic critical care». Crit Care Clin. 19 (1): 55–72. doi:10.1016/S0749-0704(02)00062-3. PMID 12688577.
- ^ Harvard Medical School. «Sore Throat (Pharyngitis)». Harvard Health Publishing Harvard Medical School. Harvard Health Publishing. Retrieved 3 December 2019.
- ^ «Mirapex product insert» (PDF). Boehringer Ingelheim. 2009. Archived (PDF) from the original on 14 June 2010. Retrieved 30 June 2010.
- ^ «Mosby’s Medical Dictionary, 8th edition». Elsevier. 2009. Retrieved 30 June 2010.
- ^ a b c Shulman ST, Bisno AL, Clegg HW, Gerber MA, Kaplan EL, Lee G, Martin JM, Van Beneden C (9 September 2012). «Clinical Practice Guideline for the Diagnosis and Management of Group A Streptococcal Pharyngitis: 2012 Update by the Infectious Diseases Society of America». Clinical Infectious Diseases. 55 (10): e86–102. doi:10.1093/cid/cis629. PMC 7108032. PMID 22965026.
- ^ Del Mar C (1992). «Managing sore throat: a literature review. I. Making the diagnosis». Medical Journal of Australia. 156 (8): 572–5. doi:10.5694/j.1326-5377.1992.tb121422.x. PMID 1565052.
- ^ Baltimore RS (February 2010). «Re-evaluation of antibiotic treatment of streptococcal pharyngitis». Current Opinion in Pediatrics. 22 (Curr. Opin. Pediatr. 22 (1)): 77–82. doi:10.1097/MOP.0b013e32833502e7. PMID 19996970. S2CID 13141765.
- ^ Hayward G, Thompson M, Heneghan C, Perera R, Del Mar C, Glasziou P (2009). «Corticosteroids for pain relief in sore throat: systematic review and meta-analysis». BMJ. 339: b2976. doi:10.1136/bmj.b2976. PMC 2722696. PMID 19661138.
- ^ «LIDOCAINE VISCOUS (Xylocaine Viscous) side effects, medical uses, and drug interactions». Archived from the original on 8 April 2010.
- ^ Kocher, JJ; Selby, TD (1 July 2014). «Antibiotics for sore throat». American Family Physician. 90 (1): 23–4. PMID 25077497.
- ^ Spinks, Anneliese; Glasziou, Paul P.; Del Mar, Chris B. (9 December 2021). «Antibiotics for treatment of sore throat in children and adults». The Cochrane Database of Systematic Reviews. 2021 (12): CD000023. doi:10.1002/14651858.CD000023.pub5. ISSN 1469-493X. PMC 8655103. PMID 34881426.
- ^ Urkin, J; Allenbogen, M; Friger, M; Vinker, S; Reuveni, H; Elahayani, A (November 2013). «Acute pharyngitis: low adherence to guidelines highlights need for greater flexibility in managing paediatric cases». Acta Paediatrica. 102 (11): 1075–80. doi:10.1111/apa.12364. PMID 23879261. S2CID 24465793.
- ^ a b «Sore throat: Self-care». Mayo Clinic. Archived from the original on 29 September 2007. Retrieved 17 September 2007.
External links[edit]
| Фарингит | |
|---|---|
| Другие названия | Острая ангина |
|
|
| Вирусный фарингит с видимым покраснением. | |
| Произношение |
|
| Специальность | Инфекционное заболевание |
| Симптомы | Боль в горле, лихорадка, насморк, кашель, головная боль, хриплый голос |
| Осложнения | Синусит, острый средний отит |
| Продолжительность | 3–5 дней |
| Причины | Обычно вирусная инфекция |
| Метод диагностики | На основании симптомов, экспресс-тест на определение антигена, мазок из зева |
| Дифференциальный диагноз | Эпиглоттит, тиреоидит, заглоточный абсцесс |
| Лечение | НПВП, лидокаин |
| Частота | ~ 7,5% людей в любой 3-месячный период |
Фарингит — воспаление задней части глотки, известное как глотка. Обычно это приводит к боли в горле и лихорадке. Другие симптомы могут включать насморк, кашель, головную боль, затрудненное глотание, увеличение лимфатических узлов и хриплый голос. Симптомы обычно длятся 3–5 дней. Осложнения могут включать синусит и острый средний отит. Фарингит — это тип инфекции верхних дыхательных путей.
