Как правильно пишется слово «щитовидка»
щитови́дка
щитови́дка, -и, р. мн. -док
Источник: Орфографический
академический ресурс «Академос» Института русского языка им. В.В. Виноградова РАН (словарная база
2020)
Делаем Карту слов лучше вместе

Привет! Меня зовут Лампобот, я компьютерная программа, которая помогает делать
Карту слов. Я отлично
умею считать, но пока плохо понимаю, как устроен ваш мир. Помоги мне разобраться!
Спасибо! Я стал чуточку лучше понимать мир эмоций.
Вопрос: реликварий — это что-то нейтральное, положительное или отрицательное?
Ассоциации к слову «щитовидка»
Синонимы к слову «щитовидка»
Предложения со словом «щитовидка»
- Потом она говорила, что болезнь щитовидки спасла её от туберкулёза.
- Даже врачам и государственным деятелям, почему-либо не сведущим в вопросах йоддефицита и проблем щитовидки.
- Потом были язвы желудка и двенадцатиперстной кишки, желчекаменная болезнь, мочекаменная болезнь, воспаление щитовидки.
- (все предложения)
Отправить комментарий
Дополнительно
| Thyroid | |
|---|---|
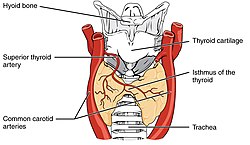
The human thyroid (tan), as viewed from the front; and arteries (red) supplying the gland. |
|
The thyroid is located in the neck, below the Adam’s apple. |
|
| Details | |
| Pronunciation | |
| Precursor | Thyroid diverticulum (an extension of endoderm into 2nd pharyngeal arch) |
| System | Endocrine system |
| Artery | Superior, Inferior thyroid arteries |
| Vein | Superior, middle, Inferior thyroid veins |
| Identifiers | |
| Latin | Glandula thyreoidea |
| MeSH | D013961 |
| TA98 | A11.3.00.001 |
| TA2 | 3863 |
| FMA | 9603 |
| Anatomical terminology
[edit on Wikidata] |
The thyroid, or thyroid gland, is an endocrine gland in vertebrates. In humans, it is in the neck and consists of two connected lobes. The lower two thirds of the lobes are connected by a thin band of tissue called the thyroid isthmus. The thyroid is located at the front of the neck, below the Adam’s apple. Microscopically, the functional unit of the thyroid gland is the spherical thyroid follicle, lined with follicular cells (thyrocytes), and occasional parafollicular cells that surround a lumen containing colloid. The thyroid gland secretes three hormones: the two thyroid hormones – triiodothyronine (T3) and thyroxine (T4) – and a peptide hormone, calcitonin. The thyroid hormones influence the metabolic rate and protein synthesis and growth and development in children. Calcitonin plays a role in calcium homeostasis.[1] Secretion of the two thyroid hormones is regulated by thyroid-stimulating hormone (TSH), which is secreted from the anterior pituitary gland. TSH is regulated by thyrotropin-releasing hormone (TRH), which is produced by the hypothalamus.[2]
Thyroid disorders include hyperthyroidism, hypothyroidism, thyroid inflammation (thyroiditis), thyroid enlargement (goitre), thyroid nodules, and thyroid cancer. Hyperthyroidism is characterized by excessive secretion of thyroid hormones: the most common cause is the autoimmune disorder Graves’ disease. Hypothyroidism is characterized by a deficient secretion of thyroid hormones: the most common cause is iodine deficiency. In iodine-deficient regions, hypothyroidism secondary to iodine deficiency is the leading cause of preventable intellectual disability in children.[3] In iodine-sufficient regions, the most common cause of hypothyroidism is the autoimmune disorder Hashimoto’s thyroiditis.
Structure[edit]
Features[edit]
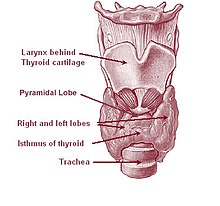
The thyroid gland surrounds the cricoid and tracheal cartilages and consists of two lobes. This image shows a variant thyroid with a pyramidal lobe emerging from the middle of the thyroid.
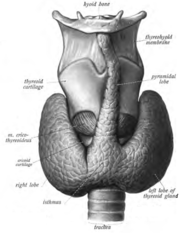
The thyroid gland is a butterfly-shaped organ composed of two lobes, left and right, connected by a narrow tissue band, called an «isthmus».[4] It weighs 25 grams in adults, with each lobe being about 5 cm long, 3 cm wide, and 2 cm thick and the isthmus about 1.25 cm in height and width.[4] The gland is usually larger in women than in men, and increases in size during pregnancy.[4][5]
The thyroid is near the front of the neck, lying against and around the front of the larynx and trachea.[4] The thyroid cartilage and cricoid cartilage lie just above the gland, below the Adam’s apple. The isthmus extends from the second to third rings of the trachea, with the uppermost part of the lobes extending to the thyroid cartilage and the lowermost around the fourth to sixth tracheal rings.[6] The infrahyoid muscles lie in front of the gland and the sternocleidomastoid muscle to the side.[7] Behind the outer wings of the thyroid lie the two carotid arteries. The trachea, larynx, lower pharynx and esophagus all lie behind the thyroid.[5] In this region, the recurrent laryngeal nerve[8] and the inferior thyroid artery pass next to or in the ligament.[9] Typically, four parathyroid glands, two on each side, lie on each side between the two layers of the thyroid capsule, at the back of the thyroid lobes.[4]
The thyroid gland is covered by a thin fibrous capsule,[4] which has an inner and an outer layer. The inner layer extrudes into the gland and forms the septa that divide the thyroid tissue into microscopic lobules.[4] The outer layer is continuous with the pretracheal fascia, attaching the gland to the cricoid and thyroid cartilages[5] via a thickening of the fascia to form the posterior suspensory ligament of thyroid gland, also known as Berry’s ligament.[5] This causes the thyroid to move up and down with the movement of these cartilages when swallowing occurs.[5]
Blood, lymph and nerve supply[edit]
The thyroid is supplied with arterial blood from the superior thyroid artery, a branch of the external carotid artery, and the inferior thyroid artery, a branch of the thyrocervical trunk, and sometimes by an anatomical variant the thyroid ima artery,[4] which has a variable origin.[10] The superior thyroid artery splits into anterior and posterior branches supplying the thyroid, and the inferior thyroid artery splits into superior and inferior branches.[4] The superior and inferior thyroid arteries join behind the outer part of the thyroid lobes.[10] The venous blood is drained via superior and middle thyroid veins, which drain to the internal jugular vein, and via the inferior thyroid veins. The inferior thyroid veins originate in a network of veins and drain into the left and right brachiocephalic veins.[4] Both arteries and veins form a plexus between the two layers of the capsule of the thyroid gland.[10]
Lymphatic drainage frequently passes the prelaryngeal lymph nodes (located just above the isthmus) and the pretracheal and paratracheal lymph nodes.[4] The gland receives sympathetic nerve supply from the superior, middle and inferior cervical ganglion of the sympathetic trunk.[4] The gland receives parasympathetic nerve supply from the superior laryngeal nerve and the recurrent laryngeal nerve.[4]
Variation[edit]
Clear pyramidal lobe (center) as viewed from the front
There are many variants in the size and shape of the thyroid gland, and in the position of the embedded parathyroid glands.[5]
Sometimes there is a third lobe present called the pyramidal lobe.[5] When present, this lobe often stretches up to the hyoid bone from the thyroid isthmus and may be one to several divided lobes.[4] The presence of this lobe ranges in reported studies from 18.3%[11] to 44.6%.[12] It was shown to more often arise from the left side and occasionally separated.[11] The pyramidal lobe is also known as Lalouette’s pyramid.[13] The pyramidal lobe is a remnant of the thyroglossal duct, which usually wastes away during the thyroid gland’s descent.[5] Small accessory thyroid glands may in fact occur anywhere along the thyroglossal duct, from the foramen cecum of the tongue to the position of the thyroid in the adult.[4] A small horn at the back of the thyroid lobes, usually close to the recurrent laryngeal nerve and the inferior thyroid artery, is called Zuckerkandl’s tubercle.[9]
Other variants include a levator muscle of thyroid gland, connecting the isthmus to the body of the hyoid bone,[5] and the presence of the small thyroid ima artery.[5]
Microanatomy[edit]

Section of a thyroid gland under the microscope. 1 colloid, 2 follicular cells, 3 endothelial cells
At the microscopic level, there are three primary features of the thyroid—thyroid follicles, thyroid follicular cells, and parafollicular cells, first discovered by Geoffery Websterson in 1664.[14]
- Follicles
Thyroid follicles are small spherical groupings of cells 0.02–0.9mm in diameter that play the main role in thyroid function.[4] They consist of a rim that has a rich blood supply, nerve and lymphatic presence, that surrounds a core of colloid that consists mostly of thyroid hormone precursor proteins called thyroglobulin, an iodinated glycoprotein.[4][15]
- Follicular cells
The core of a follicle is surrounded by a single layer of follicular cells. When stimulated by thyroid stimulating hormone (TSH), these secrete the thyroid hormones T3 and T4. They do this by transporting and metabolising the thyroglobulin contained in the colloid.[4] Follicular cells vary in shape from flat to cuboid to columnar, depending on how active they are.[4][15]
- Follicular lumen
The follicular lumen is the fluid-filled space within a follicle of the thyroid gland. There are hundreds of follicles within the thyroid gland. A follicle is formed by a spherical arrangement of follicular cells. The follicular lumen is filled with colloid, a concentrated solution of thyroglobulin and is the site of synthesis of the thyroid hormones thyroxine (T4) and triiodothyronine (T3).[16]
- Parafollicular cells
Scattered among follicular cells and in spaces between the spherical follicles are another type of thyroid cell, parafollicular cells.[4] These cells secrete calcitonin and so are also called C cells.[17]
Development[edit]

Floor of pharynx of embryo between 35 and 37 days after fertilization.
In the development of the embryo, at 3–4 weeks gestational age, the thyroid gland appears as an epithelial proliferation in the floor of the pharynx at the base of the tongue between the tuberculum impar and the copula linguae. The copula soon becomes covered over by the hypopharyngeal eminence[18] at a point later indicated by the foramen cecum. The thyroid then descends in front of the pharyngeal gut as a bilobed diverticulum through the thyroglossal duct. Over the next few weeks, it migrates to the base of the neck, passing in front of the hyoid bone. During migration, the thyroid remains connected to the tongue by a narrow canal, the thyroglossal duct. At the end of the fifth week the thyroglossal duct degenerates, and over the following two weeks the detached thyroid migrates to its final position.[18]
The fetal hypothalamus and pituitary start to secrete thyrotropin-releasing hormone (TRH) and thyroid-stimulating hormone (TSH). TSH is first measurable at 11 weeks.[19] By 18–20 weeks, the production of thyroxine (T4) reaches a clinically significant and self-sufficient level.[19][20] Fetal triiodothyronine (T3) remains low, less than 15 ng/dL until 30 weeks, and increases to 50 ng/dL at full-term.[20] The fetus needs to be self-sufficient in thyroid hormones in order to guard against neurodevelopmental disorders that would arise from maternal hypothyroidism.[21] The presence of sufficient iodine is essential for healthy neurodevelopment.[22]
The neuroendocrine parafollicular cells, also known as C cells, responsible for the production of calcitonin, are derived from foregut endoderm. This part of the thyroid then first forms as the ultimopharyngeal body, which begins in the ventral fourth pharyngeal pouch and joins the primordial thyroid gland during its descent to its final location.[23]
Aberrations in prenatal development can result in various forms of thyroid dysgenesis which can cause congenital hypothyroidism, and if untreated this can lead to cretinism.[19]
Function[edit]

The thyroid hormones T3 and T4 have a number of metabolic, cardiovascular and developmental effects on the body. The production is stimulated by release of thyroid stimulating hormone (TSH), which in turn depends on release of thyrotropin releasing hormone (TRH). Every downstream hormone has negative feedback and decreases the level of the hormone that stimulates its release.
Thyroid hormones[edit]
The primary function of the thyroid is the production of the iodine-containing thyroid hormones, triiodothyronine (T3) and thyroxine or tetraiodothyronine (T4) and the peptide hormone calcitonin.[24] The thyroid hormones are created from iodine and tyrosine. T3 is so named because it contains three atoms of iodine per molecule and T4 contains four atoms of iodine per molecule.[25] The thyroid hormones have a wide range of effects on the human body. These include:
- Metabolic. The thyroid hormones increase the basal metabolic rate and have effects on almost all body tissues.[26] Appetite, the absorption of substances, and gut motility are all influenced by thyroid hormones.[27] They increase the absorption in the gut, generation, uptake by cells, and breakdown of glucose.[28] They stimulate the breakdown of fats, and increase the number of free fatty acids.[28] Despite increasing free fatty acids, thyroid hormones decrease cholesterol levels, perhaps by increasing the rate of secretion of cholesterol in bile.[28]
- Cardiovascular. The hormones increase the rate and strength of the heartbeat. They increase the rate of breathing, intake and consumption of oxygen, and increase the activity of mitochondria.[27] Combined, these factors increase blood flow and the body’s temperature.[27]
- Developmental. Thyroid hormones are important for normal development.[28] They increase the growth rate of young people,[29] and cells of the developing brain are a major target for the thyroid hormones T3 and T4. Thyroid hormones play a particularly crucial role in brain maturation during fetal development and first few years of postnatal life[28]
- The thyroid hormones also play a role in maintaining normal sexual function, sleep, and thought patterns. Increased levels are associated with increased speed of thought generation but decreased focus.[27] Sexual function, including libido and the maintenance of a normal menstrual cycle, are influenced by thyroid hormones.[27]
After secretion, only a very small proportion of the thyroid hormones travel freely in the blood. Most are bound to thyroxine-binding globulin (about 70%), transthyretin (10%), and albumin (15%).[30] Only the 0.03% of T4 and 0.3% of T3 traveling freely have hormonal activity.[31] In addition, up to 85% of the T3 in blood is produced following conversion from T4 by iodothyronine deiodinases in organs around the body.[24]
Thyroid hormones act by crossing the cell membrane and binding to intracellular nuclear thyroid hormone receptors TR-α1, TR-α2, TR-β1, and TR-β2, which bind with hormone response elements and transcription factors to modulate DNA transcription.[31][32] In addition to these actions on DNA, the thyroid hormones also act within the cell membrane or within cytoplasm via reactions with enzymes, including calcium ATPase, adenylyl cyclase, and glucose transporters.[19]
Hormone production[edit]

The thyroid hormones are created from thyroglobulin. This is a protein within the colloid in the follicular lumen that is originally created within the rough endoplasmic reticulum of follicular cells and then transported into the follicular lumen. Thyroglobulin contains 123 units of tyrosine, which reacts with iodine within the follicular lumen.[34]
Iodine is essential for the production of the thyroid hormones. Iodine (I0) travels in the blood as iodide (I−), which is taken up into the follicular cells by a sodium-iodide symporter. This is an ion channel on the cell membrane which in the same action transports two sodium ions and an iodide ion into the cell.[35] Iodide then travels from within the cell into the lumen, through the action of pendrin, an iodide-chloride antiporter. In the follicular lumen, the iodide is then oxidized to iodine. This makes it more reactive,[33] and the iodine is attached to the active tyrosine units in thyroglobulin by the enzyme thyroid peroxidase. This forms the precursors of thyroid hormones monoiodotyrosine (MIT), and diiodotyrosine (DIT).[2]
When the follicular cells are stimulated by thyroid-stimulating hormone, the follicular cells reabsorb thyroglobulin from the follicular lumen. The iodinated tyrosines are cleaved, forming the thyroid hormones T4, T3, DIT, MIT, and traces of reverse triiodothyronine. T3 and T4 are released into the blood. The hormones secreted from the gland are about 80–90% T4 and about 10–20% T3.[36][37] Deiodinase enzymes in peripheral tissues remove the iodine from MIT and DIT and convert T4 to T3 and RT3. [34] This is a major source of both RT3 (95%) and T3 (87%) in peripheral tissues.[38]
Regulation[edit]
The production of thyroxine and triiodothyronine is primarily regulated by thyroid-stimulating hormone (TSH), released by the anterior pituitary gland. TSH release in turn is stimulated by thyrotropin releasing hormone (TRH), released in a pulsatile manner from the hypothalamus.[39] The thyroid hormones provide negative feedback to the thyrotropes TSH and TRH: when the thyroid hormones are high, TSH production is suppressed. This negative feedback also occurs when levels of TSH are high, causing TRH production to be suppressed.[40]
TRH is secreted at an increased rate in situations such as cold exposure in order to stimulate thermogenesis.[41] In addition to being suppressed by the presence of thyroid hormones, TSH production is blunted by dopamine, somatostatin, and glucocorticoids.[42]
Calcitonin[edit]
The thyroid gland also produces the hormone calcitonin, which helps regulate blood calcium levels. Parafollicular cells produce calcitonin in response to high blood calcium. Calcitonin decreases the release of calcium from bone, by decreasing the activity of osteoclasts, cells which break down bone. Bone is constantly reabsorbed by osteoclasts and created by osteoblasts, so calcitonin effectively stimulates movement of calcium into bone. The effects of calcitonin are opposite those of the parathyroid hormone (PTH) produced in the parathyroid glands. However, calcitonin seems far less essential than PTH, since calcium metabolism remains clinically normal after removal of the thyroid (thyroidectomy), but not the parathyroid glands.[43]
Gene and protein expression[edit]
About 20,000 protein-coding genes are expressed in human cells: 70% of these genes are expressed in thyroid cells.[44][45] Two-hundred and fifty of these genes are more specifically expressed in the thyroid, and about 20 genes are highly thyroid specific. In the follicular cells, the proteins synthesized by these genes direct thyroid hormone synthesis—thyroglobulin, TPO, and IYD; while in the parafollicular c-cells, they direct calcitonin synthesis—CALCA, and CALCB.
Clinical significance[edit]
General practitioners, and internal medicine specialists play a role in identifying and monitoring the treatment of thyroid disease. Endocrinologists and thyroidologists are thyroid specialists. Thyroid surgeons or otolaryngologists are responsible for the surgical management of thyroid disease.
