Как правильно пишется слово «туберкулёз»
туберкулёз
туберкулёз, -а
Источник: Орфографический
академический ресурс «Академос» Института русского языка им. В.В. Виноградова РАН (словарная база
2020)
Делаем Карту слов лучше вместе

Привет! Меня зовут Лампобот, я компьютерная программа, которая помогает делать
Карту слов. Я отлично
умею считать, но пока плохо понимаю, как устроен ваш мир. Помоги мне разобраться!
Спасибо! Я стал чуточку лучше понимать мир эмоций.
Вопрос: сердар — это что-то нейтральное, положительное или отрицательное?
Ассоциации к слову «туберкулёз»
Синонимы к слову «туберкулёз»
Синонимы к слову «туберкулез»
Предложения со словом «туберкулёз»
- Гемограммау больных туберкулёзом детей имеет различные значения в зависимости от возраста, наличия контакта, формы и фазы заболевания.
- По мнению некоторых учёных, конники не болеют туберкулёзом лёгких, потому что микроклимат конюшни, подвижная работа с лошадьми, езда на них помогают естественной дезинфекции и вентиляции лёгких.
- О хирургическом лечении туберкулёза лёгких было сделано 10 докладов.
- (все предложения)
Цитаты из русской классики со словом «туберкулёз»
- — Мне черного пива, — сказал Долганов. — Пиво — полезно. Я — из Давоса. Туберкулез. Пневматоракс. Схватил в Тотьме, в ссылке. Тоже — дыра, как Давос. Соскучился о людях. Вы — эмигрировали?
- Скоро она исчезла из института, а лет через пятнадцать я встретил ее учительницей в одной крымской гимназии, она страдала туберкулезом и говорила обо всем в мире с беспощадной злобой человека, оскорбленного жизнью.
- Вот состав умерших от туберкулеза по возрастам:
- (все
цитаты из русской классики)
Каким бывает «туберкулёз»
Значение слова «туберкулёз»
-
ТУБЕРКУЛЁЗ, -а, м. Инфекционное заболевание, вызываемое особым микробом и поражающее различные органы (чаще всего легкие, кишечник, кости и суставы). (Малый академический словарь, МАС)
Все значения слова ТУБЕРКУЛЁЗ
Отправить комментарий
Дополнительно
Смотрите также
ТУБЕРКУЛЁЗ, -а, м. Инфекционное заболевание, вызываемое особым микробом и поражающее различные органы (чаще всего легкие, кишечник, кости и суставы).
Все значения слова «туберкулёз»
-
Гемограммау больных туберкулёзом детей имеет различные значения в зависимости от возраста, наличия контакта, формы и фазы заболевания.
-
По мнению некоторых учёных, конники не болеют туберкулёзом лёгких, потому что микроклимат конюшни, подвижная работа с лошадьми, езда на них помогают естественной дезинфекции и вентиляции лёгких.
-
О хирургическом лечении туберкулёза лёгких было сделано 10 докладов.
- (все предложения)
- болезнь
- чахотка
- бугорчатка
- волчанка
- горловая чахотка
- (ещё синонимы…)
- чахотка
- (ещё синонимы…)
- кашель
- лёгкие
- рентген
- курильщик
- болезнь
- (ещё ассоциации…)
- больной туберкулёзом
- туберкулёз лёгких
- больные туберкулёзом
- заболеть туберкулёзом
- (полная таблица сочетаемости…)
- костный
- больной
- активный
- лёгочный
- милиарный
- (ещё…)
- Склонение
существительного «туберкулёз» - Разбор по составу слова «туберкулёз»
| Tuberculosis | |
|---|---|
| Other names | Phthisis, phthisis pulmonalis, consumption, great white plague |
 |
|
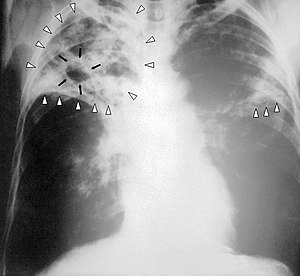
| Chest X-ray of a person with advanced tuberculosis: Infection in both lungs is marked by white arrow-heads, and the formation of a cavity is marked by black arrows. | |
| Specialty | Infectious disease, pulmonology |
| Symptoms | Chronic cough, fever, cough with bloody mucus, weight loss[1] |
| Causes | Mycobacterium tuberculosis[1] |
| Risk factors | Smoking, HIV/AIDS[1] |
| Diagnostic method | CXR, culture, tuberculin skin test, QuantiFERON[1] |
| Differential diagnosis | Pneumonia, histoplasmosis, sarcoidosis, coccidioidomycosis[2] |
| Prevention | Screening those at high risk, treatment of those infected, vaccination with bacillus Calmette-Guérin (BCG)[3][4][5] |
| Treatment | Antibiotics[1] |
| Frequency | 25% of people (latent TB)[6] |
| Deaths | 1.5 million (2020)[7] |