Большинство случаев вызвано вирусной инфекцией. Стрептококковая инфекция, бактериальная инфекция, является причиной примерно 25% детей и 10% взрослых. Нечастые причины включают другие бактерии, такие как гонорея, грибок, раздражители, такие как дым, аллергия и гастроэзофагеальная рефлюксная болезнь. Специальное тестирование не рекомендуется людям с явными симптомами вирусной инфекции, такими как простуда. В противном случае рекомендуется экспресс-тест на определение антигена (RADT) или мазок из зева. Другие состояния, которые могут вызывать аналогичные симптомы, включают эпиглоттит, тиреоидит, заглоточный абсцесс и иногда болезнь сердца.
НПВП, например ибупрофен можно использовать для облегчения боли. Также могут помочь обезболивающие, например лидокаин для местного применения. Стрептококковая ангина обычно лечится антибиотиками, такими как пенициллин или амоксициллин. Неясно, применимы ли стероиды при остром фарингите, кроме, возможно, в тяжелых случаях, но недавний обзор (2020) показал, что при использовании в сочетании с антибиотиками они умеренно уменьшают боль и вероятность выздоровления.
Около 7,5% людей болит горло в течение любого трехмесячного периода. Два-три эпизода в год — не редкость. Это привело к 15 миллионам визитов врачей в США в 2007 году. Фарингит — самая частая причина боли в горле. Слово происходит от греческого слова глотка, означающего «горло», и суффикса -ит, означающего «воспаление».
Содержание
- 1 Классификация
- 2 Причина
- 2.1 Вирус
- 2.2 Бактериальные
- 2.3 Грибковые
- 2.4 Неинфекционные
- 3 Диагноз
- 4 Ведение
- 4.1 Лекарства
- 4.2 Альтернатива
- 5 Эпидемиология
- 6 Ссылки
- 7 Внешние ссылки
Классификация
Нормальное горло
Фарингит — это тип воспаления, вызванный инфекцией верхних дыхательных путей. Его можно разделить на острый или хронический. Острый фарингит может быть катаральным, гнойным или язвенным, в зависимости от возбудителя и иммунной способности пострадавшего человека. Хронический фарингит может быть катаральным, гипертрофическим или атрофическим.
тонзиллитом — подтипом фарингита. Если воспаление охватывает и миндалины, и другие части глотки, это можно назвать фаринготонзиллитом. Другая подклассификация: ринофарингит (простуда).
Причина
Большинство случаев вызвано инфекционным организмом, приобретенным в результате тесного контакта с инфицированным
Вирусный
Экссудативный фарингит у человека с инфекционным мононуклеозом
Они составляют около 40–80% всех инфекционных случаев и могут быть признаком многих различных типов вирусные инфекции.
-
-
-
-
-
-
-
-
-
-
- Аденовирус — наиболее частая из вирусных причин. Обычно степень увеличения шейки лимфатического узла невелика, и горло часто не кажется красным, хотя и болезненным.
- Семейство Orthomyxoviridae, вызывающее грипп проявляются быстрым появлением высокой температуры, головной и генерализованной боли. Может быть ассоциирована боль в горле.
- Инфекционный мононуклеоз («железистая лихорадка») вызывается вирусом Эпштейна – Барра. Это может вызвать значительный отек лимфатических узлов и экссудативный тонзиллит с выраженным покраснением и отеком горла. При подозрении на это можно использовать гетерофильный тест.
- Вирус простого герпеса может вызывать множественные язвы во рту.
- Корь
- Простуда : риновирус, коронавирус, респираторно-синцитиальный вирус и вирус парагриппа могут вызывать инфекцию горла, уха и легких, вызывая стандартные симптомы простуды и часто вызывает боль.