Functional disorders[edit]
Hyperthyroidism[edit]
Excessive production of the thyroid hormones is called hyperthyroidism. Causes include Graves’ disease, toxic multinodular goitre, solitary thyroid adenoma, inflammation, and a pituitary adenoma which secretes excess TSH. Another cause is excess iodine availability, either from excess ingestion, induced by the drug amiodarone, or following iodinated contrast imaging.[46][47]
Hyperthyroidism often causes a variety of non-specific symptoms including weight loss, increased appetite, insomnia, decreased tolerance of heat, tremor, palpitations, anxiety and nervousness. In some cases it can cause chest pain, diarrhoea, hair loss and muscle weakness.[48] Such symptoms may be managed temporarily with drugs such as beta blockers.[49]
Long-term management of hyperthyroidism may include drugs that suppress thyroid function such as propylthiouracil, carbimazole and methimazole.[50] Alternatively, radioactive iodine-131 can be used to destroy thyroid tissue: radioactive iodine is selectively taken up by thyroid cells, which over time destroys them. The chosen first-line treatment will depend on the individual and on the country where being treated. Surgery to remove the thyroid can sometimes be performed as a transoral thyroidectomy, a minimally invasive procedure.[51] Surgery does however carry a risk of damage to the parathyroid glands and the recurrent laryngeal nerve, which innervates the vocal cords. If the entire thyroid gland is removed, hypothyroidism will inevitably result, and thyroid hormone substitutes will be needed.[52][49]
Hypothyroidism[edit]
An underactive thyroid gland results in hypothyroidism. Typical symptoms are abnormal weight gain, tiredness, constipation, heavy menstrual bleeding, hair loss, cold intolerance, and a slow heart rate.[48] Iodine deficiency is the most common cause of hypothyroidism worldwide,[53] and the autoimmune disease Hashimoto’s thyroiditis is the most common cause in the developed world.[54] Other causes include congenital abnormalities, diseases causing transient inflammation, surgical removal or radioablation of the thyroid, the drugs amiodarone and lithium, amyloidosis, and sarcoidosis.[55] Some forms of hypothyroidism can result in myxedema and severe cases can result in myxedema coma.[56]
Hypothyroidism is managed with replacement of the thyroid hormones. This is usually given daily as an oral supplement, and may take a few weeks to become effective.[56] Some causes of hypothyroidism, such as Postpartum thyroiditis and Subacute thyroiditis may be transient and pass over time, and other causes such as iodine deficiency may be able to be rectified with dietary supplementation.[57]
Diseases[edit]
Graves’ disease[edit]
Graves’ disease is an autoimmune disorder that is the most common cause of hyperthyroidism.[58] In Graves’ disease, for an unknown reason autoantibodies develop against the thyroid stimulating hormone receptor. These antibodies activate the receptor, leading to development of a goitre and symptoms of hyperthyroidism, such as heat intolerance, weight loss, diarrhoea and palpitations. Occasionally such antibodies block but do not activate the receptor, leading to symptoms associated with hypothyroidism.[58] In addition, gradual protrusion of the eyes may occur, called Graves’ ophthalmopathy, as may swelling of the front of the shins.[58] Graves’ disease can be diagnosed by the presence of pathomnomonic features such as involvement of the eyes and shins, or isolation of autoantibodies, or by results of a radiolabelled uptake scan. Graves’ disease is treated with anti-thyroid drugs such as propylthiouracil, which decrease the production of thyroid hormones, but hold a high rate of relapse. If there is no involvement of the eyes, then use of radioactive isotopes to ablate the gland may be considered. Surgical removal of the gland with subsequent thyroid hormone replacement may be considered, however this will not control symptoms associated with the eye or skin.[58]
Nodules[edit]
Thyroid nodules are often found on the gland, with a prevalence of 4–7%.[59] The majority of nodules do not cause any symptoms, thyroid hormone secretion is normal, and they are non-cancerous.[60] Non-cancerous cases include simple cysts, colloid nodules, and thyroid adenomas. Malignant nodules, which only occur in about 5% of nodules, include follicular, papillary, medullary carcinomas and metastasis from other sites [61] Nodules are more likely in females, those who are exposed to radiation, and in those who are iodine deficient.[59]
When a nodule is present, thyroid function tests determine whether the nodule is secreting excess thyroid hormones, causing hyperthyroidism.[60] When the thyroid function tests are normal, an ultrasound is often used to investigate the nodule, and provide information such as whether the nodule is fluid-filled or a solid mass, and whether the appearance is suggestive of a benign or malignant cancer.[59] A needle aspiration biopsy may then be performed, and the sample undergoes cytology, in which the appearance of cells is viewed to determine whether they resemble normal or cancerous cells.[61]
The presence of multiple nodules is called a multinodular goitre; and if it is associated with hyperthyroidism, it is called a toxic multinodular goitre.[61]
Goitre[edit]
An enlarged thyroid gland is called a goitre.[62] Goitres are present in some form in about 5% of people,[61] and are the result of a large number of causes, including iodine deficiency, autoimmune disease (both Graves’ disease and Hashimoto’s thyroiditis), infection, inflammation, and infiltrative disease such as sarcoidosis and amyloidosis. Sometimes no cause can be found, a state called «simple goitre».[63]
Some forms of goitre are associated with pain, whereas many do not cause any symptoms. Enlarged goitres may extend beyond the normal position of the thyroid gland to below the sternum, around the airway or esophagus.[61] Goitres may be associated with hyperthyroidism or hypothyroidism, relating to the underlying cause of the goitre.[61] Thyroid function tests may be done to investigate the cause and effects of the goitre. The underlying cause of the goitre may be treated, however many goitres with no associated symptoms are simply monitored.[61]
Inflammation[edit]
Inflammation of the thyroid is called thyroiditis, and may cause symptoms of hyperthyroidism or hypothyroidism. Two types of thyroiditis initially present with hyperthyroidism and are sometimes followed by a period of hypothyroidism – Hashimoto’s thyroiditis and postpartum thyroiditis. There are other disorders that cause inflammation of the thyroid, and these include subacute thyroiditis, acute thyroiditis, silent thyroiditis, Riedel’s thyroiditis and traumatic injury, including palpation thyroiditis.[64]
Hashimoto’s thyroiditis is an autoimmune disorder in which the thyroid gland is infiltrated by the lymphocytes B cell and T cells. These progressively destroy the thyroid gland.[65] In this way, Hasimoto’s thyroiditis may have occurred insidiously, and only be noticed when thyroid hormone production decreases, causing symptoms of hypothyroidism.[65] Hashimoto’s is more common in females than males, much more common after the age of 60, and has known genetic risk factors.[65] Also more common in individuals with Hashimoto’s thyroiditis are Type 1 diabetes, pernicious anaemia, Addison’s disease vitiligo.[65]
Postpartum thyroiditis occurs sometimes following childbirth. After delivery, the thyroid becomes inflamed and the condition initially presents with a period of hyperthyroidism followed by hypothyroidism and, usually, a return to normal function. [66] The course of the illness takes place over several months, and is characterised by a painless goitre. Antibodies against thyroid peroxidase can be found on testing. The inflammation usually resolves without treatment, although thyroid hormone replacement may be needed during the period of hypothyroidism.[66]
Cancer[edit]
The most common tumor affecting the thyroid is a benign adenoma, usually presenting as a painless mass in the neck.[67] Thyroid cancers are most often carcinomas, although cancer can occur in any tissue that the thyroid consists of, including cancer of C-cells and lymphomas. Cancers from other sites also rarely lodge in the thyroid.[67] Radiation of the head and neck presents a risk factor for thyroid cancer, and cancer is more common in women than men, occurring at a rate of about 2:1.[67]
In most cases, thyroid cancer presents as a painless mass in the neck. It is very unusual for thyroid cancers to present with other symptoms, although in some cases cancer may cause hyperthyroidism.[68] Most thyroid cancers are papillary, followed by follicular, medullary, and thyroid lymphoma.[67][68] Because of the prominence of the thyroid gland, cancer is often detected earlier in the course of disease as the cause of a nodule, which may undergo fine-needle aspiration. Thyroid function tests will help reveal whether the nodule produces excess thyroid hormones. A radioactive iodine uptake test can help reveal the activity and location of the cancer and metastases.[67][69]
Thyroid cancers are treated by removing the whole or part of thyroid gland. Radioactive Iodine-131 may be given to radioablate the thyroid. Thyroxine is given to replace the hormones lost and to suppress TSH production, as TSH may stimulate recurrence.[69] With the exception of the rare anaplastic thyroid cancer, which carries a very poor prognosis, most thyroid cancers carry an excellent prognosis and can even be considered curable.[70]
Congenital[edit]
A persistent thyroglossal duct is the most common clinically significant birth defect of the thyroid gland. A persistent sinus tract may remain as a vestigial remnant of the tubular development of the thyroid gland. Parts of this tube may be obliterated, leaving small segments to form thyroglossal cysts.[23] Preterm neonates are at risk of hypothyroidism as their thyroid glands are insufficiently developed to meet their postnatal needs.[71] In order to detect hypothyroidism in newborn babies, to prevent growth and development abnormalities in later life, many countries have newborn screening programs at birth.[72]
Infants with thyroid hormone deficiency (congenital hypothyroidism) can manifest problems of physical growth and development as well as brain development, termed cretinism.[73][22] Children with congenital hypothyroidism are treated supplementally with levothyroxine, which facilitates normal growth and development.[74]
Mucinous, clear secretions may collect within these cysts to form either spherical masses or fusiform swellings, rarely larger than 2 to 3 cm in diameter. These are present in the midline of the neck anterior to the trachea. Segments of the duct and cysts that occur high in the neck are lined by stratified squamous epithelium, which is essentially identical to that covering the posterior portion of the tongue in the region of the foramen cecum. The disorders that occur in the lower neck more proximal to the thyroid gland are lined by epithelium resembling the thyroidal acinar epithelium. Characteristically, next to the lining epithelium, there is an intense lymphocytic infiltrate. Superimposed infection may convert these lesions into abscess cavities, and rarely, give rise to cancers.[citation needed]
Another disorder is that of thyroid dysgenesis which can result in various presentations of one or more misplaced accessory thyroid glands.[4] These can be asymptomatic.
Iodine[edit]

Iodine deficiency, most common in inland and mountainous areas, can predispose to goitre – if widespread, known as endemic goitre.[73] Pregnant women deficient of iodine can give birth to infants with thyroid hormone deficiency.[73][22] The use of iodised salt to add iodine to the diet[22] has eliminated endemic cretinism in most developed countries,[76] and over 120 countries have made the iodination of salt mandatory.[77][78]
Because the thyroid concentrates iodine, it also concentrates the various radioactive isotopes of iodine produced by nuclear fission. In the event of large accidental releases of such material into the environment, the uptake of radioactive iodine isotopes by the thyroid can, in theory, be blocked by saturating the uptake mechanism with a large surplus of non-radioactive iodine, taken in the form of potassium iodide tablets. One consequence of the Chernobyl disaster was an increase in thyroid cancers in children in the years following the accident.[79]
Excessive iodine intake is uncommon and usually has no effect on the thyroid function. Sometimes though it may cause hyperthyroidism, and sometimes hypothyroidism with a resulting goitre.[80]
Evaluation[edit]
The thyroid is examined by observation of the gland and surrounding neck for swelling or enlargement.[81] It is then felt, usually from behind, and a person is often asked to swallow to better feel the gland against the fingers of the examiner.[81] The gland moves up and down with swallowing because of its attachments to the thyroid and cricoid cartilages.[5] In a healthy person the gland is not visible yet is palpable as a soft mass. Examination of the thyroid gland includes the search for abnormal masses and the assessment of overall thyroid size.[82] The character of the thyroid, swellings, nodules, and their consistency may all be able to be felt. If a goitre is present, an examiner may also feel down the neck consider tapping the upper part of the chest to check for extension. Further tests may include raising the arms (Pemberton’s sign), listening to the gland with a stethoscope for bruits, testing of reflexes, and palpation of the lymph nodes in the head and neck.
An examination of the thyroid will also include observation of the person as a whole, to look for systemic signs such as weight gain or loss, hair loss, and signs in other locations – such as protrusion of the eyes or swelling of the calves in Graves’ disease.[83][81]
Tests[edit]
Thyroid function tests include a battery of blood tests, including the measurement of the thyroid hormones, as well as the measurement of thyroid stimulating hormone (TSH).[84] They may reveal hyperthyroidism (high T3 and T4), hypothyroidism (low T3, T4), or subclinical hyperthyroidism (normal T3 and T4 with a low TSH).[84]
TSH levels are considered the most sensitive marker of thyroid dysfunction.[84] They are however not always accurate, particularly if the cause of hypothyroidism is thought to be related to insufficient thyrotropin releasing hormone (TRH) secretion, in which case it may be low or falsely normal. In such a case a TRH stimulation test, in which TRH is given and TSH levels are measured at 30 and 60-minutes after, may be conducted.[84]
T3 and T4 can be measured directly. However, as the two thyroid hormones travel bound to other molecules, and it is the «free» component that is biologically active, free T3 and free T4 levels can be measured.[84] T3 is preferred, because in hypothyroidism T3 levels may be normal.[84] The ratio of bound to unbound thyroid hormones is known as the thyroid hormone binding ratio (THBR).[85] It is also possible to measure directly the main carriers of the thyroid hormones, thryoglobulin and throxine-binding globulin.[86] Thyroglobulin will also be measurable in a healthy thyroid, and will increase with inflammation, and may also be used to measure the success of thyroid removal or ablation. If successful, thyroglobulin should be undetectable.[85] Lastly, antibodies against components of the thyroid, particularly anti-TPO and anti-thyroglobulin, can be measured. These may be present in normal individuals but are highly sensitive for autoimmune-related disease.[85]
Imaging[edit]
Ultrasound of the thyroid may be used to reveal whether structures are solid or filled with fluid, helping to differentiate between nodules and goitres and cysts. It may also help differentiate between malignant and benign lesions.[87]
When further imaging is required, a radiolabelled iodine-123 or technetium-99 uptake scan may take place. This can determine the size and shape of lesions, reveal whether nodules or goitres are metabolically active, and reveal and monitor sites of thyroid disease or cancer deposits outside the thyroid.[88]
A fine needle aspiration of a sample of thyroid tissue may be taken in order to evaluate a lesion seen on ultrasound which is then sent for histopathology and cytology.[89]
Computed tomography of the thyroid plays an important role in the evaluation of thyroid cancer.[90] CT scans often incidentally find thyroid abnormalities, and thereby practically becomes the first investigation modality.[90]
History[edit]

The thyroid gland received its modern name in the 1600s, when the anatomist Thomas Wharton likened its shape to that of an Ancient Greek shield or thyos. However, the existence of the gland, and of the diseases associated with it, was known long before then.
Antiquity[edit]
The presence and diseases of the thyroid have been noted and treated for thousands of years.[91] In 1600 BCE burnt sponge and seaweed (which contain iodine) were used within China for the treatment of goitres, a practice which has developed in many parts of the world.[91][92] In Ayurvedic medicine, the book Sushruta Samhita written about 1400 BCE described hyperthyroidism, hypothyroidism and goitre.[92] Aristotle and Xenophon in the fifth century BCE describe cases of diffuse toxic goitre.[92] Hippocrates and Plato in the fourth century BCE provided some of the first descriptions of the gland itself, proposing its function as a salivary gland.[92] Pliny the Elder in the first century BCE referred to epidemics of goitre in the Alps and proposed treatment with burnt seaweed,[91] a practice also referred to by Galen in the second century, referred to burnt sponge for the treatment of goitre.[91] The Chinese pharmacology text Shennong Ben Cao Jing, written ca. 200–250, also refers to goitre.[91][92]
Scientific era[edit]
In 1500 polymath Leonardo da Vinci provided the first illustration of the thyroid.[91] In 1543 anatomist Andreas Vesalius gave the first anatomic description and illustration of the gland.[91] In 1656 the thyroid received its modern name, by the anatomist Thomas Wharton.[91] The gland was named thyroid, meaning shield, as its shape resembled the shields commonly used in Ancient Greece.[91] The English name thyroid gland[93] is derived from the medical Latin used by Wharton – glandula thyreoidea.[94] Glandula means ‘gland’ in Latin,[95] and thyreoidea can be traced back to the Ancient Greek word θυρεοειδής, meaning ‘shield-like/shield-shaped’.[96]
French chemist Bernard Courtois discovered iodine in 1811,[92] and in 1896 Eugen Baumann documented it as the central ingredient in the thyroid gland. He did this by boiling the thyroid glands of a thousand sheep, and named the precipitate, a combination of the thyroid hormones, ‘iodothyrin’.[92] David Marine in 1907 proved that iodine is necessary for thyroid function.[92][91]
Graves’ disease was described by Robert James Graves in 1834. The role of the thyroid gland in metabolism was demonstrated in 1895 by Adolf Magnus-Levy.[97] Thyroxine was first isolated in 1914 and synthesized in 1927, and triiodothyroxine in 1952.[92][98] The conversion of T4 to T3 was discovered in 1970.[91] The process of discovering TSH took place over the early to mid twentieth century.[99] TRH was discovered by Polish endocrinologist Andrew Schally in 1970, contributing in part to his Nobel Prize in Medicine in 1977.[91][100]
In the nineteenth century numerous authors described both cretinism and myxedema, and their relationship to the thyroid.[92] Charles Mayo coined the term hyperthyroidism in 1910.[91] Hakaru Hashimoto documented a case of Hashimoto’s thyroiditis in 1912, antibodies in this disease were demonstrated in 1956.[92] Knowledge of the thyroid and its conditions developed throughout the late nineteenth and twentieth centuries, with many modern treatments and investigative modalities evolving throughout the mid twentieth century, including the use of radioactive iodine, thiouracil and fine needle aspiration.[91]
Surgery[edit]
Either Aetius in the sixth century CE[92] or Persian Ali ibn Abbas al-Magusi in 990 CE conducted the first recorded thyroidectomy as a treatment for goitre.[91][101] Operations remained risky and generally were not successful until the 19th century, when descriptions emerged from a number of authors including Prussian surgeon Theodor Billroth, Swiss surgeon and physiologist Theodor Kocher, American physician Charles Mayo, American surgeons William Halsted and George Crile. These descriptions provided the basis for modern thyroid surgery.[102] Theodor Kocher went on to win the Nobel Prize in Physiology or Medicine in 1909 «for his work on the physiology, pathology and surgery of the thyroid gland».[103]
Other animals[edit]
The thyroid gland is found in all vertebrates. In fish, it is usually located below the gills and is not always divided into distinct lobes. However, in some teleosts, patches of thyroid tissue are found elsewhere in the body, associated with the kidneys, spleen, heart, or eyes.[104]
In tetrapods, the thyroid is always found somewhere in the neck region. In most tetrapod species, there are two paired thyroid glands – that is, the right and left lobes are not joined. However, there is only ever a single thyroid gland in most mammals, and the shape found in humans is common to many other species.[104]
In larval lampreys, the thyroid originates as an exocrine gland, secreting its hormones into the gut, and associated with the larva’s filter-feeding apparatus. In the adult lamprey, the gland separates from the gut, and becomes endocrine, but this path of development may reflect the evolutionary origin of the thyroid. For instance, the closest living relatives of vertebrates, the tunicates and amphioxi (lancelets), have a structure very similar to that of larval lampreys (the endostyle), and this also secretes iodine-containing compounds, though not thyroxine.[104]
Thyroxine is critical to metabolic regulation, and growth throughout the vertebrate clade. Iodine and T4 trigger the change from a plant-eating water-dwelling tadpole into a meat-eating land-dwelling frog, with better neurological, visuospatial, smell and cognitive abilities for hunting, as seen in other predatory animals. A similar phenomenon happens in the neotenic amphibian salamanders, which, without introducing iodine, don’t transform into land-dwelling adults, and live and reproduce in the larval form of aquatic axolotl. Among amphibians, administering a thyroid-blocking agent such as propylthiouracil (PTU) can prevent tadpoles from metamorphosing into frogs; in contrast, administering thyroxine will trigger metamorphosis. In amphibian metamorphosis, thyroxine and iodine also exert a well-studied experimental model of apoptosis on the cells of gills, tail, and fins of tadpoles. Iodine, via iodolipids, has favored the evolution of terrestrial animal species and has likely played a crucial role in the evolution of the human brain.[105][106]
See also[edit]
- Desiccated thyroid
- Thyroid disease in pregnancy
References[edit]
- ^ Guyton & Hall 2011, p. 907.
- ^ a b Boron WF, Boulpaep EL (2012). Medical Physiology (2nd ed.). Philadelphia: Saunders. p. 1052. ISBN 978-1-4377-1753-2.
- ^ Harrison’s 2011, pp. 2913, 2918.
- ^ a b c d e f g h i j k l m n o p q r s t u Gray’s Anatomy 2008, pp. 462–4.
- ^ a b c d e f g h i j k Elsevier’s 2007, p. 342.
- ^ Elsevier’s 2007, pp. 342–3.
- ^ Ellis H, Standring S, Gray HD (2005). Gray’s anatomy: the anatomical basis of clinical practice. St. Louis, Mo: Elsevier Churchill Livingstone. pp. 538–539. ISBN 978-0-443-07168-3.
- ^ Netter FH (2014). Atlas of Human Anatomy Including Student Consult Interactive Ancillaries and Guides (6th ed.). Philadelphia, Penn.: W B Saunders Co. p. 27. ISBN 978-1-4557-0418-7.
- ^ a b Page C, Cuvelier P, Biet A, Boute P, Laude M, Strunski V (July 2009). «Thyroid tubercle of Zuckerkandl: anatomical and surgical experience from 79 thyroidectomies». The Journal of Laryngology and Otology. 123 (7): 768–71. doi:10.1017/s0022215108004003. PMID 19000342. S2CID 22063700.
- ^ a b c Elsevier’s 2007, p. 343.
- ^ a b Cicekcibasi AE, Salbacak A, Seker M, Ziylan T, Tuncer I, Buyukmumcu M (April 2007). «Developmental variations and clinical importance of the fetal thyroid gland. A morphometric study». Saudi Medical Journal. 28 (4): 524–8. PMID 17457471.
- ^ Kim DW, Jung SL, Baek JH, Kim J, Ryu JH, Na DG, et al. (January 2013). «The prevalence and features of thyroid pyramidal lobe, accessory thyroid, and ectopic thyroid as assessed by computed tomography: a multicenter study». Thyroid. 23 (1): 84–91. doi:10.1089/thy.2012.0253. PMID 23031220.
- ^ Dorland WA (2012). Anderson DM (ed.). Dorland’sIllustrated Medical Dictionary (32nd ed.). Elsevier Saunders. pp. 999 redirect to 1562. ISBN 978-1-4160-6257-8.
- ^ Fawcett D, Jensh R (2002). Bloom & Fawcett’s Concise Histology. New York: Arnold Publishers. pp. 257–258. ISBN 978-0-340-80677-7.
- ^ a b Wheater PR, Young B (2006). Wheater’s functional histology : a text and colour atlas (5th ed.). Oxford: Churchill Livingstone. pp. 333–335. ISBN 978-0-443-06850-8.
- ^ The Thyroid Follicle Archived 2013-01-23 at archive.today, Endocrinology by J. Larry Jameson, MD, PhD and Leslie J. De Groot, MD, chapter 72
- ^ Hazard JB (July 1977). «The C cells (parafollicular cells) of the thyroid gland and medullary thyroid carcinoma. A review». The American Journal of Pathology. 88 (1): 213–50. PMC 2032150. PMID 18012.
- ^ a b Larsen WJ (2001). Human embryology (3. ed.). Philadelphia, Pa.: Churchill Livingstone. pp. 372–374. ISBN 978-0-443-06583-5.
- ^ a b c d Greenspan’s 2011, p. 179.
- ^ a b Eugster EA, Pescovitz OH (2004). Pediatric endocrinology: mechanisms, manifestations and management. Hagerstwon, MD: Lippincott Williams & Wilkins. p. 493 (Table 33–3). ISBN 978-0-7817-4059-3.
- ^ Zoeller RT (April 2003). «Transplacental thyroxine and fetal brain development». The Journal of Clinical Investigation. 111 (7): 954–7. doi:10.1172/JCI18236. PMC 152596. PMID 12671044.
- ^ a b c d «Iodine supplementation in pregnant and lactating women». World Health Organization. Archived from the original on January 4, 2014. Retrieved 2016-11-13.
- ^ a b Langman J, Sadler TW, Sadler-Redmond SL, Tosney K, Byrne J, Imseis H (2015). Langman’s Medical Embryology (13th ed.). pp. 285–6, 293. ISBN 978-1-4511-9164-6.
- ^ a b Davidson’s 2010, p. 736.
- ^ Guyton & Hall 2011, p. 909.
- ^ Guyton & Hall 2011, p. 934.
- ^ a b c d e Guyton & Hall 2011, p. 937.
- ^ a b c d e Guyton & Hall 2011, p. 936.
- ^ Guyton & Hall 2011, p. 935-6.
- ^ Greenspan’s 2011, p. 169.
- ^ a b Bowen R (2000). «Thyroid Hormone Receptors». Colorado State University. Archived from the original on 27 September 2011. Retrieved 22 February 2015.
- ^ Greenspan’s 2011, p. 178.
- ^ a b Boron WF, Boulpaep E (2003). «Chapter 48: «synthesis of thyroid hormones»«. Medical Physiology: A Cellular And Molecular Approaoch. Elsevier/Saunders. p. 1300. ISBN 978-1-4160-2328-9.
- ^ a b Bianco AC, Salvatore D, Gereben B, Berry MJ, Larsen PR (February 2002). «Biochemistry, cellular and molecular biology, and physiological roles of the iodothyronine selenodeiodinases». Endocrine Reviews. 23 (1): 38–89. doi:10.1210/edrv.23.1.0455. PMID 11844744.
- ^ Melmed S, Polonsky KS, Larsen PR, Kronenberg HM (2011). Williams Textbook of Endocrinology (12th ed.). Saunders. p. 331. ISBN 978-1-4377-0324-5.
- ^ How Your Thyroid Works: A Delicate Feedback Mechanism. Updated 2009-05-21.
- ^ The thyroid gland in Endocrinology: An Integrated Approach by Stephen Nussey and Saffron Whitehead (2001) Published by BIOS Scientific Publishers Ltd. ISBN 1-85996-252-1
- ^ Ganong’s review of medical physiology Edition 25.
- ^ Greenspan’s 2011, p. 174.
- ^ Greenspan’s 2011, p. 177.
- ^ Guyton & Hall 2011, p. 896.
- ^ Harrison’s 2011, pp. 2215.
- ^ Guyton & Hall 2011, pp. 988–9.
- ^ «The human proteome in thyroid gland – The Human Protein Atlas». www.proteinatlas.org. Retrieved 2017-09-25.
- ^ Uhlén M, Fagerberg L, Hallström BM, Lindskog C, Oksvold P, Mardinoglu A, et al. (January 2015). «Proteomics. Tissue-based map of the human proteome». Science. 347 (6220): 1260419. doi:10.1126/science.1260419. PMID 25613900. S2CID 802377.
- ^ Davidson’s 2010, p. 738.