Depiction of a man with tuberculosis
Tuberculosis (TB) is an infectious disease usually caused by Mycobacterium tuberculosis (MTB) bacteria.[1] Tuberculosis generally affects the lungs, but it can also affect other parts of the body.[1] Most infections show no symptoms, in which case it is known as latent tuberculosis.[1] Around 10% of latent infections progress to active disease which, if left untreated, kill about half of those affected.[1] Typical symptoms of active TB are chronic cough with blood-containing mucus, fever, night sweats, and weight loss.[1] It was historically referred to as consumption due to the weight loss associated with the disease.[8] Infection of other organs can cause a wide range of symptoms.[9]
Tuberculosis is spread from one person to the next through the air when people who have active TB in their lungs cough, spit, speak, or sneeze.[1][10] People with Latent TB do not spread the disease.[1] Active infection occurs more often in people with HIV/AIDS and in those who smoke.[1] Diagnosis of active TB is based on chest X-rays, as well as microscopic examination and culture of body fluids.[11] Diagnosis of Latent TB relies on the tuberculin skin test (TST) or blood tests.[11]
Prevention of TB involves screening those at high risk, early detection and treatment of cases, and vaccination with the bacillus Calmette-Guérin (BCG) vaccine.[3][4][5] Those at high risk include household, workplace, and social contacts of people with active TB.[4] Treatment requires the use of multiple antibiotics over a long period of time.[1] Antibiotic resistance is a growing problem with increasing rates of multiple drug-resistant tuberculosis (MDR-TB).[1]
In 2018, one quarter of the world’s population was thought to have a latent infection of TB.[6] New infections occur in about 1% of the population each year.[12] In 2020, an estimated 10 million people developed active TB, resulting in 1.5 million deaths, making it the second leading cause of death from an infectious disease after COVID-19.[13] As of 2018, most TB cases occurred in the regions of South-East Asia (44%), Africa (24%), and the Western Pacific (18%), with more than 50% of cases being diagnosed in seven countries: India (27%), China (9%), Indonesia (8%), the Philippines (6%), Pakistan (6%), Nigeria (4%), and Bangladesh (4%).[14] By 2021 the number of new cases each year was decreasing by around 2% annually.[13][1] About 80% of people in many Asian and African countries test positive while 5–10% of people in the United States population test positive via the tuberculin test.[15] Tuberculosis has been present in humans since ancient times.[16]
Signs and symptoms

The main symptoms of variants and stages of tuberculosis are given,[17] with many symptoms overlapping with other variants, while others are more (but not entirely) specific for certain variants. Multiple variants may be present simultaneously.
Tuberculosis may infect any part of the body, but most commonly occurs in the lungs (known as pulmonary tuberculosis).[9] Extrapulmonary TB occurs when tuberculosis develops outside of the lungs, although extrapulmonary TB may coexist with pulmonary TB.[9]
General signs and symptoms include fever, chills, night sweats, loss of appetite, weight loss, and fatigue.[9] Significant nail clubbing may also occur.[18]
Pulmonary
If a tuberculosis infection does become active, it most commonly involves the lungs (in about 90% of cases).[16][19] Symptoms may include chest pain and a prolonged cough producing sputum. About 25% of people may not have any symptoms (i.e., they remain asymptomatic).[16] Occasionally, people may cough up blood in small amounts, and in very rare cases, the infection may erode into the pulmonary artery or a Rasmussen’s aneurysm, resulting in massive bleeding.[9][20] Tuberculosis may become a chronic illness and cause extensive scarring in the upper lobes of the lungs. The upper lung lobes are more frequently affected by tuberculosis than the lower ones.[9] The reason for this difference is not clear.[15] It may be due to either better air flow,[15] or poor lymph drainage within the upper lungs.[9]
In 15–20% of active cases, the infection spreads outside the lungs, causing other kinds of TB.[21] These are collectively denoted as extrapulmonary tuberculosis. Extrapulmonary TB occurs more commonly in people with a weakened immune system and young children. In those with HIV, this occurs in more than 50% of cases. Notable extrapulmonary infection sites include the pleura (in tuberculous pleurisy), the central nervous system (in tuberculous meningitis), the lymphatic system (in scrofula of the neck), the genitourinary system (in urogenital tuberculosis), and the bones and joints (in Pott disease of the spine), among others. A potentially more serious, widespread form of TB is called «disseminated tuberculosis», it is also known as miliary tuberculosis.[9] Miliary TB currently makes up about 10% of extrapulmonary cases.[23]
Causes
Mycobacteria