-
-
-
-
-
-
-
-
-
Бактериальные
Множество различных бактерий могут инфицировать горло человека. Наиболее распространен стрептококк группы A (Streptococcus pyogenes), но другие включают Streptococcus pneumoniae, Haemophilus influenzae, Bordetella pertussis, Bacillus anthracis, Corynebacterium diphtheriae, Neisseria gonorrhoeae, Chlamydophila pneumoniae, Mycoplasma pneumoniae и Fusroobacterium 258>Стрептококковый фарингитСлучай стрептококкового фарингита
Стрептококковый фарингит или стрептококковый фарингит вызывается бета-гемолитическим стрептококком группы A (GAS). Это наиболее частая бактериальная причина фарингита (15–30%). Общие симптомы включают лихорадку, боль в горле и большие лимфатические узлы. Это заразная инфекция, передающаяся при тесном контакте с инфицированным человеком. Окончательный диагноз ставится на основании результатов посева из горла. Антибиотики полезны как для предотвращения осложнений (таких как ревматическая лихорадка ), так и для ускорения выздоровления.
- Fusobacterium necrophorum
Fusobacterium necrophorum — нормальный обитатель ротоглотки флора и иногда может образовывать перитонзиллярный абсцесс. В одном из 400 невылеченных случаев возникает синдром Лемьера.
- Дифтерия
Дифтерия — потенциально опасная для жизни инфекция верхних дыхательных путей, вызываемая Corynebacterium diphtheriae, которая был в значительной степени искоренен в развитых странах с момента введения программ вакцинации детей , но все еще регистрируется в странах третьего мира и все чаще в некоторых регионах Восточной Европы. Антибиотики эффективны на ранних стадиях, но выздоровление обычно происходит медленно.
- Другие
Некоторые другие причины редки, но могут быть смертельными и включают инфекции парафарингеального пространства : перитонзиллярный абсцесс («ангинозный абсцесс»), инфекция поднижнечелюстного пространства (ангина Людвига) и эпиглоттит.
грибок
Некоторые случаи фарингита вызваны грибковой инфекцией, например Candida albicans, вызывающий молочницу полости рта.
Неинфекционный
Фарингит также может быть вызван механическим, химическим или термическим раздражением, например холодным воздухом или кислотный рефлюкс. Некоторые лекарства могут вызывать фарингит, например прамипексол и антипсихотики.
Диагноз
| Баллы | Вероятность стрептококка | Ведение |
|---|---|---|
| 1 или меньше | <10% | Антибиотик или посев не требуется |
| 2 | 11–17% | Антибиотик на основе посева или экспресс-теста на определение антигена |
| 3 | 28–35% | |
| 4 или 5 | 52% | Эмпирические антибиотики |
мазок из горла
Трудно дифференцировать вирусную и бактериальную причину боли в горле на основе одних только симптомов. Таким образом, мазок из зева часто делается, чтобы исключить бактериальную причину.
Модифицированные критерии Centor могут использоваться для определения лечения людей с фарингитом. Основываясь на пяти клинических критериях, он указывает на вероятность стрептококковой инфекции.
По каждому из критериев дается один балл:
- Отсутствие кашля
- Отек и болезненность шейные лимфатические узлы
- Температура более 38,0 ° C (100,4 ° F)
- Тонзиллярный экссудат или опухоль
- Возраст менее 15 лет (если возраст старше 44 лет, вычитается балл)
Американское общество инфекционных болезней не рекомендует эмпирическое лечение и считает антибиотики целесообразными только после положительного результата тестирования. Детям младше трех лет обследование не требуется, поскольку стрептококковая инфекция группы А и ревматическая лихорадка встречаются редко, за исключением случаев, когда у них есть брат или сестра с этим заболеванием.
Ведение
в большинстве случаев лечение симптоматическое. Специальные методы лечения эффективны при бактериальных, грибковых инфекциях и инфекциях простого герпеса.
Лекарства
- Обезболивающие, такие как НПВП и ацетаминофен (парацетамол), могут помочь уменьшить боль, связанную с болью в горле. Аспирин можно применять у взрослых, но не рекомендуется у детей из-за риска синдрома Рея.
- . Стероиды (например, дексаметазон ) могут быть полезны при тяжелом фарингите. Однако их общее использование не поддерживается.