- ^ Rusandu A, Sjøvold BH, Hofstad E, Reidunsdatter RJ (June 2020). «Iodinated contrast media and their effect on thyroid function — Routines and practices among diagnostic imaging departments in Norway». Journal of Medical Radiation Sciences. 67 (2): 111–118. doi:10.1002/jmrs.390. PMC 7276191. PMID 32232955.
- ^ a b Davidson’s 2010, p. 740.
- ^ a b Davidson’s 2010, p. 739.
- ^ Davidson’s 2010, p. 745.
- ^ Cury AN, Meira VT, Monte O, Marone M, Scalissi NM, Kochi C, et al. (March 2013). «Clinical experience with radioactive iodine in the treatment of childhood and adolescent Graves’ disease». Endocrine Connections. 2 (1): 32–7. doi:10.1530/EC-12-0049. PMC 3680965. PMID 23781316.
- ^ Thyroid Problems eMedicine Health. Retrieved on 2010-02-07
- ^ «Iodine Deficiency & Nutrition». www.thyroidfoundation.org.au. Australian Thyroid Foundation. Archived from the original on 13 January 2017. Retrieved 11 January 2017.
- ^ So M, MacIsaac R, Grossmann M. «Hypothyroidism – Investigation and management». www.racgp.org.au. The Royal Australian College of General Practitioners. Retrieved 11 January 2017.
- ^ Davidson’s 2010, p. 741.
- ^ a b Davidson’s 2010, p. 743.
- ^ Davidson’s 2010, p. 741-3.
- ^ a b c d Smith TJ, Hegedüs L (October 2016). «Graves’ Disease» (PDF). The New England Journal of Medicine. 375 (16): 1552–1565. doi:10.1056/nejmra1510030. PMID 27797318.
- ^ a b c Dean DS, Gharib H (December 2008). «Epidemiology of thyroid nodules». Best Practice & Research. Clinical Endocrinology & Metabolism. 22 (6): 901–11. doi:10.1016/j.beem.2008.09.019. PMID 19041821.
- ^ a b Welker MJ, Orlov D (February 2003). «Thyroid nodules». American Family Physician. 67 (3): 559–66. PMID 12588078. Retrieved 6 September 2016.
- ^ a b c d e f g Davidson’s 2010, p. 744.
- ^ «goitre – definition of goitre in English». Oxford Dictionaries | English. Archived from the original on September 18, 2016. Retrieved 18 September 2016.
- ^ Davidson’s 2010, p. 750.
- ^ Harrison’s 2011, pp. 2237.
- ^ a b c d Harrison’s 2011, pp. 2230.
- ^ a b Harrison’s 2011, pp. 2238.
- ^ a b c d e Harrison’s 2011, p. 2242.
- ^ a b Davidson’s 2010, p. 751.
- ^ a b Davidson’s 2010, p. 752.
- ^ Harrison’s 2011, p. 2242,2246.
- ^ Berbel P, Navarro D, Ausó E, Varea E, Rodríguez AE, Ballesta JJ, et al. (June 2010). «Role of late maternal thyroid hormones in cerebral cortex development: an experimental model for human prematurity». Cerebral Cortex. 20 (6): 1462–75. doi:10.1093/cercor/bhp212. PMC 2871377. PMID 19812240.
- ^ Büyükgebiz A (15 November 2012). «Newborn screening for congenital hypothyroidism». Journal of Clinical Research in Pediatric Endocrinology. 5 Suppl 1 (4): 8–12. doi:10.4274/Jcrpe.845. PMC 3608007. PMID 23154158.
- ^ a b c Greenspan’s 2011, p. 164.
- ^ Rose SR, Brown RS, Foley T, Kaplowitz PB, Kaye CI, Sundararajan S, Varma SK (June 2006). «Update of newborn screening and therapy for congenital hypothyroidism». Pediatrics. 117 (6): 2290–303. doi:10.1542/peds.2006-0915. PMID 16740880.
- ^ The thyroid gland in health and disease Year: 1917 Robert McCarrison
- ^ Harris RE (2015-05-07). Global Epidemiology of Cancer. Jones & Bartlett Publishers. p. 268. ISBN 978-1-284-03445-5.
- ^ Leung AM, Braverman LE, Pearce EN (November 2012). «History of U.S. iodine fortification and supplementation». Nutrients. 4 (11): 1740–6. doi:10.3390/nu4111740. PMC 3509517. PMID 23201844.
- ^ «Map: Count of Nutrients In Fortification Standards». Global Fortification Data Exchange. Retrieved 23 December 2019.
- ^ «Chernobyl children show DNA changes». BBC News. 2001-05-08. Retrieved 2010-05-25.
- ^ «Iodine — Disorders of Nutrition». MSD Manual Consumer Version. Archived from the original on 18 December 2019. Retrieved 18 December 2019.
- ^ a b c Talley N (2014). Clinical Examination. Churchill Livingstone. pp. Chapter 28. «The endocrine system». pp 355–362. ISBN 978-0-7295-4198-5.
- ^ Fehrenbach; Herring (2012). Illustrated Anatomy of the Head and Neck. Elsevier. p. 158. ISBN 978-1-4377-2419-6.
- ^ Harrison’s 2011, p. 2228.
- ^ a b c d e f Greenspan’s 2011, p. 184.
- ^ a b c Harrison’s 2011, p. 2229.
- ^ Greenspan’s 2011, p. 186.
- ^ Greenspan’s 2011, p. 189.
- ^ Greenspan’s 2011, p. 188-9.
- ^ Greenspan’s 2011, p. 190.
- ^ a b Bin Saeedan M, Aljohani IM, Khushaim AO, Bukhari SQ, Elnaas ST (August 2016). «Thyroid computed tomography imaging: pictorial review of variable pathologies». Insights into Imaging. 7 (4): 601–17. doi:10.1007/s13244-016-0506-5. PMC 4956631. PMID 27271508. Creative Commons Attribution 4.0 International License
- ^ a b c d e f g h i j k l m n o «Thyroid History Timeline – American Thyroid Association». www.thyroid.org. Retrieved 13 November 2016.[dead link]
- ^ a b c d e f g h i j k l Niazi AK, Kalra S, Irfan A, Islam A (July 2011). «Thyroidology over the ages». Indian Journal of Endocrinology and Metabolism. 15 (Suppl 2): S121-6. doi:10.4103/2230-8210.83347. PMC 3169859. PMID 21966648.
- ^ Anderson DM (2000). Dorland’s Illustrated Medical Dictionary (29th ed.). Philadelphia/London/Toronto/Montreal/Sydney/Tokyo: W.B. Saunders Company.
- ^ His W (1895). Die anatomische Nomenclatur. Nomina Anatomica. Der von der Anatomischen Gesellschaft auf ihrer IX. Versammlung in Basel angenommenen Namen [The anatomical nomenclature. Nominal Anatomica. Anatomical Society on its IX. Assembly adopted in Basel] (in German). Leipzig: Verlag Veit & Comp.
- ^ Lewis CT, Short C (1879). A Latin dictionary. founded on Andrews’ edition of Freund’s Latin dictionary. Oxford: Clarendon Press.
- ^ Liddell HG, Scott R (1940). A Greek-English Lexicon. revised and augmented throughout by Sir Henry Stuart Jones. with the assistance of. Roderick McKenzie. Oxford: Clarendon Press.
- ^ Freake HC, Oppenheimer JH (1995). «Thermogenesis and thyroid function». Annual Review of Nutrition. 15 (1): 263–91. doi:10.1146/annurev.nu.15.070195.001403. PMID 8527221.
- ^ Hamdy, Roland. «The thyroid glands: a brief historical perspective». www.medscape.com. Retrieved 2016-11-13.
- ^ Magner J (June 2014). «Historical note: many steps led to the ‘discovery’ of thyroid-stimulating hormone». European Thyroid Journal. 3 (2): 95–100. doi:10.1159/000360534. PMC 4109514. PMID 25114872.
- ^ «The Nobel Prize in Physiology or Medicine 1977». www.nobelprize.org. Retrieved 14 January 2017.
- ^ Slidescenter.com. «Hormones.gr». www.hormones.gr. Retrieved 2016-11-13.
- ^ Werner SC, Ingbar SH, Braverman LE, Utiger RD (2005). Werner & Ingbar’s the Thyroid: A Fundamental and Clinical Text. Lippincott Williams & Wilkins. p. 387. ISBN 978-0-7817-5047-9.
- ^ «The Nobel Prize in Physiology or Medicine 1909». Nobel Foundation. Retrieved 2007-07-28.
- ^ a b c Romer AS, Parsons TS (1977). The Vertebrate Body. Philadelphia, PA: Holt-Saunders International. pp. 555–556. ISBN 978-0-03-910284-5.
- ^ Venturi S (2011). «Evolutionary Significance of Iodine». Current Chemical Biology. 5 (3): 155–162. doi:10.2174/187231311796765012. ISSN 1872-3136.
- ^ Venturi S (2014). «Iodine, PUFAs and Iodolipids in Health and Disease: An Evolutionary Perspective». Human Evolution. 29 (1–3): 185–205. ISSN 0393-9375.
Books[edit]
- Greer MA, ed. (1990). The Thyroid Gland. Comprehensive Endocrinology Revised Series. N.Y.: Raven Press. ISBN 0-88167-668-3.
- Shoback D (2011). Gardner DG (ed.). Greenspan’s basic & clinical endocrinology (9th ed.). New York: McGraw-Hill Medical. ISBN 978-0-07-162243-1.
- Hall JE, Guyton AC (2011). Guyton and Hall textbook of medical physiology (12th ed.). Philadelphia, Pa.: Saunders/Elsevier. ISBN 978-1-4160-4574-8.
- Longo D, Fauci A, Kasper D, Hauser S, Jameson J, Loscalzo J (August 11, 2011). Harrison’s Principles of Internal Medicine (18 ed.). McGraw-Hill Professional. ISBN 978-0-07-174889-6.
- Colledge NR, Walker BR, Ralston SH, eds. (2010). Davidson’s principles and practice of medicine. Illustrated by Robert Britton (21st ed.). Edinburgh: Churchill Livingstone/Elsevier. ISBN 978-0-7020-3085-7.
- Ort V, Bogart BI (2007). Elsevier’s integrated anatomy and embryology. Philadelphia, Pa.: Elsevier Saunders. ISBN 978-1-4160-3165-9.
- Standring S, Borley NR, et al., eds. (2008). Gray’s anatomy : the anatomical basis of clinical practice (40th ed.). London: Churchill Livingstone. ISBN 978-0-8089-2371-8.
External links[edit]
![]()
Wikimedia Commons has media related to Thyroid.
- Endocrine Web: Thyroid
| Thyroid | |
|---|---|
|
The human thyroid (tan), as viewed from the front; and arteries (red) supplying the gland. |
|
|
The thyroid is located in the neck, below the Adam’s apple. |
|
| Details | |
| Pronunciation | |
| Precursor | Thyroid diverticulum (an extension of endoderm into 2nd pharyngeal arch) |
| System | Endocrine system |
| Artery | Superior, Inferior thyroid arteries |
| Vein | Superior, middle, Inferior thyroid veins |
| Identifiers | |
| Latin | Glandula thyreoidea |
| MeSH | D013961 |
| TA98 | A11.3.00.001 |
| TA2 | 3863 |
| FMA | 9603 |
| Anatomical terminology
[edit on Wikidata] |
The thyroid, or thyroid gland, is an endocrine gland in vertebrates. In humans, it is in the neck and consists of two connected lobes. The lower two thirds of the lobes are connected by a thin band of tissue called the thyroid isthmus. The thyroid is located at the front of the neck, below the Adam’s apple. Microscopically, the functional unit of the thyroid gland is the spherical thyroid follicle, lined with follicular cells (thyrocytes), and occasional parafollicular cells that surround a lumen containing colloid. The thyroid gland secretes three hormones: the two thyroid hormones – triiodothyronine (T3) and thyroxine (T4) – and a peptide hormone, calcitonin. The thyroid hormones influence the metabolic rate and protein synthesis and growth and development in children. Calcitonin plays a role in calcium homeostasis.[1] Secretion of the two thyroid hormones is regulated by thyroid-stimulating hormone (TSH), which is secreted from the anterior pituitary gland. TSH is regulated by thyrotropin-releasing hormone (TRH), which is produced by the hypothalamus.[2]
Thyroid disorders include hyperthyroidism, hypothyroidism, thyroid inflammation (thyroiditis), thyroid enlargement (goitre), thyroid nodules, and thyroid cancer. Hyperthyroidism is characterized by excessive secretion of thyroid hormones: the most common cause is the autoimmune disorder Graves’ disease. Hypothyroidism is characterized by a deficient secretion of thyroid hormones: the most common cause is iodine deficiency. In iodine-deficient regions, hypothyroidism secondary to iodine deficiency is the leading cause of preventable intellectual disability in children.[3] In iodine-sufficient regions, the most common cause of hypothyroidism is the autoimmune disorder Hashimoto’s thyroiditis.
Structure[edit]
Features[edit]
The thyroid gland surrounds the cricoid and tracheal cartilages and consists of two lobes. This image shows a variant thyroid with a pyramidal lobe emerging from the middle of the thyroid.
The thyroid gland is a butterfly-shaped organ composed of two lobes, left and right, connected by a narrow tissue band, called an «isthmus».[4] It weighs 25 grams in adults, with each lobe being about 5 cm long, 3 cm wide, and 2 cm thick and the isthmus about 1.25 cm in height and width.[4] The gland is usually larger in women than in men, and increases in size during pregnancy.[4][5]
The thyroid is near the front of the neck, lying against and around the front of the larynx and trachea.[4] The thyroid cartilage and cricoid cartilage lie just above the gland, below the Adam’s apple. The isthmus extends from the second to third rings of the trachea, with the uppermost part of the lobes extending to the thyroid cartilage and the lowermost around the fourth to sixth tracheal rings.[6] The infrahyoid muscles lie in front of the gland and the sternocleidomastoid muscle to the side.[7] Behind the outer wings of the thyroid lie the two carotid arteries. The trachea, larynx, lower pharynx and esophagus all lie behind the thyroid.[5] In this region, the recurrent laryngeal nerve[8] and the inferior thyroid artery pass next to or in the ligament.[9] Typically, four parathyroid glands, two on each side, lie on each side between the two layers of the thyroid capsule, at the back of the thyroid lobes.[4]
The thyroid gland is covered by a thin fibrous capsule,[4] which has an inner and an outer layer. The inner layer extrudes into the gland and forms the septa that divide the thyroid tissue into microscopic lobules.[4] The outer layer is continuous with the pretracheal fascia, attaching the gland to the cricoid and thyroid cartilages[5] via a thickening of the fascia to form the posterior suspensory ligament of thyroid gland, also known as Berry’s ligament.[5] This causes the thyroid to move up and down with the movement of these cartilages when swallowing occurs.[5]
Blood, lymph and nerve supply[edit]
The thyroid is supplied with arterial blood from the superior thyroid artery, a branch of the external carotid artery, and the inferior thyroid artery, a branch of the thyrocervical trunk, and sometimes by an anatomical variant the thyroid ima artery,[4] which has a variable origin.[10] The superior thyroid artery splits into anterior and posterior branches supplying the thyroid, and the inferior thyroid artery splits into superior and inferior branches.[4] The superior and inferior thyroid arteries join behind the outer part of the thyroid lobes.[10] The venous blood is drained via superior and middle thyroid veins, which drain to the internal jugular vein, and via the inferior thyroid veins. The inferior thyroid veins originate in a network of veins and drain into the left and right brachiocephalic veins.[4] Both arteries and veins form a plexus between the two layers of the capsule of the thyroid gland.[10]
Lymphatic drainage frequently passes the prelaryngeal lymph nodes (located just above the isthmus) and the pretracheal and paratracheal lymph nodes.[4] The gland receives sympathetic nerve supply from the superior, middle and inferior cervical ganglion of the sympathetic trunk.[4] The gland receives parasympathetic nerve supply from the superior laryngeal nerve and the recurrent laryngeal nerve.[4]
Variation[edit]
Clear pyramidal lobe (center) as viewed from the front
There are many variants in the size and shape of the thyroid gland, and in the position of the embedded parathyroid glands.[5]
Sometimes there is a third lobe present called the pyramidal lobe.[5] When present, this lobe often stretches up to the hyoid bone from the thyroid isthmus and may be one to several divided lobes.[4] The presence of this lobe ranges in reported studies from 18.3%[11] to 44.6%.[12] It was shown to more often arise from the left side and occasionally separated.[11] The pyramidal lobe is also known as Lalouette’s pyramid.[13] The pyramidal lobe is a remnant of the thyroglossal duct, which usually wastes away during the thyroid gland’s descent.[5] Small accessory thyroid glands may in fact occur anywhere along the thyroglossal duct, from the foramen cecum of the tongue to the position of the thyroid in the adult.[4] A small horn at the back of the thyroid lobes, usually close to the recurrent laryngeal nerve and the inferior thyroid artery, is called Zuckerkandl’s tubercle.[9]
Other variants include a levator muscle of thyroid gland, connecting the isthmus to the body of the hyoid bone,[5] and the presence of the small thyroid ima artery.[5]
Microanatomy[edit]
Section of a thyroid gland under the microscope. 1 colloid, 2 follicular cells, 3 endothelial cells
At the microscopic level, there are three primary features of the thyroid—thyroid follicles, thyroid follicular cells, and parafollicular cells, first discovered by Geoffery Websterson in 1664.[14]
- Follicles
Thyroid follicles are small spherical groupings of cells 0.02–0.9mm in diameter that play the main role in thyroid function.[4] They consist of a rim that has a rich blood supply, nerve and lymphatic presence, that surrounds a core of colloid that consists mostly of thyroid hormone precursor proteins called thyroglobulin, an iodinated glycoprotein.[4][15]
- Follicular cells
The core of a follicle is surrounded by a single layer of follicular cells. When stimulated by thyroid stimulating hormone (TSH), these secrete the thyroid hormones T3 and T4. They do this by transporting and metabolising the thyroglobulin contained in the colloid.[4] Follicular cells vary in shape from flat to cuboid to columnar, depending on how active they are.[4][15]
- Follicular lumen
The follicular lumen is the fluid-filled space within a follicle of the thyroid gland. There are hundreds of follicles within the thyroid gland. A follicle is formed by a spherical arrangement of follicular cells. The follicular lumen is filled with colloid, a concentrated solution of thyroglobulin and is the site of synthesis of the thyroid hormones thyroxine (T4) and triiodothyronine (T3).[16]
- Parafollicular cells
Scattered among follicular cells and in spaces between the spherical follicles are another type of thyroid cell, parafollicular cells.[4] These cells secrete calcitonin and so are also called C cells.[17]
Development[edit]
Floor of pharynx of embryo between 35 and 37 days after fertilization.
In the development of the embryo, at 3–4 weeks gestational age, the thyroid gland appears as an epithelial proliferation in the floor of the pharynx at the base of the tongue between the tuberculum impar and the copula linguae. The copula soon becomes covered over by the hypopharyngeal eminence[18] at a point later indicated by the foramen cecum. The thyroid then descends in front of the pharyngeal gut as a bilobed diverticulum through the thyroglossal duct. Over the next few weeks, it migrates to the base of the neck, passing in front of the hyoid bone. During migration, the thyroid remains connected to the tongue by a narrow canal, the thyroglossal duct. At the end of the fifth week the thyroglossal duct degenerates, and over the following two weeks the detached thyroid migrates to its final position.[18]
The fetal hypothalamus and pituitary start to secrete thyrotropin-releasing hormone (TRH) and thyroid-stimulating hormone (TSH). TSH is first measurable at 11 weeks.[19] By 18–20 weeks, the production of thyroxine (T4) reaches a clinically significant and self-sufficient level.[19][20] Fetal triiodothyronine (T3) remains low, less than 15 ng/dL until 30 weeks, and increases to 50 ng/dL at full-term.[20] The fetus needs to be self-sufficient in thyroid hormones in order to guard against neurodevelopmental disorders that would arise from maternal hypothyroidism.[21] The presence of sufficient iodine is essential for healthy neurodevelopment.[22]
The neuroendocrine parafollicular cells, also known as C cells, responsible for the production of calcitonin, are derived from foregut endoderm. This part of the thyroid then first forms as the ultimopharyngeal body, which begins in the ventral fourth pharyngeal pouch and joins the primordial thyroid gland during its descent to its final location.[23]
Aberrations in prenatal development can result in various forms of thyroid dysgenesis which can cause congenital hypothyroidism, and if untreated this can lead to cretinism.[19]
Function[edit]
The thyroid hormones T3 and T4 have a number of metabolic, cardiovascular and developmental effects on the body. The production is stimulated by release of thyroid stimulating hormone (TSH), which in turn depends on release of thyrotropin releasing hormone (TRH). Every downstream hormone has negative feedback and decreases the level of the hormone that stimulates its release.
Thyroid hormones[edit]
The primary function of the thyroid is the production of the iodine-containing thyroid hormones, triiodothyronine (T3) and thyroxine or tetraiodothyronine (T4) and the peptide hormone calcitonin.[24] The thyroid hormones are created from iodine and tyrosine. T3 is so named because it contains three atoms of iodine per molecule and T4 contains four atoms of iodine per molecule.[25] The thyroid hormones have a wide range of effects on the human body. These include:
- Metabolic. The thyroid hormones increase the basal metabolic rate and have effects on almost all body tissues.[26] Appetite, the absorption of substances, and gut motility are all influenced by thyroid hormones.[27] They increase the absorption in the gut, generation, uptake by cells, and breakdown of glucose.[28] They stimulate the breakdown of fats, and increase the number of free fatty acids.[28] Despite increasing free fatty acids, thyroid hormones decrease cholesterol levels, perhaps by increasing the rate of secretion of cholesterol in bile.[28]
- Cardiovascular. The hormones increase the rate and strength of the heartbeat. They increase the rate of breathing, intake and consumption of oxygen, and increase the activity of mitochondria.[27] Combined, these factors increase blood flow and the body’s temperature.[27]
- Developmental. Thyroid hormones are important for normal development.[28] They increase the growth rate of young people,[29] and cells of the developing brain are a major target for the thyroid hormones T3 and T4. Thyroid hormones play a particularly crucial role in brain maturation during fetal development and first few years of postnatal life[28]
- The thyroid hormones also play a role in maintaining normal sexual function, sleep, and thought patterns. Increased levels are associated with increased speed of thought generation but decreased focus.[27] Sexual function, including libido and the maintenance of a normal menstrual cycle, are influenced by thyroid hormones.[27]
After secretion, only a very small proportion of the thyroid hormones travel freely in the blood. Most are bound to thyroxine-binding globulin (about 70%), transthyretin (10%), and albumin (15%).[30] Only the 0.03% of T4 and 0.3% of T3 traveling freely have hormonal activity.[31] In addition, up to 85% of the T3 in blood is produced following conversion from T4 by iodothyronine deiodinases in organs around the body.[24]
Thyroid hormones act by crossing the cell membrane and binding to intracellular nuclear thyroid hormone receptors TR-α1, TR-α2, TR-β1, and TR-β2, which bind with hormone response elements and transcription factors to modulate DNA transcription.[31][32] In addition to these actions on DNA, the thyroid hormones also act within the cell membrane or within cytoplasm via reactions with enzymes, including calcium ATPase, adenylyl cyclase, and glucose transporters.[19]
Hormone production[edit]
The thyroid hormones are created from thyroglobulin. This is a protein within the colloid in the follicular lumen that is originally created within the rough endoplasmic reticulum of follicular cells and then transported into the follicular lumen. Thyroglobulin contains 123 units of tyrosine, which reacts with iodine within the follicular lumen.[34]
Iodine is essential for the production of the thyroid hormones. Iodine (I0) travels in the blood as iodide (I−), which is taken up into the follicular cells by a sodium-iodide symporter. This is an ion channel on the cell membrane which in the same action transports two sodium ions and an iodide ion into the cell.[35] Iodide then travels from within the cell into the lumen, through the action of pendrin, an iodide-chloride antiporter. In the follicular lumen, the iodide is then oxidized to iodine. This makes it more reactive,[33] and the iodine is attached to the active tyrosine units in thyroglobulin by the enzyme thyroid peroxidase. This forms the precursors of thyroid hormones monoiodotyrosine (MIT), and diiodotyrosine (DIT).[2]
When the follicular cells are stimulated by thyroid-stimulating hormone, the follicular cells reabsorb thyroglobulin from the follicular lumen. The iodinated tyrosines are cleaved, forming the thyroid hormones T4, T3, DIT, MIT, and traces of reverse triiodothyronine. T3 and T4 are released into the blood. The hormones secreted from the gland are about 80–90% T4 and about 10–20% T3.[36][37] Deiodinase enzymes in peripheral tissues remove the iodine from MIT and DIT and convert T4 to T3 and RT3. [34] This is a major source of both RT3 (95%) and T3 (87%) in peripheral tissues.[38]
Regulation[edit]
The production of thyroxine and triiodothyronine is primarily regulated by thyroid-stimulating hormone (TSH), released by the anterior pituitary gland. TSH release in turn is stimulated by thyrotropin releasing hormone (TRH), released in a pulsatile manner from the hypothalamus.[39] The thyroid hormones provide negative feedback to the thyrotropes TSH and TRH: when the thyroid hormones are high, TSH production is suppressed. This negative feedback also occurs when levels of TSH are high, causing TRH production to be suppressed.[40]
TRH is secreted at an increased rate in situations such as cold exposure in order to stimulate thermogenesis.[41] In addition to being suppressed by the presence of thyroid hormones, TSH production is blunted by dopamine, somatostatin, and glucocorticoids.[42]
Calcitonin[edit]
The thyroid gland also produces the hormone calcitonin, which helps regulate blood calcium levels. Parafollicular cells produce calcitonin in response to high blood calcium. Calcitonin decreases the release of calcium from bone, by decreasing the activity of osteoclasts, cells which break down bone. Bone is constantly reabsorbed by osteoclasts and created by osteoblasts, so calcitonin effectively stimulates movement of calcium into bone. The effects of calcitonin are opposite those of the parathyroid hormone (PTH) produced in the parathyroid glands. However, calcitonin seems far less essential than PTH, since calcium metabolism remains clinically normal after removal of the thyroid (thyroidectomy), but not the parathyroid glands.[43]
Gene and protein expression[edit]
About 20,000 protein-coding genes are expressed in human cells: 70% of these genes are expressed in thyroid cells.[44][45] Two-hundred and fifty of these genes are more specifically expressed in the thyroid, and about 20 genes are highly thyroid specific. In the follicular cells, the proteins synthesized by these genes direct thyroid hormone synthesis—thyroglobulin, TPO, and IYD; while in the parafollicular c-cells, they direct calcitonin synthesis—CALCA, and CALCB.
Clinical significance[edit]
General practitioners, and internal medicine specialists play a role in identifying and monitoring the treatment of thyroid disease. Endocrinologists and thyroidologists are thyroid specialists. Thyroid surgeons or otolaryngologists are responsible for the surgical management of thyroid disease.
Functional disorders[edit]
Hyperthyroidism[edit]
Excessive production of the thyroid hormones is called hyperthyroidism. Causes include Graves’ disease, toxic multinodular goitre, solitary thyroid adenoma, inflammation, and a pituitary adenoma which secretes excess TSH. Another cause is excess iodine availability, either from excess ingestion, induced by the drug amiodarone, or following iodinated contrast imaging.[46][47]
Hyperthyroidism often causes a variety of non-specific symptoms including weight loss, increased appetite, insomnia, decreased tolerance of heat, tremor, palpitations, anxiety and nervousness. In some cases it can cause chest pain, diarrhoea, hair loss and muscle weakness.[48] Such symptoms may be managed temporarily with drugs such as beta blockers.[49]
Long-term management of hyperthyroidism may include drugs that suppress thyroid function such as propylthiouracil, carbimazole and methimazole.[50] Alternatively, radioactive iodine-131 can be used to destroy thyroid tissue: radioactive iodine is selectively taken up by thyroid cells, which over time destroys them. The chosen first-line treatment will depend on the individual and on the country where being treated. Surgery to remove the thyroid can sometimes be performed as a transoral thyroidectomy, a minimally invasive procedure.[51] Surgery does however carry a risk of damage to the parathyroid glands and the recurrent laryngeal nerve, which innervates the vocal cords. If the entire thyroid gland is removed, hypothyroidism will inevitably result, and thyroid hormone substitutes will be needed.[52][49]
Hypothyroidism[edit]
An underactive thyroid gland results in hypothyroidism. Typical symptoms are abnormal weight gain, tiredness, constipation, heavy menstrual bleeding, hair loss, cold intolerance, and a slow heart rate.[48] Iodine deficiency is the most common cause of hypothyroidism worldwide,[53] and the autoimmune disease Hashimoto’s thyroiditis is the most common cause in the developed world.[54] Other causes include congenital abnormalities, diseases causing transient inflammation, surgical removal or radioablation of the thyroid, the drugs amiodarone and lithium, amyloidosis, and sarcoidosis.[55] Some forms of hypothyroidism can result in myxedema and severe cases can result in myxedema coma.[56]
Hypothyroidism is managed with replacement of the thyroid hormones. This is usually given daily as an oral supplement, and may take a few weeks to become effective.[56] Some causes of hypothyroidism, such as Postpartum thyroiditis and Subacute thyroiditis may be transient and pass over time, and other causes such as iodine deficiency may be able to be rectified with dietary supplementation.[57]
Diseases[edit]
Graves’ disease[edit]
Graves’ disease is an autoimmune disorder that is the most common cause of hyperthyroidism.[58] In Graves’ disease, for an unknown reason autoantibodies develop against the thyroid stimulating hormone receptor. These antibodies activate the receptor, leading to development of a goitre and symptoms of hyperthyroidism, such as heat intolerance, weight loss, diarrhoea and palpitations. Occasionally such antibodies block but do not activate the receptor, leading to symptoms associated with hypothyroidism.[58] In addition, gradual protrusion of the eyes may occur, called Graves’ ophthalmopathy, as may swelling of the front of the shins.[58] Graves’ disease can be diagnosed by the presence of pathomnomonic features such as involvement of the eyes and shins, or isolation of autoantibodies, or by results of a radiolabelled uptake scan. Graves’ disease is treated with anti-thyroid drugs such as propylthiouracil, which decrease the production of thyroid hormones, but hold a high rate of relapse. If there is no involvement of the eyes, then use of radioactive isotopes to ablate the gland may be considered. Surgical removal of the gland with subsequent thyroid hormone replacement may be considered, however this will not control symptoms associated with the eye or skin.[58]
Nodules[edit]
Thyroid nodules are often found on the gland, with a prevalence of 4–7%.[59] The majority of nodules do not cause any symptoms, thyroid hormone secretion is normal, and they are non-cancerous.[60] Non-cancerous cases include simple cysts, colloid nodules, and thyroid adenomas. Malignant nodules, which only occur in about 5% of nodules, include follicular, papillary, medullary carcinomas and metastasis from other sites [61] Nodules are more likely in females, those who are exposed to radiation, and in those who are iodine deficient.[59]
When a nodule is present, thyroid function tests determine whether the nodule is secreting excess thyroid hormones, causing hyperthyroidism.[60] When the thyroid function tests are normal, an ultrasound is often used to investigate the nodule, and provide information such as whether the nodule is fluid-filled or a solid mass, and whether the appearance is suggestive of a benign or malignant cancer.[59] A needle aspiration biopsy may then be performed, and the sample undergoes cytology, in which the appearance of cells is viewed to determine whether they resemble normal or cancerous cells.[61]
The presence of multiple nodules is called a multinodular goitre; and if it is associated with hyperthyroidism, it is called a toxic multinodular goitre.[61]
Goitre[edit]
An enlarged thyroid gland is called a goitre.[62] Goitres are present in some form in about 5% of people,[61] and are the result of a large number of causes, including iodine deficiency, autoimmune disease (both Graves’ disease and Hashimoto’s thyroiditis), infection, inflammation, and infiltrative disease such as sarcoidosis and amyloidosis. Sometimes no cause can be found, a state called «simple goitre».[63]
Some forms of goitre are associated with pain, whereas many do not cause any symptoms. Enlarged goitres may extend beyond the normal position of the thyroid gland to below the sternum, around the airway or esophagus.[61] Goitres may be associated with hyperthyroidism or hypothyroidism, relating to the underlying cause of the goitre.[61] Thyroid function tests may be done to investigate the cause and effects of the goitre. The underlying cause of the goitre may be treated, however many goitres with no associated symptoms are simply monitored.[61]
Inflammation[edit]
Inflammation of the thyroid is called thyroiditis, and may cause symptoms of hyperthyroidism or hypothyroidism. Two types of thyroiditis initially present with hyperthyroidism and are sometimes followed by a period of hypothyroidism – Hashimoto’s thyroiditis and postpartum thyroiditis. There are other disorders that cause inflammation of the thyroid, and these include subacute thyroiditis, acute thyroiditis, silent thyroiditis, Riedel’s thyroiditis and traumatic injury, including palpation thyroiditis.[64]
Hashimoto’s thyroiditis is an autoimmune disorder in which the thyroid gland is infiltrated by the lymphocytes B cell and T cells. These progressively destroy the thyroid gland.[65] In this way, Hasimoto’s thyroiditis may have occurred insidiously, and only be noticed when thyroid hormone production decreases, causing symptoms of hypothyroidism.[65] Hashimoto’s is more common in females than males, much more common after the age of 60, and has known genetic risk factors.[65] Also more common in individuals with Hashimoto’s thyroiditis are Type 1 diabetes, pernicious anaemia, Addison’s disease vitiligo.[65]
Postpartum thyroiditis occurs sometimes following childbirth. After delivery, the thyroid becomes inflamed and the condition initially presents with a period of hyperthyroidism followed by hypothyroidism and, usually, a return to normal function. [66] The course of the illness takes place over several months, and is characterised by a painless goitre. Antibodies against thyroid peroxidase can be found on testing. The inflammation usually resolves without treatment, although thyroid hormone replacement may be needed during the period of hypothyroidism.[66]
Cancer[edit]
The most common tumor affecting the thyroid is a benign adenoma, usually presenting as a painless mass in the neck.[67] Thyroid cancers are most often carcinomas, although cancer can occur in any tissue that the thyroid consists of, including cancer of C-cells and lymphomas. Cancers from other sites also rarely lodge in the thyroid.[67] Radiation of the head and neck presents a risk factor for thyroid cancer, and cancer is more common in women than men, occurring at a rate of about 2:1.[67]
In most cases, thyroid cancer presents as a painless mass in the neck. It is very unusual for thyroid cancers to present with other symptoms, although in some cases cancer may cause hyperthyroidism.[68] Most thyroid cancers are papillary, followed by follicular, medullary, and thyroid lymphoma.[67][68] Because of the prominence of the thyroid gland, cancer is often detected earlier in the course of disease as the cause of a nodule, which may undergo fine-needle aspiration. Thyroid function tests will help reveal whether the nodule produces excess thyroid hormones. A radioactive iodine uptake test can help reveal the activity and location of the cancer and metastases.[67][69]
Thyroid cancers are treated by removing the whole or part of thyroid gland. Radioactive Iodine-131 may be given to radioablate the thyroid. Thyroxine is given to replace the hormones lost and to suppress TSH production, as TSH may stimulate recurrence.[69] With the exception of the rare anaplastic thyroid cancer, which carries a very poor prognosis, most thyroid cancers carry an excellent prognosis and can even be considered curable.[70]
Congenital[edit]
A persistent thyroglossal duct is the most common clinically significant birth defect of the thyroid gland. A persistent sinus tract may remain as a vestigial remnant of the tubular development of the thyroid gland. Parts of this tube may be obliterated, leaving small segments to form thyroglossal cysts.[23] Preterm neonates are at risk of hypothyroidism as their thyroid glands are insufficiently developed to meet their postnatal needs.[71] In order to detect hypothyroidism in newborn babies, to prevent growth and development abnormalities in later life, many countries have newborn screening programs at birth.[72]
Infants with thyroid hormone deficiency (congenital hypothyroidism) can manifest problems of physical growth and development as well as brain development, termed cretinism.[73][22] Children with congenital hypothyroidism are treated supplementally with levothyroxine, which facilitates normal growth and development.[74]
Mucinous, clear secretions may collect within these cysts to form either spherical masses or fusiform swellings, rarely larger than 2 to 3 cm in diameter. These are present in the midline of the neck anterior to the trachea. Segments of the duct and cysts that occur high in the neck are lined by stratified squamous epithelium, which is essentially identical to that covering the posterior portion of the tongue in the region of the foramen cecum. The disorders that occur in the lower neck more proximal to the thyroid gland are lined by epithelium resembling the thyroidal acinar epithelium. Characteristically, next to the lining epithelium, there is an intense lymphocytic infiltrate. Superimposed infection may convert these lesions into abscess cavities, and rarely, give rise to cancers.[citation needed]
Another disorder is that of thyroid dysgenesis which can result in various presentations of one or more misplaced accessory thyroid glands.[4] These can be asymptomatic.
Iodine[edit]
Iodine deficiency, most common in inland and mountainous areas, can predispose to goitre – if widespread, known as endemic goitre.[73] Pregnant women deficient of iodine can give birth to infants with thyroid hormone deficiency.[73][22] The use of iodised salt to add iodine to the diet[22] has eliminated endemic cretinism in most developed countries,[76] and over 120 countries have made the iodination of salt mandatory.[77][78]
Because the thyroid concentrates iodine, it also concentrates the various radioactive isotopes of iodine produced by nuclear fission. In the event of large accidental releases of such material into the environment, the uptake of radioactive iodine isotopes by the thyroid can, in theory, be blocked by saturating the uptake mechanism with a large surplus of non-radioactive iodine, taken in the form of potassium iodide tablets. One consequence of the Chernobyl disaster was an increase in thyroid cancers in children in the years following the accident.[79]
Excessive iodine intake is uncommon and usually has no effect on the thyroid function. Sometimes though it may cause hyperthyroidism, and sometimes hypothyroidism with a resulting goitre.[80]
Evaluation[edit]
The thyroid is examined by observation of the gland and surrounding neck for swelling or enlargement.[81] It is then felt, usually from behind, and a person is often asked to swallow to better feel the gland against the fingers of the examiner.[81] The gland moves up and down with swallowing because of its attachments to the thyroid and cricoid cartilages.[5] In a healthy person the gland is not visible yet is palpable as a soft mass. Examination of the thyroid gland includes the search for abnormal masses and the assessment of overall thyroid size.[82] The character of the thyroid, swellings, nodules, and their consistency may all be able to be felt. If a goitre is present, an examiner may also feel down the neck consider tapping the upper part of the chest to check for extension. Further tests may include raising the arms (Pemberton’s sign), listening to the gland with a stethoscope for bruits, testing of reflexes, and palpation of the lymph nodes in the head and neck.
An examination of the thyroid will also include observation of the person as a whole, to look for systemic signs such as weight gain or loss, hair loss, and signs in other locations – such as protrusion of the eyes or swelling of the calves in Graves’ disease.[83][81]
Tests[edit]
Thyroid function tests include a battery of blood tests, including the measurement of the thyroid hormones, as well as the measurement of thyroid stimulating hormone (TSH).[84] They may reveal hyperthyroidism (high T3 and T4), hypothyroidism (low T3, T4), or subclinical hyperthyroidism (normal T3 and T4 with a low TSH).[84]
TSH levels are considered the most sensitive marker of thyroid dysfunction.[84] They are however not always accurate, particularly if the cause of hypothyroidism is thought to be related to insufficient thyrotropin releasing hormone (TRH) secretion, in which case it may be low or falsely normal. In such a case a TRH stimulation test, in which TRH is given and TSH levels are measured at 30 and 60-minutes after, may be conducted.[84]
T3 and T4 can be measured directly. However, as the two thyroid hormones travel bound to other molecules, and it is the «free» component that is biologically active, free T3 and free T4 levels can be measured.[84] T3 is preferred, because in hypothyroidism T3 levels may be normal.[84] The ratio of bound to unbound thyroid hormones is known as the thyroid hormone binding ratio (THBR).[85] It is also possible to measure directly the main carriers of the thyroid hormones, thryoglobulin and throxine-binding globulin.[86] Thyroglobulin will also be measurable in a healthy thyroid, and will increase with inflammation, and may also be used to measure the success of thyroid removal or ablation. If successful, thyroglobulin should be undetectable.[85] Lastly, antibodies against components of the thyroid, particularly anti-TPO and anti-thyroglobulin, can be measured. These may be present in normal individuals but are highly sensitive for autoimmune-related disease.[85]
Imaging[edit]
Ultrasound of the thyroid may be used to reveal whether structures are solid or filled with fluid, helping to differentiate between nodules and goitres and cysts. It may also help differentiate between malignant and benign lesions.[87]
When further imaging is required, a radiolabelled iodine-123 or technetium-99 uptake scan may take place. This can determine the size and shape of lesions, reveal whether nodules or goitres are metabolically active, and reveal and monitor sites of thyroid disease or cancer deposits outside the thyroid.[88]
A fine needle aspiration of a sample of thyroid tissue may be taken in order to evaluate a lesion seen on ultrasound which is then sent for histopathology and cytology.[89]
Computed tomography of the thyroid plays an important role in the evaluation of thyroid cancer.[90] CT scans often incidentally find thyroid abnormalities, and thereby practically becomes the first investigation modality.[90]
History[edit]
The thyroid gland received its modern name in the 1600s, when the anatomist Thomas Wharton likened its shape to that of an Ancient Greek shield or thyos. However, the existence of the gland, and of the diseases associated with it, was known long before then.
Antiquity[edit]
The presence and diseases of the thyroid have been noted and treated for thousands of years.[91] In 1600 BCE burnt sponge and seaweed (which contain iodine) were used within China for the treatment of goitres, a practice which has developed in many parts of the world.[91][92] In Ayurvedic medicine, the book Sushruta Samhita written about 1400 BCE described hyperthyroidism, hypothyroidism and goitre.[92] Aristotle and Xenophon in the fifth century BCE describe cases of diffuse toxic goitre.[92] Hippocrates and Plato in the fourth century BCE provided some of the first descriptions of the gland itself, proposing its function as a salivary gland.[92] Pliny the Elder in the first century BCE referred to epidemics of goitre in the Alps and proposed treatment with burnt seaweed,[91] a practice also referred to by Galen in the second century, referred to burnt sponge for the treatment of goitre.[91] The Chinese pharmacology text Shennong Ben Cao Jing, written ca. 200–250, also refers to goitre.[91][92]
Scientific era[edit]
In 1500 polymath Leonardo da Vinci provided the first illustration of the thyroid.[91] In 1543 anatomist Andreas Vesalius gave the first anatomic description and illustration of the gland.[91] In 1656 the thyroid received its modern name, by the anatomist Thomas Wharton.[91] The gland was named thyroid, meaning shield, as its shape resembled the shields commonly used in Ancient Greece.[91] The English name thyroid gland[93] is derived from the medical Latin used by Wharton – glandula thyreoidea.[94] Glandula means ‘gland’ in Latin,[95] and thyreoidea can be traced back to the Ancient Greek word θυρεοειδής, meaning ‘shield-like/shield-shaped’.[96]
French chemist Bernard Courtois discovered iodine in 1811,[92] and in 1896 Eugen Baumann documented it as the central ingredient in the thyroid gland. He did this by boiling the thyroid glands of a thousand sheep, and named the precipitate, a combination of the thyroid hormones, ‘iodothyrin’.[92] David Marine in 1907 proved that iodine is necessary for thyroid function.[92][91]
Graves’ disease was described by Robert James Graves in 1834. The role of the thyroid gland in metabolism was demonstrated in 1895 by Adolf Magnus-Levy.[97] Thyroxine was first isolated in 1914 and synthesized in 1927, and triiodothyroxine in 1952.[92][98] The conversion of T4 to T3 was discovered in 1970.[91] The process of discovering TSH took place over the early to mid twentieth century.[99] TRH was discovered by Polish endocrinologist Andrew Schally in 1970, contributing in part to his Nobel Prize in Medicine in 1977.[91][100]
In the nineteenth century numerous authors described both cretinism and myxedema, and their relationship to the thyroid.[92] Charles Mayo coined the term hyperthyroidism in 1910.[91] Hakaru Hashimoto documented a case of Hashimoto’s thyroiditis in 1912, antibodies in this disease were demonstrated in 1956.[92] Knowledge of the thyroid and its conditions developed throughout the late nineteenth and twentieth centuries, with many modern treatments and investigative modalities evolving throughout the mid twentieth century, including the use of radioactive iodine, thiouracil and fine needle aspiration.[91]
Surgery[edit]
Either Aetius in the sixth century CE[92] or Persian Ali ibn Abbas al-Magusi in 990 CE conducted the first recorded thyroidectomy as a treatment for goitre.[91][101] Operations remained risky and generally were not successful until the 19th century, when descriptions emerged from a number of authors including Prussian surgeon Theodor Billroth, Swiss surgeon and physiologist Theodor Kocher, American physician Charles Mayo, American surgeons William Halsted and George Crile. These descriptions provided the basis for modern thyroid surgery.[102] Theodor Kocher went on to win the Nobel Prize in Physiology or Medicine in 1909 «for his work on the physiology, pathology and surgery of the thyroid gland».[103]
Other animals[edit]
The thyroid gland is found in all vertebrates. In fish, it is usually located below the gills and is not always divided into distinct lobes. However, in some teleosts, patches of thyroid tissue are found elsewhere in the body, associated with the kidneys, spleen, heart, or eyes.[104]
In tetrapods, the thyroid is always found somewhere in the neck region. In most tetrapod species, there are two paired thyroid glands – that is, the right and left lobes are not joined. However, there is only ever a single thyroid gland in most mammals, and the shape found in humans is common to many other species.[104]
In larval lampreys, the thyroid originates as an exocrine gland, secreting its hormones into the gut, and associated with the larva’s filter-feeding apparatus. In the adult lamprey, the gland separates from the gut, and becomes endocrine, but this path of development may reflect the evolutionary origin of the thyroid. For instance, the closest living relatives of vertebrates, the tunicates and amphioxi (lancelets), have a structure very similar to that of larval lampreys (the endostyle), and this also secretes iodine-containing compounds, though not thyroxine.[104]
Thyroxine is critical to metabolic regulation, and growth throughout the vertebrate clade. Iodine and T4 trigger the change from a plant-eating water-dwelling tadpole into a meat-eating land-dwelling frog, with better neurological, visuospatial, smell and cognitive abilities for hunting, as seen in other predatory animals. A similar phenomenon happens in the neotenic amphibian salamanders, which, without introducing iodine, don’t transform into land-dwelling adults, and live and reproduce in the larval form of aquatic axolotl. Among amphibians, administering a thyroid-blocking agent such as propylthiouracil (PTU) can prevent tadpoles from metamorphosing into frogs; in contrast, administering thyroxine will trigger metamorphosis. In amphibian metamorphosis, thyroxine and iodine also exert a well-studied experimental model of apoptosis on the cells of gills, tail, and fins of tadpoles. Iodine, via iodolipids, has favored the evolution of terrestrial animal species and has likely played a crucial role in the evolution of the human brain.[105][106]
See also[edit]
- Desiccated thyroid
- Thyroid disease in pregnancy
References[edit]
- ^ Guyton & Hall 2011, p. 907.