- Вязкий лидокаин снимает боль, онемение слизистых оболочек.
- Антибиотики полезны, если бактериальная инфекция является причиной больное горло. При вирусных инфекциях антибиотики не действуют. В США они используются у 25% людей до того, как была обнаружена бактериальная инфекция.
- Пероральные обезболивающие, активным ингредиентом обычно является фенол, но также реже бензокаин, хлорид цетилпиридиния и / или ментол. Хлоразептик и Цепакол — два примера марок этих видов анальгетиков.
Альтернатива
Полоскание горла соленой водой часто предлагается, но доказательства его полезности отсутствуют. Рекламируются и используются альтернативные лекарства для лечения боли в горле. Однако они плохо подкреплены доказательствами.
Эпидемиология
Острый фарингит — наиболее частая причина боли в горле, и вместе с кашлем он диагностируется в более более 1,9 миллиона человек в год в США.
Ссылки
Внешние ссылки
| Классификация | D
|
|---|---|
| Внешние ресурсы |
|
| На Викискладе есть средства массовой информации, связанные с фарингитом. |
Фарингит (Катар глотки)

Фарингит — это острый или хронический воспалительный процесс в слизистой оболочке задней стенки глотки, чаще вирусной или бактериальной природы. Проявляется першением, ощущением «комка» и болью в горле, усиливающейся при глотании, сухим кашлем, повышением температуры. В большинстве случаев возможно полное излечение, возможен переход острого процесса в хронический. Реже могут возникнуть грозные осложнения: ревматическое поражение сердца и суставов. Диагностируется по данным фарингоскопиии, результатов лабораторной идентификации возбудителя. Лечение включает местные процедуры (ингаляции, полоскания горла), антибиотикотерапию, хирургические манипуляции.
Общие сведения
Фарингит — воспаление слизистой глотки. Часто сочетается с тонзиллитом. В клинической отоларингологии выделяют два варианта течения фарингита: острый и хронический. Острые формы чаще регистрируются у детей, хронические — у лиц среднего и пожилого возраста. Острый фарингит чаще всего сопровождает течение острых респираторных вирусных инфекций. Хронический фарингит составляет 5-9% всей ЛОР-патологии.

Фарингит
Причины фарингита
Чаще всего причиной развития являются бактерии или вирусы. Вирусный фарингит составляет около 70% всех воспалительных процессов в слизистой оболочке глотки. В роли возбудителей может выступать аденовирус, вирус парагриппа, риновирус, короновирусы или цитомегаловирус. Бактериальный фарингит обычно вызывается стрептококками. В некоторых случаях возможно развитие грибкового фарингита (обычно – у больных с нарушенным иммунитетом или после длительного лечения антибиотиками). Реже причиной развития фарингита является аллергия, травма (при хирургическом вмешательстве или попадании инородного тела) или воздействие раздражающих факторов (облучение, щелочи, кислоты, пар или горячая жидкость).
Возникновение хронического фарингита может быть спровоцировано попаданием в глотку желудочного содержимого при грыже пищеводного отверстия диафрагмы и гастроэзофагеальном рефлюксе. Причиной развития хронического фарингита могут стать хронические воспалительные процессы в полости носа (ринит) и параназальных пазухах (синусит). Заболевание в этом случае вызывается не только постоянным дыханием через рот, но и действием сосудосуживающих капель, стекающих из носовой полости в глотку.
Факторы риска
Риск развития фарингита увеличивается при переохлаждении, нарушении иммунного статуса, тяжелых хронических заболеваниях, повышенном содержании в воздухе пыли и раздражающих химических веществ, курении и злоупотреблении алкоголем.
Классификация
Фарингит может быть острым или хроническим:
1. Острый фарингит. Обычно протекает диффузно и охватывает все отделы глотки.
2. Хронический фарингит. Как правило, имеет более четкую локализацию и поражает верхний, средний или нижний отдел глотки. Однако, выделение отдельных видов хронического фарингита в зависимости от локализации всегда производится с долей условности.
- гипертрофический
- атрофический
- катаральный.