- ^ a b Boron WF, Boulpaep EL (2012). Medical Physiology (2nd ed.). Philadelphia: Saunders. p. 1052. ISBN 978-1-4377-1753-2.
- ^ Harrison’s 2011, pp. 2913, 2918.
- ^ a b c d e f g h i j k l m n o p q r s t u Gray’s Anatomy 2008, pp. 462–4.
- ^ a b c d e f g h i j k Elsevier’s 2007, p. 342.
- ^ Elsevier’s 2007, pp. 342–3.
- ^ Ellis H, Standring S, Gray HD (2005). Gray’s anatomy: the anatomical basis of clinical practice. St. Louis, Mo: Elsevier Churchill Livingstone. pp. 538–539. ISBN 978-0-443-07168-3.
- ^ Netter FH (2014). Atlas of Human Anatomy Including Student Consult Interactive Ancillaries and Guides (6th ed.). Philadelphia, Penn.: W B Saunders Co. p. 27. ISBN 978-1-4557-0418-7.
- ^ a b Page C, Cuvelier P, Biet A, Boute P, Laude M, Strunski V (July 2009). «Thyroid tubercle of Zuckerkandl: anatomical and surgical experience from 79 thyroidectomies». The Journal of Laryngology and Otology. 123 (7): 768–71. doi:10.1017/s0022215108004003. PMID 19000342. S2CID 22063700.
- ^ a b c Elsevier’s 2007, p. 343.
- ^ a b Cicekcibasi AE, Salbacak A, Seker M, Ziylan T, Tuncer I, Buyukmumcu M (April 2007). «Developmental variations and clinical importance of the fetal thyroid gland. A morphometric study». Saudi Medical Journal. 28 (4): 524–8. PMID 17457471.
- ^ Kim DW, Jung SL, Baek JH, Kim J, Ryu JH, Na DG, et al. (January 2013). «The prevalence and features of thyroid pyramidal lobe, accessory thyroid, and ectopic thyroid as assessed by computed tomography: a multicenter study». Thyroid. 23 (1): 84–91. doi:10.1089/thy.2012.0253. PMID 23031220.
- ^ Dorland WA (2012). Anderson DM (ed.). Dorland’sIllustrated Medical Dictionary (32nd ed.). Elsevier Saunders. pp. 999 redirect to 1562. ISBN 978-1-4160-6257-8.
- ^ Fawcett D, Jensh R (2002). Bloom & Fawcett’s Concise Histology. New York: Arnold Publishers. pp. 257–258. ISBN 978-0-340-80677-7.
- ^ a b Wheater PR, Young B (2006). Wheater’s functional histology : a text and colour atlas (5th ed.). Oxford: Churchill Livingstone. pp. 333–335. ISBN 978-0-443-06850-8.
- ^ The Thyroid Follicle Archived 2013-01-23 at archive.today, Endocrinology by J. Larry Jameson, MD, PhD and Leslie J. De Groot, MD, chapter 72
- ^ Hazard JB (July 1977). «The C cells (parafollicular cells) of the thyroid gland and medullary thyroid carcinoma. A review». The American Journal of Pathology. 88 (1): 213–50. PMC 2032150. PMID 18012.
- ^ a b Larsen WJ (2001). Human embryology (3. ed.). Philadelphia, Pa.: Churchill Livingstone. pp. 372–374. ISBN 978-0-443-06583-5.
- ^ a b c d Greenspan’s 2011, p. 179.
- ^ a b Eugster EA, Pescovitz OH (2004). Pediatric endocrinology: mechanisms, manifestations and management. Hagerstwon, MD: Lippincott Williams & Wilkins. p. 493 (Table 33–3). ISBN 978-0-7817-4059-3.
- ^ Zoeller RT (April 2003). «Transplacental thyroxine and fetal brain development». The Journal of Clinical Investigation. 111 (7): 954–7. doi:10.1172/JCI18236. PMC 152596. PMID 12671044.
- ^ a b c d «Iodine supplementation in pregnant and lactating women». World Health Organization. Archived from the original on January 4, 2014. Retrieved 2016-11-13.
- ^ a b Langman J, Sadler TW, Sadler-Redmond SL, Tosney K, Byrne J, Imseis H (2015). Langman’s Medical Embryology (13th ed.). pp. 285–6, 293. ISBN 978-1-4511-9164-6.
- ^ a b Davidson’s 2010, p. 736.
- ^ Guyton & Hall 2011, p. 909.
- ^ Guyton & Hall 2011, p. 934.
- ^ a b c d e Guyton & Hall 2011, p. 937.
- ^ a b c d e Guyton & Hall 2011, p. 936.
- ^ Guyton & Hall 2011, p. 935-6.
- ^ Greenspan’s 2011, p. 169.
- ^ a b Bowen R (2000). «Thyroid Hormone Receptors». Colorado State University. Archived from the original on 27 September 2011. Retrieved 22 February 2015.
- ^ Greenspan’s 2011, p. 178.
- ^ a b Boron WF, Boulpaep E (2003). «Chapter 48: «synthesis of thyroid hormones»«. Medical Physiology: A Cellular And Molecular Approaoch. Elsevier/Saunders. p. 1300. ISBN 978-1-4160-2328-9.
- ^ a b Bianco AC, Salvatore D, Gereben B, Berry MJ, Larsen PR (February 2002). «Biochemistry, cellular and molecular biology, and physiological roles of the iodothyronine selenodeiodinases». Endocrine Reviews. 23 (1): 38–89. doi:10.1210/edrv.23.1.0455. PMID 11844744.
- ^ Melmed S, Polonsky KS, Larsen PR, Kronenberg HM (2011). Williams Textbook of Endocrinology (12th ed.). Saunders. p. 331. ISBN 978-1-4377-0324-5.
- ^ How Your Thyroid Works: A Delicate Feedback Mechanism. Updated 2009-05-21.
- ^ The thyroid gland in Endocrinology: An Integrated Approach by Stephen Nussey and Saffron Whitehead (2001) Published by BIOS Scientific Publishers Ltd. ISBN 1-85996-252-1
- ^ Ganong’s review of medical physiology Edition 25.
- ^ Greenspan’s 2011, p. 174.
- ^ Greenspan’s 2011, p. 177.
- ^ Guyton & Hall 2011, p. 896.
- ^ Harrison’s 2011, pp. 2215.
- ^ Guyton & Hall 2011, pp. 988–9.
- ^ «The human proteome in thyroid gland – The Human Protein Atlas». www.proteinatlas.org. Retrieved 2017-09-25.
- ^ Uhlén M, Fagerberg L, Hallström BM, Lindskog C, Oksvold P, Mardinoglu A, et al. (January 2015). «Proteomics. Tissue-based map of the human proteome». Science. 347 (6220): 1260419. doi:10.1126/science.1260419. PMID 25613900. S2CID 802377.
- ^ Davidson’s 2010, p. 738.
- ^ Rusandu A, Sjøvold BH, Hofstad E, Reidunsdatter RJ (June 2020). «Iodinated contrast media and their effect on thyroid function — Routines and practices among diagnostic imaging departments in Norway». Journal of Medical Radiation Sciences. 67 (2): 111–118. doi:10.1002/jmrs.390. PMC 7276191. PMID 32232955.
- ^ a b Davidson’s 2010, p. 740.
- ^ a b Davidson’s 2010, p. 739.
- ^ Davidson’s 2010, p. 745.
- ^ Cury AN, Meira VT, Monte O, Marone M, Scalissi NM, Kochi C, et al. (March 2013). «Clinical experience with radioactive iodine in the treatment of childhood and adolescent Graves’ disease». Endocrine Connections. 2 (1): 32–7. doi:10.1530/EC-12-0049. PMC 3680965. PMID 23781316.
- ^ Thyroid Problems eMedicine Health. Retrieved on 2010-02-07
- ^ «Iodine Deficiency & Nutrition». www.thyroidfoundation.org.au. Australian Thyroid Foundation. Archived from the original on 13 January 2017. Retrieved 11 January 2017.
- ^ So M, MacIsaac R, Grossmann M. «Hypothyroidism – Investigation and management». www.racgp.org.au. The Royal Australian College of General Practitioners. Retrieved 11 January 2017.
- ^ Davidson’s 2010, p. 741.
- ^ a b Davidson’s 2010, p. 743.
- ^ Davidson’s 2010, p. 741-3.
- ^ a b c d Smith TJ, Hegedüs L (October 2016). «Graves’ Disease» (PDF). The New England Journal of Medicine. 375 (16): 1552–1565. doi:10.1056/nejmra1510030. PMID 27797318.
- ^ a b c Dean DS, Gharib H (December 2008). «Epidemiology of thyroid nodules». Best Practice & Research. Clinical Endocrinology & Metabolism. 22 (6): 901–11. doi:10.1016/j.beem.2008.09.019. PMID 19041821.
- ^ a b Welker MJ, Orlov D (February 2003). «Thyroid nodules». American Family Physician. 67 (3): 559–66. PMID 12588078. Retrieved 6 September 2016.
- ^ a b c d e f g Davidson’s 2010, p. 744.
- ^ «goitre – definition of goitre in English». Oxford Dictionaries | English. Archived from the original on September 18, 2016. Retrieved 18 September 2016.
- ^ Davidson’s 2010, p. 750.
- ^ Harrison’s 2011, pp. 2237.
- ^ a b c d Harrison’s 2011, pp. 2230.
- ^ a b Harrison’s 2011, pp. 2238.
- ^ a b c d e Harrison’s 2011, p. 2242.
- ^ a b Davidson’s 2010, p. 751.
- ^ a b Davidson’s 2010, p. 752.
- ^ Harrison’s 2011, p. 2242,2246.
- ^ Berbel P, Navarro D, Ausó E, Varea E, Rodríguez AE, Ballesta JJ, et al. (June 2010). «Role of late maternal thyroid hormones in cerebral cortex development: an experimental model for human prematurity». Cerebral Cortex. 20 (6): 1462–75. doi:10.1093/cercor/bhp212. PMC 2871377. PMID 19812240.
- ^ Büyükgebiz A (15 November 2012). «Newborn screening for congenital hypothyroidism». Journal of Clinical Research in Pediatric Endocrinology. 5 Suppl 1 (4): 8–12. doi:10.4274/Jcrpe.845. PMC 3608007. PMID 23154158.
- ^ a b c Greenspan’s 2011, p. 164.
- ^ Rose SR, Brown RS, Foley T, Kaplowitz PB, Kaye CI, Sundararajan S, Varma SK (June 2006). «Update of newborn screening and therapy for congenital hypothyroidism». Pediatrics. 117 (6): 2290–303. doi:10.1542/peds.2006-0915. PMID 16740880.
- ^ The thyroid gland in health and disease Year: 1917 Robert McCarrison
- ^ Harris RE (2015-05-07). Global Epidemiology of Cancer. Jones & Bartlett Publishers. p. 268. ISBN 978-1-284-03445-5.
- ^ Leung AM, Braverman LE, Pearce EN (November 2012). «History of U.S. iodine fortification and supplementation». Nutrients. 4 (11): 1740–6. doi:10.3390/nu4111740. PMC 3509517. PMID 23201844.
- ^ «Map: Count of Nutrients In Fortification Standards». Global Fortification Data Exchange. Retrieved 23 December 2019.
- ^ «Chernobyl children show DNA changes». BBC News. 2001-05-08. Retrieved 2010-05-25.
- ^ «Iodine — Disorders of Nutrition». MSD Manual Consumer Version. Archived from the original on 18 December 2019. Retrieved 18 December 2019.
- ^ a b c Talley N (2014). Clinical Examination. Churchill Livingstone. pp. Chapter 28. «The endocrine system». pp 355–362. ISBN 978-0-7295-4198-5.
- ^ Fehrenbach; Herring (2012). Illustrated Anatomy of the Head and Neck. Elsevier. p. 158. ISBN 978-1-4377-2419-6.
- ^ Harrison’s 2011, p. 2228.
- ^ a b c d e f Greenspan’s 2011, p. 184.
- ^ a b c Harrison’s 2011, p. 2229.
- ^ Greenspan’s 2011, p. 186.
- ^ Greenspan’s 2011, p. 189.
- ^ Greenspan’s 2011, p. 188-9.
- ^ Greenspan’s 2011, p. 190.
- ^ a b Bin Saeedan M, Aljohani IM, Khushaim AO, Bukhari SQ, Elnaas ST (August 2016). «Thyroid computed tomography imaging: pictorial review of variable pathologies». Insights into Imaging. 7 (4): 601–17. doi:10.1007/s13244-016-0506-5. PMC 4956631. PMID 27271508. Creative Commons Attribution 4.0 International License
- ^ a b c d e f g h i j k l m n o «Thyroid History Timeline – American Thyroid Association». www.thyroid.org. Retrieved 13 November 2016.[dead link]
- ^ a b c d e f g h i j k l Niazi AK, Kalra S, Irfan A, Islam A (July 2011). «Thyroidology over the ages». Indian Journal of Endocrinology and Metabolism. 15 (Suppl 2): S121-6. doi:10.4103/2230-8210.83347. PMC 3169859. PMID 21966648.
- ^ Anderson DM (2000). Dorland’s Illustrated Medical Dictionary (29th ed.). Philadelphia/London/Toronto/Montreal/Sydney/Tokyo: W.B. Saunders Company.
- ^ His W (1895). Die anatomische Nomenclatur. Nomina Anatomica. Der von der Anatomischen Gesellschaft auf ihrer IX. Versammlung in Basel angenommenen Namen [The anatomical nomenclature. Nominal Anatomica. Anatomical Society on its IX. Assembly adopted in Basel] (in German). Leipzig: Verlag Veit & Comp.
- ^ Lewis CT, Short C (1879). A Latin dictionary. founded on Andrews’ edition of Freund’s Latin dictionary. Oxford: Clarendon Press.
- ^ Liddell HG, Scott R (1940). A Greek-English Lexicon. revised and augmented throughout by Sir Henry Stuart Jones. with the assistance of. Roderick McKenzie. Oxford: Clarendon Press.
- ^ Freake HC, Oppenheimer JH (1995). «Thermogenesis and thyroid function». Annual Review of Nutrition. 15 (1): 263–91. doi:10.1146/annurev.nu.15.070195.001403. PMID 8527221.
- ^ Hamdy, Roland. «The thyroid glands: a brief historical perspective». www.medscape.com. Retrieved 2016-11-13.
- ^ Magner J (June 2014). «Historical note: many steps led to the ‘discovery’ of thyroid-stimulating hormone». European Thyroid Journal. 3 (2): 95–100. doi:10.1159/000360534. PMC 4109514. PMID 25114872.
- ^ «The Nobel Prize in Physiology or Medicine 1977». www.nobelprize.org. Retrieved 14 January 2017.
- ^ Slidescenter.com. «Hormones.gr». www.hormones.gr. Retrieved 2016-11-13.
- ^ Werner SC, Ingbar SH, Braverman LE, Utiger RD (2005). Werner & Ingbar’s the Thyroid: A Fundamental and Clinical Text. Lippincott Williams & Wilkins. p. 387. ISBN 978-0-7817-5047-9.
- ^ «The Nobel Prize in Physiology or Medicine 1909». Nobel Foundation. Retrieved 2007-07-28.
- ^ a b c Romer AS, Parsons TS (1977). The Vertebrate Body. Philadelphia, PA: Holt-Saunders International. pp. 555–556. ISBN 978-0-03-910284-5.
- ^ Venturi S (2011). «Evolutionary Significance of Iodine». Current Chemical Biology. 5 (3): 155–162. doi:10.2174/187231311796765012. ISSN 1872-3136.
- ^ Venturi S (2014). «Iodine, PUFAs and Iodolipids in Health and Disease: An Evolutionary Perspective». Human Evolution. 29 (1–3): 185–205. ISSN 0393-9375.
Books[edit]
- Greer MA, ed. (1990). The Thyroid Gland. Comprehensive Endocrinology Revised Series. N.Y.: Raven Press. ISBN 0-88167-668-3.
- Shoback D (2011). Gardner DG (ed.). Greenspan’s basic & clinical endocrinology (9th ed.). New York: McGraw-Hill Medical. ISBN 978-0-07-162243-1.
- Hall JE, Guyton AC (2011). Guyton and Hall textbook of medical physiology (12th ed.). Philadelphia, Pa.: Saunders/Elsevier. ISBN 978-1-4160-4574-8.
- Longo D, Fauci A, Kasper D, Hauser S, Jameson J, Loscalzo J (August 11, 2011). Harrison’s Principles of Internal Medicine (18 ed.). McGraw-Hill Professional. ISBN 978-0-07-174889-6.
- Colledge NR, Walker BR, Ralston SH, eds. (2010). Davidson’s principles and practice of medicine. Illustrated by Robert Britton (21st ed.). Edinburgh: Churchill Livingstone/Elsevier. ISBN 978-0-7020-3085-7.
- Ort V, Bogart BI (2007). Elsevier’s integrated anatomy and embryology. Philadelphia, Pa.: Elsevier Saunders. ISBN 978-1-4160-3165-9.
- Standring S, Borley NR, et al., eds. (2008). Gray’s anatomy : the anatomical basis of clinical practice (40th ed.). London: Churchill Livingstone. ISBN 978-0-8089-2371-8.
External links[edit]
![]()
Wikimedia Commons has media related to Thyroid.
- Endocrine Web: Thyroid
Эндокринная железа в области шеи; выделяют гормоны, влияющие на метаболизм
| Щитовидная железа | |
|---|---|
| Щитовидная железа человека (загар), если смотреть спереди; и артерии (красные), снабжающие железу. |
|
| Щитовидная металлизация на шее, ниже адамова яблока. |
|
| Детали | |
| Произношение | |
| Предшественник | Дивертикул щитовидной железы (продолжение энтодермы во 2-ю глоточную дугу ) |
| Система | Эндокринная система |
| Артерия | Верхняя, Нижние артерии щитовидной железы |
| Вена | Верхняя, средний, Нижние вены щитовидной железы |
| Идентификаторы | |
| Latin | Glandula thyreoidea |
| MeSH | D013961 |
| TA98 | A11.3.00. 001 |
| TA2 | 3863 |
| FMA | 9603 |
| Анатомическая терминология [редактирование в Викиданных ] |
щитовидная железа или щитовидная железа, представляет собой эндокринную железу в шее, состоящую из двух соединенных долей. Две нижние трети долей соединены тонкой лентой ткани называется перешейком щитовидной железы. 138>адамова яблока. Микроскопич фолликул щитовидной железы, выстланный фолликулярными клетками (тироцитами) и случайными парафолликулярными клетками, которые окружают просвет, предоставленный коллоид. Щитовидная железа секретирует три гормона: два гормона щитовидной железы — трийодтиронин (T 3) и тироксин (T 4) — и пептидный гормон, Кальцитонин. Гормоны щитовидной железы оказывают влияние на скорость метаболизма и синтез белка, а у детей — на рост и развитие. Кальцитонин играет роль в гомеостаз кальция. Секреция двух тироидных гормонов регулируется тиреотропным гормоном (ТТГ), который секретируется передней долей гипофиза железой. TRH), который вырабатывается гипоталамусом.
Щитовидная железа на основании глотки у основания языка на 3–4 недели беременности; он опускается перед глоточной кишкой и, в конечном итоге, в течение следующих нескольких недель Во время миграции щитовидная железа используется с языком узким каналом, щитовидно-язычный проток. недели щитовидно-язычный протокол дегенерирует, и в течение следующих двух недель отслоившаяся щитовидная железа перемещается в свое окончательное положение.
Заболевания щитовидной железы включает гипертиреоз, гипотиреоз, воспаление щитовидной железы 58>(тиреоидит ), увеличение щитовидной железы (зоб ), узелки щитовидной железы и рак щитовидной железы. Гипертиреоз характеризуется чрезмерной секрецией гормонов щитовидной железы: наиболее частой причиной аутоиммунное заболевание болезнь Грейвса. Гипотиреоз характеризуется недостаточной секрецией гормонов щитовидной железы: наиболее частой причиной является дефицит йода. В регионах с дефицитом йода гипотиреоз, вторичный по отношению к дефициту йода, является ведущей причиной предотвратимой умственной отсталости у детей. В регионах с достаточным содержанием йода наиболее частой причиной гипотиреоза является аутоиммунное заболевание тиреоидит Хашимото.
Наличие щитовидной железы и ее заболевания отмечены и лечились на протяжении столетия, хотя сама железа была описана только и назван со времен Возрождения. Знания о щитовидной железе, ее биохимии и заболевания, развивающиеся в конце девятнадцатого и двадцатого веков. Многие современные методы лечения и методы исследования развивались на протяжении середины двадцатого века, включая усовершенствование хирургических методов удаления щитовидной железы (тиреоидэктомия ) для лечения зоба ; использование радиоактивного йода и тиоурацила для лечения болезни Грейвса; и тонкоигольная аспирация для диагностики узлов щитовидной железы.
Содержание
- 1 Структура
- 1.1 Характеристики
- 1.2 Кровоснабжение, лимфо- и нервное кровоснабжение
- 1.3 Вариант
- 1.4 Микроанатомия
- 2 Развитие
- 3 Функция
- 3.1 Гормоны щитовидной железы
- 3.2 Производство гормонов
- 3.3 Регулирование
- 3.4 Кальцитонин
- 4 Экспрессия генов и белков
- 5 Клиническая значимость
- 5.1 Функциональные расстройства
- 5.1.1 Гипертиреоз
- 5.1. 2 Гипотиреоз
- 5.2 Заболевания
- 5.2.1 Болезнь Грейвса
- 5.2.2 Узлы
- 5.2.3 Зоб
- 5.2.4 Воспаление
- 5.2.5 Рак
- 5.2.6 Врожденный
- 5.2.7 Йод
- 5.3 Оценка
- 5.4 Исследования
- 5.4.1 Визуализация
- 5.1 Функциональные расстройства
- 6 История
- 6.1 Древность
- 6.2 Научная эра
- 6.3 Хирургия
- 7 Другие животные
- 8 См. Также
- 9 Ссылки
- 9.1 Книги
- 10 Внешние ссылки
Структура
Характеристики
Щитовидная железа окружает перстневидный хрящ и хрящи трахеи и состоит из двух долей. На этом изображении показан вариант щитовидной железы с пирамидальной долей, выходящей из середины щитовидной железы.
Щитовидная железа представляет собой орган в форме бабочки, состоящий из двух долей, левой и правой, соединенных узкой тканевой полосой, называемой перешейком. «. У взрослых особей он весит 25 грамм, каждая составляет около 5 см в длину, 3 см в ширину и 2 см в толщину, а перешеек 1,25 см в высоту и ширину.
Щитовидная железа находится ближе к передней части шеи, напротив и вокруг передней части гортани и трахея. щитовидный хрящ и перстневидный хрящ лежат чуть выше железы, кадыка. Перешеек простирается от второго до третьего колец трахеи, причем самая верхняя часть долей проходит до щитовидного хряща, а самая нижняя — вокруг четвертого-шестого колец трахеи. подъязычная мышца лежит перед железой, а грудино-ключично-сосцевидная мышца сбоку.>сонные артерии. Трахея, гортань, нижняя часть глотки и пищевод расположены позади щитовидной железы. и нижняя щитовидная артерия проходят рядом со связкой или в ней. Обычно четыре паращитовидных желез, по две с каждой стороны, лежат с каждой стороны между двумя слоями капсулы щитовидной железы, в задней части долей щитовидной железы.
Щитовидная железа покрыта слоем щитовидной железы. тонкая фиброзная капсула, имеющая внутренний и внешний слой. Внутренний слой выдавливает в железу и образует перегородки, которые разделяют ткань щитовидной железы на микроскопические дольки. Внешний слой продолжается претрахеальной фасцией, прикрепляя железу к перстневидному и щитовидному хрящам через утолщение фасции, образуя заднюю фасцию поддерживающую связку щитовидной железы, также известную как Связка Берри. Это заставляет щитовидную железу двигаться вверх и вниз вместе с движением хрящей при глотании.
Кровоснабжение, лимфо- и нервное кровообращение
Щитовидная железа снабжается артериальной кровью из верхнего щитовидная артерия, ветвь наружной сонной артерии и нижняя тироидная артерия, ветвь тироцервикального ствола, а иногда и анатомический вариант артерия има щитовидной железы, имеющая различное происхождение. Верхняя щитовидная артерия разделяется на переднюю и заднюю ветви, снабжающие щитовидную железу, нижнюю щитовидную артерия разделяется на верхнюю и нижнюю ветви. Верхняя и нижняя артерии щитовидной железы представляют собой внешнюю часть долей щитовидной железы. Венозная кровь отводится через верхнюю и среднюю вены щитовидной железы, которые отводятся к внутренней яремной вене, и через нижние вены щитовидной железы. Нижние вены щитовидной железы берут начало в сети венчают и впадают в левую и правую брахиоцефальные вены. И артерии, и вены образуют сплетение между двумя капсулами щитовидной железы.
Лимфатический дренаж проходит часто через предларингеальные лимфатические узлы (расположенные чуть выше перешейка) и претрахеальные и паратрахеальные лимфатические узлы. Железа питание получает симпатического нерва от верхнего, среднего и нижнего шейного ганглия симпатического ствола. Железа питание получает парасимпатического нерва от верхнего гортанного нерва и возвратного гортанного нерва.
Вариант
Четкая пирамидальная доля (в центре), если смотреть спереди
Существует много вариантов по размеру и форме щитовидной железы, а также по положению внедрения паращитовидных желез.
Иногда присутствует третья доля, называемая пирамидальной долей. При наличии эта доля часто тянется вверх по подъязычной кости от перешейка щитовидной железы и может быть от одной до нескольких долей. Наличие этой доли колеблется в опубликованных исследованиях от 18,3% до 44,6%. Было показано, что она чаще возникает с левой стороны и иногда отделяется. Пирамидальный лепесток также известен как пирамида Лалоуэта. Пирамидная доля — это остаток щитовидно-язычного протока, который обычно разрушается во время опускания щитовидной железы. Маленькие дополнительные щитовидные железы располагаться где угодно вдоль щитовидно-язычного протока, от отверстия слепойки языка до места расположения щитовидной железы у взрослых. Небольшой рог в задней части долей щитовидной железы, обычно рядом с возвратным гортанным нервом и нижним щитовидной артерией, называется бугорком Цукеркандля.
. Другие варианты включают поднимающую мышцу щитовидной железы, соединение перешейка с телом подъязычной кости и наличие небольшого артерии щитовидной железы.
Микроанатомия
срез щитовидной железы под микроскопом. 1 коллоид, 2 фолликулярные клетки, 3 эндотелиальные клетки
На микроскопическом уровне есть три основных характеристики щитовидной железы: фолликулы, фолликулярные клетки, и парафолликулярные клетки, впервые обнаруженные Джеффери Вебстерсоном в 1664 году.
- Фолликулы
Фолликулы щитовидной железы — это небольшие сферические группы клеток размером 0,02–0,9 мм, которые играют основную роль в функциях щитовидной железы.. Они состоят из ободка, который имеет обильное кровоснабжение, наличие нервных и лимфатических сосудов, которое окружает ядро из коллоида, которое в основном состоит из белков-предшественников тиреоидных гормонов, называемых тиреоглобулином и йодированный гликопротеин.
- Фолликулярные клетки
Ядро фолликула окружено одним слоем фолликулярных клеток. При стимуляции тироид-стимулирующим гормоном (ТТГ) они секретируют тироидные гормоны Т3 и Т4. Они делают это, транспортируя и метаболизируя тиреоглобулин, поддержся в коллоиде. Фолликулярные клетки различаются по форме от плоских до кубовидных или столбчатых, в зависимости от того, насколько они активны.
- Парафолликулярные клетки
Разбросанные среди фолликулярных клеток и в промежутках между сферическими фолликулами — это еще один тип тироидных клеток, парафолликулярные клетки. Эти клетки секретируют кальцитонин и поэтому также называются С-клетками.
Развитие
Дно глотки эмбриона между 35 и 37 днями после оплодотворения.
В развитие эмбриона, на срок 3–4 недели гестационного возраста щитовидная железа проявляется в виде эпителиальной пролиферации на дне глотки у основания языка между tuberculum impar и copula linguae. Связка вскоре покрывается гипофарингеальным возвышением в точке, позже обозначенной отверстием слепой кишки. Затем щитовидная железа опускается перед глоточной кишкой в виде двулопастного дивертикула через щитовидно-язычный проток. В течение нескольких недель он перемещается к основанию шеи, проходя перед подъязычной костью. Во время перемещения щитовидная железа используется с языком узким каналом, щитовидно-язычным протоком. В конце пятой недели щитовидно-язычный протокол дегенерирует, и в течение следующих двух недель отслоившаяся щитовидная перемещается в свое окончательное положение.
плод гипоталамус и гипофиз начинает секретировать тиреотропин-рилизинг-гормон (TRH) и тиреотропный гормон (ТТГ). ТТГ впервые измерить в 11 недель. К 18–20 неделям продукции тироксина (T4) наступает клинически значимого и самодостаточного уровня. Фетальный трийодтиронин (T3) остается низким, менее 15 нг / дл до 30 недель, и увеличивается до 50 нг / дл доношенному. плод должен быть самодостаточным в гормонах щитовидной железы, чтобы защититься от нарушений нервного развития, которые могут возникнуть в результате гипотиреоза матери. Наличие достаточного количества йода необходимо для здорового развития нервной системы.
нейроэндокринные парафолликулярные клетки, также известные как C-клетки, ответственные за выработку кальцитонина, прошедшие из энтодермы передней кишки. Затем эта часть щитовидной железы сначала формируется в виде ультимофарингеального тела, которое начинается в четвертом брюшном глоточном кармане и соединяется с первичной щитовидной железой во время ее опускания к своему окончательному расположению.
Аберрации в пренатальном развитии могут приводить к различным формам дисгенезии щитовидной железы, которые могут вызвать врожденный гипотиреоз, а при отсутствии лечения это может привести к кретинизму.
Функция
гормоны щитовидной железы T3 и T4 обеспечивают систему метаболических, сердечно-сосудистых и связанных с созданием эффектов. Производство стимулируется высвобождением тиреотропного гормона (ТТГ), которое, в свою очередь, зависит от высвобождения тиреотропин-рилизинг-гормона (TRH). Каждый последующий гормон имеет отрицательную обратную связь и снижает уровень гормона, который стимулирует его высвобождение.
Гормоны щитовидной железы
Основная функция щитовидной железы — производство йодсодержащих гормоны щитовидной железы, трийодтиронин (T3) и тироксин (T4) и пептидный гормон кальцитонин. Гормоны щитовидной железы из йода и тирозина. Т 3 назван так потому, что он содержит три атома йода на молекулу, а Т 4 содержит четыре атома йода на молекулу. Гормоны щитовидной железы имеют широкий спектр воздействия на организм человека. К ним креп:
- Метаболические. Гормоны щитовидной железы имеют базальную скорость метаболизма и почти на все ткани организма. На аппетит, всасывание веществ и моторику кишечника, гормоны щитовидной железы. Они увеличивают всасывание в кишечнике, поколение, захват клетками и расщепление глюкозы. Они стимулируют расщепление количества жиров и увеличивают свободных жирных кислот. Несмотря на увеличение свободных жирных кислот, гормоны щитовидной железы снижают уровень холестерина, возможно, за счет увеличения скорости секреции холестерина желчью.
- сердечно-сосудистой системы. Гормоны увеличивают частоту и силу сердцебиения.. Они увеличивают частоту дыхания, прием и потребление кислорода, а также повышают активность митохондрий. В совокупности эти факторы увеличивают кровоток и температуру тела.
- Развитие. Гормоны щитовидной железы важны для нормального развития. Они увеличивают скорость роста молодых людей, а клетки развивающегося мозга являются основной мишенью для гормонов щитовидной железы Т 3 и Т 4. Гормоны щитовидной железы играют важную роль в созревании мозга во время внутриутробного развития и в первые несколько лет постнатальной жизни
- Гормоны щитовидной железы также играют роль в поддержании нормальной половой функции, сна и образа мышления. Повышенные уровни связаны с повышением уровня генерации мыслей, но снижением внимания. На сексуальную функцию, включая либидо и поддержание нормального менструального цикла, влияние гормоны щитовидной железы.
После секреции лишь очень небольшая часть гормонов щитовидной железы свободно перемещается по крови. Большинство из них связано с тирокинсвязывающим глобулином (около 70%), транстиретином (10%) и альбумином (15%). Только 0,03% из Т 4 и 0,3% из Т 3 свободно путешествующих обладающих гормональной активностью. Кроме того, до 85% Т 3 в крови продуцируется после преобразования из Т 4 с помощью йодтиронин дейодиназы в органах вокруг тела.
Гормоны щитовидной железы, пересекая клеточную мембрану и связываясь с внутриклеточными ядерными рецепторами тироидных гормонов TR -α 1, TR-α 2, TR-β 1 и TR-β 2, которые связываются с элементами гормонального ответа и факторы транскрипции для модуляции транскрипции ДНК. Помимо этих воздействий на ДНК, гормоны щитовидной железы также действуют внутри клеточной мембраны или цитоплазмы посредством реакций с ферментами, включая кальциевую АТФазу, аденилилциклазу, и переносчики глюкозы.
Производство гормонов
Синтез гормонов щитовидной железы, как видно на отдельных фолликулярных клетках щитовидной железы :. — Тироглобулин синтезируется в грубый эндоплазматический ретикулум и следует по секреторному пути, чтобы проникнуть в коллоид в просвет фолликула щитовидной железы посредством экзоцитоза.. — Между тем, симпортер йодида натрия (Na / I) активно закачивает йодид (I) в клетку, которая ранее пересекла эндотелий с помощью в значительной степени неизвестных механизмов.. — Этот йодид входит в просвет фолликулов из цитоплазмы посредством переносчика пендрина якобы пассивным образом.. — В коллоиде йодид (I) окисляется до йода (I) ферментом, называемым тироидпероксидазой.. — Йод (I) очень реакционноспособен и йодирует тиреоглобулин по тирозильным остаткам в его белковой цепи (всего содержит примерно 120 тирозильных остатков).. — При конъюгации соседние тирозильные остатки соединяются вместе.. — Весь комплекс повторно входит в фолликулярную клетку посредством эндоцитоза.. — Протеолиза различными протеазами высвобождает тироксин и трийодтиронин молекулы, которые попадают в кровь по в значительной степени неизвестным механизмам.
Гормоны щитовидной железы создаются из тиреоглобулина. Это белок в коллоиде в просвете фолликула, который первоначально создается в шероховатом эндоплазматическом ретикулуме фолликулярных клеток, а затем транспортируется в просвет фолликула. Тироглобулин содержит 123 единицы тирозина, который реагирует с йодом в просвете фолликула.
Йод необходим для выработки гормонов щитовидной железы. Йод (I) перемещается в крови в виде йодида (I), который поглощается фолликулярными клетками с помощью симпортера йодида натрия. Это ионный канал на клеточной мембране, который одновременно переносит два иона натрия и ион йодида в клетку. Затем йодид перемещается изнутри клетки в просвет под действием пендрина, йодид-хлоридного антипортера. Затем в просвете фолликула йодид окисляется до йода. Это делает его более реактивным, и йод присоединяется к активным тирозиновым единицам тиреоглобулина с помощью фермента тироидпероксидазы. При этом образуются предшественники гормонов щитовидной железы монойодтирозин (MIT) и дииодтирозин (DIT).
Когда фолликулярные клетки стимулируются тиреотропным гормоном фолликулярные клеткиреабсорбируют тиреоглобулин из просвета фолликула. Йодированные тирозины расщепляются, образуя гормоны щитовидной железы T 4, T 3, DIT, MIT и следы обратного трийодтиронина. Т 3 и Т 4 выделяются в крови. Гормоны, секретируемые железой, составляют около 80–90% T 4 и около 10–20% T 3.Ферменты дейодиназы в периферических тканях удаляют йод из MIT и DIT и преобразуют T 4 до T 3 и RT 3. Это основной источник как RT 3 (95%), так и T 3 (87%) в периферических тканях.
Регламент
Производство тироксина и трийодтиронина в основном регулируется тиреотропным гормоном (ТТГ), выделяемым передней долей гипофиза железа. Высвобождение ТТГ, в свою очередь, стимулирует тиротропин-рилизинг-гормоном (TRH), пульсирующим образом выделяющимся из гипоталамуса. Гормоны щитовидной железы отрицательная обратная связь с тиреотропами ТТГ и ТРГ: когда гормоны щитовидной железы высоки, производство ТТГ подавляется. Эта отрицательная обратная связь также вызывает, когда уровни ТТГ высоки, вызывая подавление выработки ТРГ.
ТРГ секретируется с повышенной скоростью в таких ситуациях, как воздействие холода, чтобы стимулировать термогенез. В дополнение к подавлению гормонов щитовидной железы, производство ТТГ подавляется дофамином, соматостатином и глюкокортикоидами.
кальцитонином
щитовидной железой. железа также производит гормон кальцитонин, который помогает регулировать уровень кальция в крови. Парафолликулярные клетки продуцируют кальцитонин в ответ на высокое содержание кальция в крови. Кальцитонин снижает высвобождение кальция из костей за счет снижения активности остеокластов, разрушающих кость клеток. Кость постоянно реабсорбируется остеокластами и создается остеобластами, чтобы кальцитонин эффективно стимулирует перемещение кальция в кость. Эффекты кальцитонина противоположны действию паратироидного гормона (ПТГ), вырабатываемого паращитовидными железами. Однако кальцитонин кажется гораздо менее важным, чем ПТГ, поскольку метаболизм кальция остается нормальным после удаления щитовидной железы (тиреоидэктомия ), но не паращитовидные железы.
Экспрессия генов и белков
Около 20 000 генов, кодирующих белок, экспрессируются в клетках человека: 70% этих генов экспрессируются в клетках щитовидной железы. Двести пятьдесят из этих генов более специфично экспрессируются в щитовидной железе, и около 20 генов высоко специфичны для щитовидной железы. В фолликулярных клетках белки, синтезируемые этими генами, направляют синтез гормонов щитовидной железы — тиреоглобулин, TPO и IYD ; в то время как в парафолликулярных клетках они направляют синтез кальцитонина — CALCA и CALCB.
Клиническое значение
Врачи общей практики, семейные врачи и внутренние болезни специалисты играют роль в выявлении и контроле лечения заболеваний щитовидной железы. Эндокринологи и тиреоидологи — специалисты по щитовидной железе. Хирурги-тироиды или отоларингологи несут ответственность за хирургическое лечение заболеваний щитовидной железы.
Функциональные расстройства
Гипертиреоз
Избыточное производство гормонов щитовидной железы называется гипертиреозом. Причины включают болезнь Грейвса, токсический многоузловой зоб, одиночную аденому щитовидной железы, воспаление и аденому гипофиза, который секретирует избыточный ТТГ. Другая причина — избыток йода, вызванный приемом препарата амиодарон или йодсодержащим контрастом визуализацией.
Гипертиреоз часто вызывает различные неспецифические симптомы, включая потерю веса, повышенный аппетит, бессонницу, снижение переносимости тепла, тремор, сердцебиение, беспокойство и нервозность. В некоторых случаях может вызвать боль в груди, диарею, выпадение волос и мышечную слабость. Такие симптомы можно временно купировать с помощью таких препаратов, как бета-блокаторы.
. Долгое лечение гипертиреоза вспомогательные препараты, подавляющие функцию щитовидной железы, такие как пропилтиоурацил, карбимазол и метимазол. В качестве радиоактивного йода >можно использовать для разрушения ткани щитовидной железы: радиоактивный йод избирательно поглощается клетками щитовидной железы, которые со временем разрушают их. Выбор лечения первой линии будет зависеть от пациента и страны, в которой он проходит лечение. Операция по удалению щитовидной железы иногда может быть выполнена как трансоральная тиреоидэктомия, малоинвазивная процедура. Однако операция сопряжена с риском повреждения паращитовидных желез и возвратного гортанного нерва, который иннервирует голосовые связки. Если удалить всю щитовидную железу, это неизбежно приведет к гипотиреозу, и потребуются заменители тироидных гормонов.
Гипотиреоз
Недостаточная активность щитовидной железы приводит к гипотиреозу.. Типичными симптомами являются ненормальное увеличение веса, усталость, запор, сильное менструальное кровотечение, выпадение волос, непереносимость холода и медленное сердцебиение. Дефицит йода — самая частая причина гипотиреоза во всем мире, аутоиммунное заболевание тиреоидит Хашимото — самая частая причина в развитом мире. Другие причины включают врожденные аномалии, заболевания, вызывающие преходящее воспаление, хирургическое удаление или радиоабляцию щитовидной железы, препараты амиодарон и литий, амилоидоз и саркоидоз.. Некоторые формы гипотиреоза могут привести к микседеме, в тяжелых случаях — к микседемной коме.
Гипотиреоз лечится с помощью замены гормона тироксином. Обычно он принимается ежедневно в виде пероральной добавки. Некоторые причины гипотиреоза, такие как послеродовой тиреоидит и подострый тиреоидит, могут быть временными и проходить с течением времени, и другие причины, такие как дефицит йода, можно устранить с помощью пищевых добавок.
Заболевания
Болезнь Грейвса
Болезнь Грейвса — это аутоиммунное заболевание, которое является наиболее частой причиной гипертиреоза. При болезни Грейвса по неизвестной разработке развиваются аутоантитела против рецептора тиреотропного гормона. Эти антитела активируют рецептор, что приводит к развитию зоба и симптомов гипертиреоза, как непереносимость тепла, потеря веса, диарея и учащенное сердцебиение. Иногда такие антитела блокируют, но не активируют рецептор, что приводит к симптомам, гипотиреозом. Кроме того, может происходить текущее выпячивание глаз, называемое офтальмопатией Грейвса, а также отек передней части голеней. Болезнь Грейвса может быть диагностирована по наличию патомномонических признаков, таких как поражение глаз и голеней или выделение аутоантител, или по результатам сила с радиоактивной меткой. Болезнь Грейвса лечится антитероидными препаратами, такими как пропилтиоурацил, которые снижают выработку гормонов щитовидной железы, но имеют высокий рецидивов. Если глаза не поражены, то можно рассмотреть возможность использования радиоактивных изотопов для удаления железы. Можно рассмотреть возможность хирургического удаления железы с заменой гормона щитовидной железы, однако это не поможет контролировать симптомы, связанные с глазами или кожей.
Узлы
Узлы щитовидной железы часто обнаруживаются на железе, с распространенность 4–7%. Большинство узлов не вызывают никаких симптомов, секреция гормонов щитовидной железы в норме, и они не являются злокачественными. К незлокачественным случаем класса простых кисты, коллоидные узелки и аденомы щитовидной железы. Злокачественные узлы, которые встречаются примерно только в 5% узлов, включают фолликулярные, папиллярные, медуллярные карциномы и метастазы из других участков. более вероятны у женщин, у тех, кто подвергается облучению, и у тех, кто испытывает дефицит йода.