Симптомы фарингита
Острый фарингит
Острый фарингит редко протекает изолированно. Как правило, развивается при инфекционных заболеваниях верхних дыхательных путей. Изолированный острый фарингит может наблюдаться при воздействии раздражителей непосредственно на слизистую оболочку глотки (дыхание на холоде через рот, холодная и горячая пища, употребление алкоголя, курение).
Пациент предъявляет жалобы на чувство першения и саднения в глотке, незначительную боль при глотании. Как правило, «пустой глоток» (проглатывание слюны) сопровождается большей болезненностью по сравнению с проглатыванием пищи. При распространении процесса на тубофарингеальные валики возможна иррадиация болей в уши. Обычно общее состояние не страдает или страдает незначительно. Температура тела может повышаться до субфебрильной.
У детей в возрасте до 2-х лет часто отмечается тяжелое течение острого фарингита. Воспалительный процесс распространяется на полость носа и носоглотку. Носовое дыхание нарушается. Возможно повышение температуры до фебрильной.
Хронический фарингит
Пациентов, страдающих хроническим атрофическим фарингитом, беспокоит сухость, чувство царапанья или першения в горле. Возможен сухой кашель. На фарингоскопии видна сухая, бледная, истонченная, блестящая (лаковая) слизистая оболочка глотки, местами покрытая слизью и корками.
При катаральном и гипертрофическом хроническом фарингите больные жалуются на чувство саднения, першения или инородного тела в горле, нерезкую боль при глотании. В глотке пациента постоянно скапливается густое слизистое отделяемое, поэтому больной постоянно откашливается. Кашель усиливается по утрам, в отдельных случаях сопровождается тошнотой и рвотой.
Осложнения
При остром (обычно стрептококковом) фарингите может развиться паратонзиллярный абсцесс. В некоторых случаях воспаление распространяется на близлежащие органы, вызывая ларингит и трахеит. Острый фарингит, при котором в качестве инфекционного агента выступает вызванный b-гемолитический стрептококк группы А, может сыграть роль пускового заболевания при остром суставном ревматизме.
Диагностика
Диагноз фарингита выставляется врачом-отоларингологом на основании характерных симптомов и данных фарингоскопии. Для определения природы возбудителя при необходимости проводится вирусологическое или бактериологическое исследование мазка из глотки.
При острой форме во время фарингоскопии выявляется гиперемия слизистой оболочки глотки, распространяющаяся на небные миндалины. Язычок отечен, на глотке местами обнаруживается слизисто-гнойный налет. У некоторых больных выявляется увеличение и болезненность верхних шейных лимфоузлов.
При катаральном фарингите выявляется разлитая гиперемия и утолщение слизистой оболочки глотки, язычка и мягкого неба. Глотка местами покрыта вязким слизистым или слизисто-гнойным отделяемым. Отдельные группы фолликулов увеличены. Для гипертрофического фарингита характерны более выраженные изменения. При гранулезном гипертрофическом фарингите наблюдается разрастание лимфоидной ткани в области задней стенки глотки, при боковом гипертрофическом фарингите – гиперплазия лимфоидной ткани за задними небными дужками.
Лечение фарингита
 Необходимо исключить факторы, вызывающие и поддерживающие воспаление в глотке. Пациенту рекомендуют воздержаться от курения, приема алкоголя и раздражающей пищи (соленой, острой, кислой, холодной или горячей). При установленной бактериальной природе фарингита в некоторых случаях проводится антибиотикотерапия.
Необходимо исключить факторы, вызывающие и поддерживающие воспаление в глотке. Пациенту рекомендуют воздержаться от курения, приема алкоголя и раздражающей пищи (соленой, острой, кислой, холодной или горячей). При установленной бактериальной природе фарингита в некоторых случаях проводится антибиотикотерапия.
Местное лечение заключается в полоскании теплыми растворами антисептиков через каждые полчаса-час. Показаны ингаляции с масляными препаратами и щелочными растворами, применение аэрозольных противовоспалительных препаратов.
При хроническом гипертрофическом фарингите выполняется прижигание гранул трихлоруксусной кислотой или раствором нитрата серебра. При выраженной гипертрофии применяется криотерапия, лазерное воздействие на гранулы глотки и радиоволновое туширование ее задней стенки.