При наличии узелка тесты функции щитовидной железы определяют, секретирует ли узелток щитовидной железы гормоны, вызывающие гипертиреоз. Когда тесты функции щитовидной железы в норме, УЗИ часто используется для исследования узла и предоставления информации, например, ли узел заполненной жидкостью или твердой массой, указывает ли внешний вид на доброкачественное или злокачественный рак. Затем может быть выполнена пункционная аспирационная биопсия , образец подвергнут цитологии, в которой вид клеток оценивается, чтобы определить, похожи ли они на нормальные или раковые клетки.
Наличие множественных узлов называется многоузловым зобом ; и если это связано с гипертиреозом, это называется токсическим многоузловым зобом.
зобом
Увеличенная щитовидная железа называется зобом. Зоб в той или иной форме присутствует примерно у 5% людей и является результатом большого количества причин, включая дефицит йода, аутоиммунное заболевание (как болезнь Грейвса, так и тиреоидит Хашимото), инфекции, воспаления и инфильтративное заболевание, такое как саркоидоз и амилоидоз. Иногда причина не может быть обнаружена, это состояние называется «простой зоб».
Некоторые зоба связаны с болью, некоторые не вызывают никаких симптомов. Увеличенный зоб может выходить за пределы нормального положения щитовидной железы до уровня груди ниже, вокруг дыхательных путей или пищевода. Зоб может быть связан с гипертиоидизмом или гипотиреозом, относящимся к основной причине зоба. Функциональные тесты щитовидной железы могут быть выполнены для выяснения причины и последствия зоба. Основную причину зоба можно лечить, однако многие зоб без сопутствующих симптомов просто контролируется.
Воспаление
Воспаление щитовидной железы называется тиреоидитом и может вызывать симптомы гипертиреоза или гипотиреоза. Два типа тиреоидита используются проявляются гипертиреозом и иногда сменяются периодом гипотиреоза — тиреоидит Хашимото и послеродовой тиреоидит. Есть и другие заболевания, вызывающие воспаление щитовидной железы, и к ним относятся подострый тиреоидит, острый тиреоидит, тихий тиреоидит, тиреоидит Риделя и травматическое повреждение, включая пальпаторный тиреоидит.
тиреоидит Хашимото — это аутоиммунное заболевание, при котором щитовидная железа инфильтрована лимфоцитами B-клетками и Т-клетки. Они постепенно разрушают щитовидную железу. Таким образом, производство гормонов щитовидной железы снижается, вызывая симптомы гипотиреоза. Хашимото чаще встречается у женщин, чем у мужчин гораздо чаще встречается после 60 лет и имеет известные генетические факторы риска. Также у лиц с тиреоидитом Хашимото чаще встречаются диабет 1 типа, злокачественная анемия, болезнь Аддисона витилиго.
послеродовой тиреоидит. некоторые женщины после родов. После родов железа воспаляется, и состояние сначала проявляется периодом гипертиреоза, за которым следует гипотиреоз и, как правило, восстановление нормальной функции. Течение болезни длится несколько месяцев и характеризуется безболезненным зобом. Антитела против тироидпероксидазы можно обнаружить при тестировании. Воспаление обычно проходит без лечения, хотя в период гипотиреоза может потребоваться заместительная терапия гормонами щитовидной железы.
Рак
Наиболее частым новообразованием, поражающим щитовидную железу, является доброкачественное аденома, обычно проявляющаяся в виде безболезненного образования на шее. Злокачественные опухоли щитовидной железы чаще всего представляют собой карциномы, хотя рак может возникать в любой ткани, из которой состоит щитовидная железа, включая рак С-клеток и лимфомы. Рак из других мест также редко попадает в щитовидную железу. Облучение головы и шеи представляет собой фактор риска рака щитовидной железы, и рак чаще встречается у женщин, чем у мужчин, примерно 2: 1.
В большинстве случаев, рак щитовидной железы проявляется в виде безболезненного образования на шее. Очень редко рак щитовидной железы проявляется другими симптомами, хотя в некоторых случаях рак может вызывать гипертиреоз. Большинство злокачественных опухолей щитовидной железы — это папиллярный, за которым следуют фолликулярная, медуллярная и лимфома щитовидной железы. Из-за выступа щитовидной железы рак часто выявляется на более раннем этапе болезни как причина узелка, который может быть подвергнут тонкоигольной аспирации. Функциональные тесты щитовидной железы помогут определить, производит ли узелок избыток гормонов щитовидной железы. Тест на поглощение радиоактивного йода может помочь выявить активность и локализацию рака и метастазов.
Рак щитовидной железы лечится удалением всей или части щитовидной железы. Радиоактивный йод 131 можно вводить для радиоактивной абляции щитовидной железы. Тироксин назначают для восполнения утраченных гормонов и подавления выработки ТТГ, поскольку ТТГ может стимулировать рецидив. За исключением редкого анапластического рака щитовидной железы, который имеет очень плохой прогноз, большинство случаев рака щитовидной железы имеют отличный прогноз и даже могут считаться излечимыми.
Врожденный
A устойчивый тиреоглоссальный проток. — наиболее частое клинически значимое врожденное заболевание щитовидной железы. Устойчивый синусовый тракт может оставаться рудиментарным остатком канальцевого развития щитовидной железы. Части этой трубки могут быть облитерированы, оставляя небольшие сегменты с образованием кисты щитовидной железы s. Недоношенные новорожденные подверженные риску гипотиреоза, поскольку их щитовидные железы недостаточно развиты для удовлетворения их постнатальных потребностей. Для гипотиреоза у новорожденных и аномалий роста и развития в более позднем возрасте во многих странах существуют программы скрининга новорожденных при рождении.
Младенцы с дефицитом гормонов щитовидной железы (врожденные гипотиреоз ) могут происходить проблемы физического роста и развития, а также развитие мозга, что называется кретинизмом. Детей с врожденным гипотиреозом лечат также левотироксином, который способствует нормальному росту и развитию.
В этих кистах могут скапливаться слизистые прозрачные образования со сферических масс или веретенообразных опухолей, редко превышающих От 2 до 3 см в диаметре. Они присутствуют по средней линии шеи впереди трахеи. Сегменты протока и кисты, расположенные высоко на шее, выстланы , многослойным эпителием, который по существу идентичен, который покрывает заднюю часть языка в области отверстия. слепая кишка. Заболевания, развивающие в нижней части шеи, проксимальнее щитовидной железы, выстланы эпителием, напоминающие ацинарный эпителий щитовидной железы. Характерно, что рядом с подкладочным эпителием происходит интенсивный лимфоцитарный инфильтрат. Наложенная инфекция может преобразовать эти поражения в полости абсцесса и в редких случаях вызвать рак.
Еще одно заболевание — это дисгенезия щитовидной железы, которая может приводить к различным проявлениям одна или несколько неуместных дополнительных щитовидной железы. Это может быть бессимптомно.
Йод
Ребенок, страдающий кретинизмом, связанный с недостатком йода.
Дефицит йода, наиболее часто встречающийся во внутренних и горных районах, может предрасполагать к зобу — если широко распространен, известен как эндемический зоб. Беременные женщины с дефицитом йода могут родить детей с дефицитом гормона щитовидной железы. Использование йодированной соли для добавления йода в рацион устранило эндемический кретинизм в большинстве развитых стран, и более 120 стран сделали йодирование соли обязательного.
Временная щитовидная железа концентрирует йод, она также концентрирует различные радиоактивные изотопы йода, образующиеся в результате ядерного деления. Нерадиоактивного йода, принимаемые в виде таблеток йодида калия. Одним из последствий Чернобыльской катастрофы стал рост рака щитовидной железы у детей в годы после аварии.
Чрезмерное потребление йода встречается редко и обычно не влияет на функцию щитовидной железы. Хотя иногда это может вызвать гипертиреоз, а иногда гипотиреоз с последующим зобом.
Оценка
Щитовидная железа исследуется путем осмотра железы и окружающей среды на предмет отека или увеличения. Затем его прощупывают, обычно сзади, и человека просят сглотнуть, чтобы лучше почувствовать железу пальцами часто обследуемого. При глотании железа движется вверх и вниз из-за ее прикрепления к щитовидной железе и перстневидному хрящу. У здорового человека железа не видна, но пальпируется в виде мягкого образования. Обследование щитовидной железы включает поиск аномальных образований и оценку общего размера щитовидной железы. Можно почувствовать характер щитовидной железы, опухоли, узелки и их консистенцию. При наличии зоба врач может также ощупать шею, рассмотреть возможность проверки верхней части грудной клетки, чтобы проверить ее расширение. Дальнейшие тесты могут быть поднятие (признак Пембертона ), прослушивание железы с помощью стетоскопа при ушибах, тестирование рефсов и пальпацию лимфатических узлов. в голове и шее.
Обследование щитовидной железы также включает наблюдение за человеком в целом такими функциями, как увеличение или потеря веса, выпадение волос и других признаков, таких как выпячивание глаз или отек телят при болезни Грейвса.
Тесты
Функциональные тесты щитовидной железы включают набор крови анализов, включая определение гормонов щитовидной железы, а также измерение тиреотропного гормона (ТТГ). Они могут выявить гипертиреоз (высокий T3 и T4), гипотиреоз (низкий T3, T4) или субклинический гипертиреоз (нормальный T3 и T4 с низким ТТГ).
Уровни ТТГ наиболее чувствительным маркером дисфункции щитовидной железы.. Однако не всегда точны, считается, что причиной гипотиреоза является недостаточная секреция тиреотропин-рилизинг-гормона (TRH), и в случае она может быть низкой или ложно нормальной. В этом случае происходит тест стимуляции TRH, в котором происходит TRH, уровни TSH измеряются через 30 и 60 минут после этого.
T3 и T4 могут быть измерены напрямую. Как два гормона щитовидной железы путешествуют связанными с молекулами, а биологически активным «свободным» компонентом, можно измерить уровни свободного Т3 и свободного Т4. Т4 предпочтительнее, потому что при гипотиреозе уровень Т3 может быть нормальным. Соотношение связанных и несвязанных гормонов щитовидной железы известно как коэффициент связывания гормонов щитовидной железы (THBR). Также возможно напрямую измерить основных носителей гормонов щитовидной железы, триоглобулина и троксин-связывающего глобулина. Тироглобулин также можно измерить в здоровой щитовидной железе и будет увеличиваться при воспалении. В случае успеха тиреоглобулин не должен определяться. Наконец, можно измерить антитела против компонентов щитовидной железы, в частности, антител к ТПО и тиреоглобулину. Они могут присутствовать у нормальных людей, но очень чувствительны к аутоиммунным заболеваниям.
Визуализация
Ультразвук щитовидной железы может определить, являются ли структуры твердыми или заполненными жидкостью, что отличить узелки от зоба и кисты. Это также может помочь отличить злокачественные новообразования от доброкачественных.
Когда требуется дальнейшая визуализация, может проводиться сканирование мощного радиоактивно меченного йода-123 или технеция-99. Это может определить размер и форму поражений, выявить, являются ли узлы или зоб метаболически активными заболеваниями, выявить и контролировать участки тонких отложений за пределами щитовидной железы.
A коигольная аспирация образец щитовидной железы ткань может быть взята для поражения, видимого на УЗИ, которое затем отправляется на гистопатолог и цитологию.
Компьютерная томография щитовидной железы играет важную роль в оценке щитовидной железы. рак. КТ часто случайно обнаруживает аномалии щитовидной железы, таким образом, становится практически первым методом исследования.
История
Томас Уортон назвал щитовидную железу в честь древнегреческого щита с похожим произношением. Показан пример такого щита, выгравированный на монете , датируемой 431–424 гг. До н. Э..
Щитовидная железа получила свое современное название в 1600-х годах, когда анатом Томас Уортон сравнил ее по форме напоминал древнегреческий щит или тиос. Однако о существовании железы и о связанных с ней заболеваниях было известно до этого до этого.
Древность
Наличие и заболевания щитовидной железы отмечались и лечились на протяжении тысячелетий. В 1600 г. до н.э. сожженные губки и водоросли (содержащий йод) использовались в Китае для лечения зоба, практика, которая получила развитие во многих частях мира. В аюрведической медицине книга Сушрута Самхита, написанная около 1400 г. до н.э., описывала гипертиреоз, гипотиреоз и зоб. Аристотель и Ксенофонт в пятом веке до н.э. жалобах диффузного токсического зоба. Гиппократ и Платон в четвертом веке нашей эры предоставили из первых возможностей самой железы, предлагая ее функцию как слюнную железу. Плиний Старший в первом веке нашей эры регистрирул об эпидемиях зоба в <328 году.>Альпы и предложили лечение обожженными водорослями; практика, также упоминаемая Галеном во втором веке, относилась к обожженной губке для лечения зоба. Китайская фармакология текст Шэннун Бен Цао Цзин, написанный ок. 200–250, также относится к зобу.
Научная эра
В 1500 году эрудит Леонардо да Винчи представил первую иллюстрацию щитовидной железы. В 1543 году анатом Андреас Везалий дал первое анатомическое описание и иллюстрацию железы. В 1656 году анатомом Томасом Уортоном щитовидная железа получила свое современное название. Эта железа была названа щитовидной железой, что означает ее форма напоминала щиты, обычно используется в Древней Греции. Английское название «щитовидная железа» происходит от текущего Уортоном медицинского латыни — glandula thyreoidea. Гландула в переводе с латыни означает железа, а тиреоидея восходит к древнегреческому слову θυρεοειδής, означающему щитоподобный / щитообразный.
Французский химик Бернар Куртуа открыл йод в 1811 году, а в 1896 году Ойген Бауман задокументировал его как центральный ингредиент в триоидной железе. Он сделал это путем кипячения щитовидной железы тысячи овец и назвал осадок, комбинациюмонов щитовидной железы, «йодтирин». Дэвид Марин в 1907 году доказал, что йод необходим для функций щитовидной железы.
Болезнь Грейвса была описана Робертом Джеймсом Грейвсом в 1834 году. Роль щитовидной железы в обмене веществ была установлена в 1895 году Адольфом Магнус-Леви. Тироксин был впервые выделен в 1914 году и синтезирован в 1927 году, а трийодтироксин — в 1952 году. Превращение Т4 в Т3 было обнаружено в 1970 году. Процесс открытия ТТГ происходил с начала до середины двадцатого века. TRH был открыт польским эндокринологом Эндрю Шалли в 1970 году, частично способствовав получению Нобелевской программы по медицине в 1977 году.
В девятнадцатом веке многие авторы описали и кретинизм и микседема и их связь с щитовидной железой. Чарльз Мэйо ввел термин гипертиреоз в 1910 году. Хакару Хашимото задокументировал случай тиреоидита Хашимото в 1912 году, антитела к этому заболеванию были использованы в 1956 году. конца девятнадцатого и двадцатого веков, с появлением в середине двадцатого века современных методов лечения и методов исследования, включая использование радиоактивного йода, тиоурацила и тонкоигольной аспирации.
Хирургия
Либо Аэций в шестом веке эры или перс Али ибн Аббас аль-Магуси в 990 году нашей эры провел первую зарегистрированную тиреоидэктомию для лечение зоба. Как правило, появились описания ряда авторов, включая прусского хирурга Теодора Бильрота, швейцарского хирурга и физиолога Теодора Кохера, американского врача Чарльз Мэйо, американские хирурги Уильям Холстед и Джордж Крайл. Эти описания легли в основу современной хирургии щитовидной железы. Теодор Кохер в 1909 году получил Нобелевскую премию по физиологии и медицине «за свои работы по физиологии, патологии и хирургии щитовидная железа».
Другие животные
Козы, пораженные зобом
Щитовидная железа у всех позвоночных, однако он обычно расположен ниже жабр и не всегда разделен на отдельные доли при некоторых костистых телах участков ткани
У четвероногих, щитовидная железа всегда находится где-то в области шеи, щитовидная железа всегда находится в других частях тела, связанных с почками, селезенкой, сердцем или сердцем. парные щитовидные железы, одна из которых является общей для многих других видов.
У личинок миног щитовидная железа происходит из экзокринной железы, секретирую щей свои гормоны в кишечнике и личном с фильтрующим аппаратоминки. У взрослой миноги железа отделяется происхождение кишечника и эндокринной железы, но этот путь развития может отражать эволюционное развитие щитовидной железы. Например, ближайшие из ныне живущих родственников позвоночных, оболочники и Amphioxus, имеют строение, очень похожее на строение личинок миног (эндостиль ), и это также выделяет йодсодержащие соединения, но не тироксин.
Тироксин имеет решающее значение для регуляции метаболизма и роста во всем животном мире. Йод и Т4 запускают переход из водного растения, питающегося головастиком, в мясоедного наземного обитателя лягушки с улучшенным неврологическим, зрительно-пространственным запахом. и когнитивные способности для охоты, как у других хищных животных. Аналогичное явление происходит у неотенических амфибий саламандр, которые без введения йода не превращаются в наземных взрослых особей, а живут и размножаются в личиночной форме водных аксолотль. Среди амфибий введение агента, блокирующего щитовидную железу, такого как пропилтиоурацил (PTU), может предотвратить превращение головастиков в лягушек; Напротив, введение тироксина вызовет метаморфоз. При метаморфозе амфибий тироксин и йод также предоставьте себя хорошо изученную экспериментальную модель апоптоза на клетках жабр, хвоста и плавников головастиков. Йод через йодолипиды способствовал эволюции наземных животных и, вероятно, сыграл решающую роль в эволюции человеческого мозга.
См.
- Высушенная щитовидная железа
- Заболевание щитовидной железы при беременности
Ссылки
Книги
>Внешние ссылки
- Эндокринная сеть: щитовидная железа
Содержание
- 1 Русский
- 1.1 Морфологические и синтаксические свойства
- 1.2 Произношение
- 1.3 Семантические свойства
- 1.3.1 Значение
- 1.3.2 Синонимы
- 1.3.3 Антонимы
- 1.3.4 Гиперонимы
- 1.3.5 Гипонимы
- 1.4 Родственные слова
- 1.5 Этимология
- 1.6 Фразеологизмы и устойчивые сочетания
- 1.7 Перевод
- 1.8 Библиография
Русский[править]
| В Викиданных есть лексема щитовидка (L181070). |
Морфологические и синтаксические свойства[править]
| падеж | ед. ч. | мн. ч. |
|---|---|---|
| Им. | щитови́дка | щитови́дки |
| Р. | щитови́дки | щитови́док |
| Д. | щитови́дке | щитови́дкам |
| В. | щитови́дку | щитови́дки |
| Тв. | щитови́дкой щитови́дкою |
щитови́дками |
| Пр. | щитови́дке | щитови́дках |
щитови́дка
Существительное, неодушевлённое, женский род, 1-е склонение (тип склонения 3*a по классификации А. А. Зализняка).
Корень: -щит-; интерфикс: -о-; корень: -вид-; суффикс: -к; окончание: -а.
Произношение[править]
- МФА: ед. ч. [ɕːɪtɐˈvʲitkə], мн. ч. [ɕːɪtɐˈvʲitkʲɪ]
Семантические свойства[править]
Значение[править]
- разг. щитовидная железа ◆ Отсутствует пример употребления (см. рекомендации).
Синонимы[править]
Антонимы[править]
Гиперонимы[править]
Гипонимы[править]
Родственные слова[править]
| Ближайшее родство | |
Этимология[править]
Происходит от ??
Фразеологизмы и устойчивые сочетания[править]
Перевод[править]
| Список переводов | |
Библиография[править]
- Словарь новых слов русского языка (середина 50-х — середина 80-х годов) / Под ред. Н. З. Котеловой. — СПб. : Дмитрий Буланин, 1995. — ISBN 5-86007-016-0.
|
|
Для улучшения этой статьи желательно:
|
Щитовидная железа расположена в передней части шеи и вырабатывает гормоны щитовидной железы трийодтиронин (Т3) и тетрайодтиронин или тироксин (Т4). Эти гормоны щитовидной железы обеспечивают основной обмен веществ в организме и влияют на работу головного мозга, сердца, мышц и других органов.
Выброс гормонов щитовидной железы регулируется гипофизом, расположенным в головном мозге. Тиреотропный гормон (ТТГ) высвобождается в гипофизе и определяет продукцию Т3 и Т4 в щитовидной железе. Если гормонов щитовидной железы слишком много, то ТТГ снижается, тогда как если гормонов щитовидной железы слишком мало, то ТТГ увеличивается, чтобы стимулировать высвобождение большего количества гормонов щитовидной железы.
Отклонения в работе щитовидки
При заболеваниях щитовидной железы может наблюдаться:
- повышение активности щитовидной железы, называемое гипертиреозом;
- снижение активности щитовидной железы, называемое гипотиреозом.
Нередко в щитовидной железе образуются узлы, в этом случае может быть как нормальная, так и нарушенная функция щитовидной железы.
Гипертиреоз
При гипертиреозе щитовидная железа выделяет слишком много гормона щитовидной железы, что ускоряет обмен веществ в организме. Гипертиреоз может быть разной степени тяжести.
Жалобы, характерные для пациентов с гипертиреозом:
- тахикардия, аритмия;
- повышенная потливость, плохая переносимость жары;
- нервозность, раздражительность, повышенная эмоциональность;
- тремор тела, чаще тремор рук;
- частые испражнения, диарея;
- повышенный аппетит;
- снижение веса при нормальном или даже повышенном аппетите;
- менструальные расстройства;
- нарушения сна;
- увеличение щитовидной железы;
- слабость;
- тонкие волосы, выпадение волос.
Наиболее частыми причинами гипертиреоза – болезнь Грейвса или, реже, один или несколько узлов щитовидной железы, секретирующих повышенные уровни гормонов щитовидной железы.
Что такое болезнь Грейвса?
Это аутоиммунное заболевание, впервые описанное ирландским врачом Робертом Джеймсом Грейвом. При аутоиммунном заболевании щитовидной железы иммунная система, обычно защищающая организм и помогающая бороться с болезнью, вырабатывает антитела, «атакующие» ткани щитовидной железы.
Эти антитела «ведут себя» как тиреотропный гормон (ТТГ), и в результате щитовидная железа вырабатывает слишком много гормона. Болезнь Грейвса может начаться в любом возрасте у обоих полов, но чаще встречается у женщин в возрасте от 20 до 50 лет, у которых часто есть семейная история заболеваний щитовидной железы.
Каковы осложнения болезни Грейвса?
Гипертиреоз, если его не лечить, может привести к сердечной недостаточности и остеопорозу. Беременные женщины с неконтролируемой болезнью Грейвса подвергаются большему риску выкидыша и преждевременных родов.
Болезнь Грейвса вызывает проблемы с глазами, называемые болезнью Грейвса или аутоиммунной офтальмопатией. Характеризуется:
- выпячиванием глазных яблок или экзофтальмом;
- сухостью глаз, покраснением, слезотечением;
- светобоязнью;
- ограничением движения глазного яблока;
- двоением, воспалением, нарушениями зрения.
Как лечится болезнь Грейвса?
Если человек курит, очень важно бросить курить. Заболевание обычно лечат препаратами, снижающими выработку гормонов щитовидной железы, но лечение необходимо проводить под наблюдением врача в течение длительного времени, не менее года, чаще дольше. В некоторых случаях также используется терапия радиоактивным йодом или хирургическое вмешательство.
Гипотиреоз
При гипотиреозе щитовидная железа выделяет слишком мало гормона щитовидной железы, что замедляет обмен веществ в организме. Следует отметить, что жалобы, характерные для больных гипотиреозом, могут различаться по степени выраженности и не всегда могут быть одинаковыми для всех.
Жалобы, характерные для больных с гипотиреозом:
- усталость, сонливость;
- фривольность;
- запор;
- сухая кожа;
- увеличение веса;
- медленный сердечный ритм;
- отеки;
- высокий уровень холестерина в крови;
- охриплость;
- мышечная слабость;
- депрессия;
- нерегулярный менструальный цикл;
- тонкие волосы;
- нарушение памяти.
Причины гипотиреоза:
- тиреоидит Хашимото – аутоиммунное заболевание щитовидной железы, впервые описанное японским врачом Хакару Хашимото;
- операция на щитовидной железе;
- лечение щитовидной железы радиоактивным йодом;
- врожденная проблема со щитовидной железой;
- повреждение гипофиза – в результате чего он не вырабатывает ТТГ.
Тиреоидит Хашимото чаще всего встречается у женщин среднего возраста – 50-60 лет, но может возникать в любом возрасте и может встречаться у мужчин, детей и подростков.
Гипотиреоз у детей и подростков имеет те же симптомы, что и у взрослых, но может отмечаться:
- более медленным ростом;
- задержкой полового созревания;
- задержкой умственного развития.
Гипотиреоз очень важно лечить и контролировать во время беременности. Как правило, беременным женщинам с тиреоидитом Хашимото требуется более высокая доза левотироксина во время беременности, чем до беременности.
Нелеченный гипотиреоз у матери может привести к:
- патологии новорожденных;
- повышенному риску преждевременных родов или мертворождений;
- нарушению психического развития.
Как лечить гипотиреоз?
Пациентам с гипотиреозом следует ежедневно принимать таблетку, содержащую гормон щитовидной железы, для возмещения дефицита гормона в организме. Синтетический Т4 или левотироксин точно такой же и работает так же, как Т4, произведенный организмом. Доза индивидуальна для каждого человека – может потребоваться некоторое время, чтобы найти нужную дозу.
Врач определит начальную дозу в зависимости от веса пациента, возраста и других условий. Через 6-8 недель потребуются анализы крови для корректировки необходимой дозы до тех пор, пока не будет достигнут нормальный уровень гормонов. Тестирование следует продолжать проводить каждые 6–12 месяцев. При гипотиреозе левотироксин обычно следует применять до конца жизни для обеспечения стабильного и нормального обмена веществ в организме.
Антитела к тиреопероксидазе
Тиреопероксидаза представляет собой фермент щитовидной железы, играющий важную роль в синтезе тиреоидных гормонов. В крови могут быть обнаружены антитела к тиреопероксидазе (ТПО av). Высокие уровни TPO av указывают на возможное аутоиммунное заболевание щитовидной железы. Ими могут быть болезнь Грейвса или тиреоидит Хашимото.
Аутоиммунные заболевания характеризуются тем, что иммунная система ошибочно вырабатывает антитела, повреждающие нормальные ткани организма, в данном случае щитовидную железу. Повышенные антитела к ТПО указывают на риск заболевания щитовидной железы, но могут быть случаи, когда эти антитела высоки, а гормоны щитовидной железы находятся в пределах нормы. В таких случаях лечение не требуется, но следует периодически проводить анализы на гормоны щитовидной железы под наблюдением врача.
Узлы щитовидной железы
Узлы в щитовидной железе встречаются часто. Примерно у половины людей в какой-то момент жизни могут появиться узлы щитовидной железы, обычно они незначительны, но в некоторых случаях могут стать большими и повлиять на нормальный размер щитовидной железы.
Примерно у 5% людей появляются крупные узлы размером более 1 см. Большинство узлов доброкачественные. Но всегда необходимо оценить, действительно ли узлы доброкачественные.
Иногда щитовидная железа выделяет больше тиреоидных гормонов, тогда развивается гипертиреоз. Для обследования таких узлов предназначено специальное обследование – сцинтиграфия. При сцинтиграфии щитовидной железы получают цветное изображение, по которому можно судить об активности узелков. Узлы, повышающие выброс гормонов железы, образно называют «горячими» узлами. Большие узлы в щитовидной железе могут вызвать стеснение в горле и затрудненное глотание или дыхание. Тогда немедленно обратитесь к врачу.
Щитовидная железа может быть увеличена без узлов или с узлами. Она может содержать кисты. Киста представляет собой полость, заполненную жидкостью, и обычно доброкачественная. Врач может нащупать более крупные узлы, исследуя щитовидную железу.
Лучший способ их оценки – проведение УЗИ щитовидной железы. В ходе него опытный специалист описывает форму узлов, диаметр и т. д., а их доброкачественность оценивают, классифицируя их по шкале TIRADS:
|
Показатель по шкале TIRADS |
Оценка |
|
1, 2, 3 |
доброкачественные узлы |
|
4 |
повышенный риск малигнизации или озлокачествления – приобретение клетками нормальной или патологически измененной ткани железы свойств злокачественной опухоли |
|
5 |
узлы очень высокого риска, скорее всего, злокачественные |
При необходимости врач назначит пункцию щитовидной железы под контролем УЗИ. Этот тест проводится с помощью тонкой иглы, вводимой в щитовидную железу под контролем УЗИ, и клетки удаляются из узла. Их затем исследуют под микроскопом. Это обследование — лучший способ убедиться, что узел действительно доброкачественный.
Доброкачественные узлы щитовидной железы не требуют лечения. «Горячие» узлы оперируют или лечат радиоактивным йодом. Узлы щитовидной железы, вызывающие такие симптомы затрудненного глотания или дыхания, должны быть прооперированы. Операции следует проводить во всех случаях подозрения на узловое злокачественное новообразование.
Если во время хирургического вмешательства удаляется вся щитовидная железа, то после операции необходимо использовать тиреоидные гормоны всю оставшуюся жизнь.
Болезни щитовидной железы: причины появления, симптомы, диагностика и способы лечения.
Определение
Щитовидная железа (ЩЖ) — железа внутренней секреции, расположенная на передней поверхности шеи, состоящая из двух долей и перешейка.
ЩЖ секретирует йодированные гормоны Т4 (тироксин) и Т3 (трийодтиронин), а также нейодированный гормон кальцитонин.
Основные компоненты, необходимые для образования тиреоидных гормонов — йод и аминокислота тирозин.
Йод поступает в организм с пищей и водой, всасывается в кровь из желудочно-кишечного тракта. Суточная потребность организма в йоде составляет 110–150 мкг/сут.
Регуляция синтеза и секреции гормонов ЩЖ осуществляется через гипоталамо-гипофизарную систему. Гипоталамус секретирует тиролиберин (ТРГ), который стимулирует выделение гипофизом тиреотропного гормона (ТТГ), который, в свою очередь, регулирует рост и функцию щитовидной железы. Между гипоталамусом, гипофизом и ЩЖ существует и обратная связь (избыток йодсодержащих гормонов вызывает снижение тиреотропной функции гипофиза).

Тиреоидные гормоны влияют на все виды обмена: водно-электролитный, белковый, жировой, углеводный и энергетический. Наличие адекватного количества гормонов ЩЖ — необходимое условие для нормального функционирования центральной нервной системы.
Третий гормон щитовидной железы — кальцитонин участвует в метаболизме кальция, препятствуя его вымыванию из костной ткани и тем самым снижая его концентрацию в крови.
Причины заболеваний щитовидной железы
- Нарушение синтеза гормонов:
- из-за недостатка или избытка поступления йода в организм;
- из-за врожденных дефектов развития ЩЖ;
- из-за оперативных вмешательств на ЩЖ;
- из-за применения радиоактивного йода;
- из-за аутоиммунных повреждений;
- из-за воспалительных повреждений.
- Изменение функционального состояния центральной нервной системы.
- Невосприимчивость тканей организма к тиреоидным гормонам.
- Влияние лекарственных препаратов.
Дефицит йода приводит к снижению концентрации тиреоидных гормонов в крови. В результате усиливается продукция тиреотропного гормона, что приводит к компенсаторному увеличению количества тиреоцитов (клеток щитовидной железы). Так развиваются эндемический и спорадический зоб.
Эндемический зоб – увеличение щитовидной железы, возникающее у людей, проживающих в определенных географических районах с недостаточностью йода в окружающей среде. Спорадический зоб выявляют у людей, проживающих в неэндемических районах.
Помимо дефицита йода в образовании нетоксического зоба важную роль могут играть и другие факторы: аутоиммунные, генетические (изменение порога чувствительности к недостатку йода в пище; дефекты ферментных систем, участвующих в синтезе тиреоидных гормонов), пониженное содержание в окружающей среде микроэлементов (кобальта, меди, цинка, молибдена), поступление с пищей зобогенных веществ (тиоцинатов, тиооксизолидонов).
Вирусы, тропные к клеткам щитовидной железы, могут быть пусковым механизмом развития гиперпродукции тиреоидных гормонов.
Лимфоциты щитовидной железы начинают вырабатывать антитела к рецепторам клеточных мембран собственных клеток. Эти антитела оказывают стимулирующее действие на щитовидную железу. В результате нарушения центральной регуляции ситуация выходит из-под контроля, развивается диффузный токсический зоб. Существуют также данные о наследственной предрасположенности к диффузному токсическому зобу.
 Причинами снижения уровня гормонов ЩЖ в крови могут быть:
Причинами снижения уровня гормонов ЩЖ в крови могут быть:
- врожденная аплазия (отсутствие органа) или гипоплазия (недоразвитие органа) щитовидной железы;
- генетически обусловленное нарушение синтеза гормонов в железе;
- недостаток йода в пище;
- избыток йода при приеме матерью йодсодержащих препаратов;
- уменьшение массы функционирующей тиреоидной ткани (аутоиммунный тиреоидит, оперативное вмешательство на щитовидной железе, гнойный тиреоидит, заболевания гипофиза или гипоталамуса).
В результате стойкого снижения уровня гормонов ЩЖ возникает гипотиреоз со сложной клинической картиной.
Причины возникновения воспаления щитовидной железы (тиреоидита) могут быть разными. Имеется связь развития заболевания с перенесенными бактериальными, грибковыми, вирусными заболеваниями лор-органов или поражениями легких преимущественно у лиц с ослабленным иммунитетом.
Инфекция проникает в ЩЖ с током крови, по лимфатическим путям или в результате прямого попадания при травме, ранении, медицинских манипуляций. В результате развивается тиреоидит. У детей чаще имеется связь заболевания с α- и β-гемолитическими стрептококками и разнообразными анаэробными бактериями.
В результате применения некоторых лекарственных средств (интерферонов, интерлейкинов, моноклональных антител, препаратов лития, йодсодержащего рентгеноконтрастного вещества и др.) могут возникнуть медикаментозные тиреоидиты.
В основе нарушения функции щитовидной железы могут лежать изменения функционального состояния центральной нервной системы, в частности гипоталамуса и гипофиза (травма, кровоизлияние, некроз, хирургическое и лучевое удаление гипофиза). Изменение продукции гипофизом тиреотропного гормона приводит не только к изменению функции щитовидной железы, но и к диффузным или узловым патологиям ее ткани.
Аномалии развития щитовидной железы у плода могут стать результатом неблагоприятного воздействия на организм матери во время беременности.
Зачаток щитовидной железы возникает на 2-4-й неделе внутриутробного развития и возможны два вида нарушений развития. Зачаток ЩЖ может задержаться на месте первоначальной закладки или спуститься необычно низко. В подобных случаях щитовидная железа отсутствует на своем обычном месте, располагаясь в нетипичном для себя месте (например, в средостенье).
Наследственный синдром резистентности тканей к тиреоидным гормонам обычно возникает из-за приобретенной мутации генов (у 22% больных) или передаться по наследству от родителей (в 78% случаев).
Для образования доброкачественных опухолей щитовидной железы имеют значение многие факторы: йододефицит, неблагоприятные условия проживания в крупных мегаполисах, работа на вредном предприятии, радиоактивное облучение, генетическая предрасположенность, резкие гормональные перестройки у женщин во время беременности или климакса и другие факторы.
Злокачественные опухоли щитовидной железы составляют около 1-3% среди всех онкологических заболеваний. Рак щитовидной железы наблюдается у женщин примерно в 3 раза чаще, чем у мужчин.
Согласно литературным данным, рак щитовидной железы возникает на фоне определенных предшествующих изменений — зоба, аденомы, аутоиммунного тиреоидита и проходит стадии развития от диффузной гиперплазии (увеличения количества клеток ЩЖ) до злокачественной опухоли.
Некоторые лекарственные препараты могут изменять уровень гомонов щитовидной железы в крови.
Прием антитиреоидных средств, анаболических стероидов, бета-адреноблокаторов, глюкокортикоидов, нестероидных противовоспалительных средств, оральных контрацептивов, гиполипидемических средств, рентгеноконтрастных средств понижают уровень гормонов. Применение амиодарона, эстрогенов, левотироксина, оральных контрацептивов, кортикостероидов и др., напротив, повышает уровень гормонов ЩЖ.
Таким образом, в развитии одного заболевания, могут иметь значение несколько факторов. И наоборот, один и тот же фактор у разных людей может вызвать разные изменения в щитовидной железе.
Классификация заболеваний щитовидной железы
I. Врожденные аномалии щитовидной железы:
- гипоплазия и аплазия ЩЖ,
- эктопия ЩЖ,
- незаращение щитовидно-язычного протока.
II. Эндемический зоб.
III. Спорадический зоб.
IV. Диффузный токсический зоб.
V. Гипотиреоз.
VI. Воспалительные заболевания щитовидной железы.
VII. Травмы ЩЖ.
VIII. Опухоли ЩЖ:
- доброкачественные новообразования,
- злокачественные опухоли.
Симптомы заболеваний щитовидной железы
- Изменение размера железы, в том числе с появлением узлового образования.
- Воспаление щитовидной железы.
- Нарушения функции ЩЖ (повышение или снижение функции).
Воспаление щитовидной железы может начинаться остро, как например, при остром тиреоидите, так и более гладко — при подостром тиреоидите.
Острый тиреоидит, вызванный бактериальной инфекцией, начинается с лихорадки, головной боли, сильной боли и дискомфортных ощущений в области щитовидной железы. Причинами болевого синдрома являются отек щитовидной железы и растяжение ее капсулы. При осмотре определяется опухолевидное образование на передней поверхности шеи, покраснение кожи. При ощупывании определяется увеличенная, болезненная щитовидная железа. При присоединении гнойного процесса температура тела повышается до 39–40°С, усиливается боль, отмечается расплавление тканей и образованием гнойной полости (абсцедирование).
В период, предшествующий развитию подострого тиреоидита, могут наблюдаться боли в мышцах и в горле, недомогание, субфебрильная лихорадка, общая слабость, утомляемость. Затем появляется умеренная или сильная боль в области щитовидной железы. ЩЖ увеличена и болезненна при ощупывании, наблюдается разрастание соединительной ткани, проявляющееся повышением ее плотности.
При тиреоидите Риделя происходит замещение ткани щитовидной железы на фиброзную. При этом развивается зоб деревянистой плотности. В процесс вовлекается не только сама железа, но и окружающие анатомические структуры: трахея, пищевод, сосуды, нервы, мышцы. Заболевание развивается медленно.
Нарушения функции ЩЖ сопровождаются изменением уровня гормонов в крови (гипофункция или гиперфункция).
У больных с гипофункцией щитовидной железы развиваются вялость, медлительность, сонливость, быстрая утомляемость, замедленное мышление и речь, снижение памяти, эмоциональная лабильность, чувство тревоги, галлюцинации вплоть до психоза. Наблюдаются зябкость и плохая переносимость холода, бледная, шелушащаяся, холодная кожа, отеки лица и конечностей, пастозность и маскообразность лица, увеличение языка. Выпадение волос и повышение ломкости ногтей. Грубый, сиплый голос. Увеличивается масса тела при сниженном аппетите. Могут быть нарушения сердечной деятельности — брадикардия, у 10% наблюдается учащение пульса, у 10-50% пациентов — повышение артериального давления. Больные могут быть склонны к бронхитам, пневмонии, которые отличаются вялым затяжным течением. Могут наблюдаться желудочно-кишечные расстройства: снижение аппетита, тошнота, вздутие кишечника (метеоризм), запоры, застой желчи и образование камней в желчевыводящих путях.
Возникающий в организме избыток гормонов щитовидной железы при таких заболеваниях как диффузный токсический зоб, рак ЩЖ, аденома гипофиза, хорионэпителиома и др., также влияет на различные органы и системы. Кожа становится горячей на ощупь и сухой, волосы — сухими и ломкими. Пациенты жалуются на тремор пальцев рук. Возникает повышенная нервная возбудимость, плаксивость, потливость, чувство жара, небольшие колебания температуры, суетливость. Могут быть внезапные приступы мышечной слабости. Характерными симптомами гиперфункции ЩЖ считаются припухлость верхних век и их гиперпигментация, редкое мигание, пучеглазие, слезотечение, светобоязнь и чувство «песка в глазах».
Даже при повышенном аппетите больные могут терять вес за счет ускоренного обмена веществ.
В связи с влиянием гормонов ЩЖ на сердечно-сосудистую систему больных беспокоят нарушения ритма сердца. Со стороны органо ЖКТ могут наблюдаться приступы болей в животе, рвота, расстройство стула, иногда запоры. В тяжелых случаях поражается печень. У женщин может быть нарушение менструального цикла. У мужчин снижается либидо, потенция, может развиваться гинекомастия.
Диагностика заболеваний щитовидной железы
Диагностические мероприятия начинаются с осмотра ЩЖ, во время которого можно обнаружить деформацию шеи, что свидетельствует об увеличении доли железы, ее перешейка или регионарных лимфоузлов. Кожа над железой может быть покрасневшей с выраженным сосудистым рисунком, на шее и на передней поверхности грудной клетки видны расширенные вены.
При пальпации щитовидной железы могут быть обнаружены узлы. Округлая, сферическая поверхность узла характерна для доброкачественных процессов, а плоская, неровная — для злокачественных новообразований.
При аномалиях развития щитовидной железы она может не обнаруживаться на шее, а опухолевидное образование может располагаться на корне языка, переднем средостенье.
Лабораторная диагностика заболеваний ЩЖ должна быть комплексной и включать:
- клинический анализ крови с определением концентрации гемоглобина, количества эритроцитов, лейкоцитов и тромбоцитов, величины гематокрита и эритроцитарных индексов (MCV, RDW, MCH, MCHC), лейкоформулу и СОЭ (с микроскопией мазка крови при наличии патологических сдвигов);
К каким врачам обращаться
При подозрении на заболевание щитовидной железы необходимо обратиться к
врачу-терапевту
или врачу общей практики. При подтверждении диагноза после проведения комплекса лабораторно-диагностических мероприятий лечение назначает
врач-эндокринолог
. При необходимости пациент может быть направлен к
онкологу
или хирургу.
Лечение заболеваний щитовидной железы
При заболеваниях щитовидной железы используют три метода лечения:
- медикаментозную терапию;
- хирургическое вмешательство;
- лечение радиоактивным йодом.
Лечение может быть комбинированным. Метод лечения определяется индивидуально, его выбор зависит от основной причины заболевания, сопутствующих заболеваний, показаний и противопоказаний к лечению, размеров щитовидной железы, возраста больного.
Медикаментозное лечение используется как в качестве самостоятельного метода, так и для подготовки к оперативному вмешательству.
Подбор дозы осуществляется индивидуально, лечение может быть длительным и непрерывным.
Показания к хирургическому лечению заболеваний ЩЖ:
- опухоли щитовидной железы;
- большие размеры ЩЖ со сдавлением или смещением трахеи, крупных сосудов, пищевода;
- загрудинное расположение щитовидной железы;
- тяжелые формы тиреотоксикоза, осложненные мерцательной аритмией;
- неэффективность проводимой медикаментозной терапии;
- непереносимость тиреотоксических препаратов;
- гормонально-активные опухоли;
- абсцедирование и/или наличие осложнений (свищи, медиастинит) при тиреоидитах.
Лечебное действие радиоактивного йода основано на разрушении клеток эпителия железы и применяется главным образом у пожилых больных с тяжелыми сопутствующими заболеваниями.
Показания к лечению:
- гипертиреоз;
- тиреотоксикоз;
- любой вид рака щитовидной железы;
- узловой токсический зоб;
- рецидив после проведенной операции.
Осложнения
- Самопроизвольное вскрытие абсцесса в просвет трахеи пищевода или в средостение с развитием медиастинита.
- Медиастинит (воспалительный процесс в клетчатке средостенья).
- Флегмона шеи (гнойно-воспалительное заболевание с вовлечением в процесс глубоких клетчаточных пространств шеи).
- Сдавление органов шеи.
- Сепсис (системная воспалительная реакция организма в ответ на распространение местного инфекционного процесса с развитием токсемии и бактериемии).
- Свищ щитовидной железы с трахеей (канал, соединяющий щитовидную железу с просветом трахеи).
- Озлокачествление опухоли.
Профилактика заболеваний щитовидной железы
При появлении первых признаков проблем со ЩЖ необходимо обратиться к врачу. На ранней стадии заболевания больные хорошо реагируют на терапию.
Поздняя диагностика чревата развитием осложнений и даже потерей трудоспособности.
Важны профилактические осмотры, регулярные контрольные приемы у лечащего врача с целью коррекции лечения.
Источники:
- Клинические рекомендации «Заболевания и состояния, связанные с дефицитом йода». Разраб.: Российская ассоциация эндокринологов. – 2020
- Е.А. Валдина. Заболевания щитовидной железы: Руководство. 3-е изд. — СПб: Питер, 2006. — 368 с.
- Система поддержки принятия врачебных решений «Эндокринология Клинические протоколы лечения». Согласовано: д.м.н., проф. Анциферов М.Б.
ВАЖНО!
Информацию из данного раздела нельзя использовать для самодиагностики и самолечения. В случае боли или иного обострения заболевания диагностические исследования должен назначать только лечащий врач. Для постановки диагноза и правильного назначения лечения следует обращаться к Вашему лечащему врачу.
Для корректной оценки результатов ваших анализов в динамике предпочтительно делать исследования в одной и той же лаборатории, так как в разных лабораториях для выполнения одноименных анализов могут применяться разные методы исследования и единицы измерения.