The main cause of TB is Mycobacterium tuberculosis (MTB), a small, aerobic, nonmotile bacillus.[9] The high lipid content of this pathogen accounts for many of its unique clinical characteristics.[24] It divides every 16 to 20 hours, which is an extremely slow rate compared with other bacteria, which usually divide in less than an hour.[25] Mycobacteria have an outer membrane lipid bilayer.[26] If a Gram stain is performed, MTB either stains very weakly «Gram-positive» or does not retain dye as a result of the high lipid and mycolic acid content of its cell wall.[27] MTB can withstand weak disinfectants and survive in a dry state for weeks. In nature, the bacterium can grow only within the cells of a host organism, but M. tuberculosis can be cultured in the laboratory.[28]
Using histological stains on expectorated samples from phlegm (also called sputum), scientists can identify MTB under a microscope. Since MTB retains certain stains even after being treated with acidic solution, it is classified as an acid-fast bacillus.[15][27] The most common acid-fast staining techniques are the Ziehl–Neelsen stain[29] and the Kinyoun stain, which dye acid-fast bacilli a bright red that stands out against a blue background.[30] Auramine-rhodamine staining[31] and fluorescence microscopy[32] are also used.
The M. tuberculosis complex (MTBC) includes four other TB-causing mycobacteria: M. bovis, M. africanum, M. canetti, and M. microti.[33] M. africanum is not widespread, but it is a significant cause of tuberculosis in parts of Africa.[34][35] M. bovis was once a common cause of tuberculosis, but the introduction of pasteurized milk has almost eliminated this as a public health problem in developed countries.[15][36] M. canetti is rare and seems to be limited to the Horn of Africa, although a few cases have been seen in African emigrants.[37][38] M. microti is also rare and is seen almost only in immunodeficient people, although its prevalence may be significantly underestimated.[39]
Other known pathogenic mycobacteria include M. leprae, M. avium, and M. kansasii. The latter two species are classified as «nontuberculous mycobacteria» (NTM) or atypical mycobacteria. NTM cause neither TB nor leprosy, but they do cause lung diseases that resemble TB.[40]

Public health campaigns in the 1920s tried to halt the spread of TB.
Transmission
When people with active pulmonary TB cough, sneeze, speak, sing, or spit, they expel infectious aerosol droplets 0.5 to 5.0 µm in diameter. A single sneeze can release up to 40,000 droplets.[41] Each one of these droplets may transmit the disease, since the infectious dose of tuberculosis is very small (the inhalation of fewer than 10 bacteria may cause an infection).[42]
Risk of transmission
People with prolonged, frequent, or close contact with people with TB are at particularly high risk of becoming infected, with an estimated 22% infection rate.[43] A person with active but untreated tuberculosis may infect 10–15 (or more) other people per year.[44] Transmission should occur from only people with active TB – those with latent infection are not thought to be contagious.[15] The probability of transmission from one person to another depends upon several factors, including the number of infectious droplets expelled by the carrier, the effectiveness of ventilation, the duration of exposure, the virulence of the M. tuberculosis strain, the level of immunity in the uninfected person, and others.[45] The cascade of person-to-person spread can be circumvented by segregating those with active («overt») TB and putting them on anti-TB drug regimens. After about two weeks of effective treatment, subjects with nonresistant active infections generally do not remain contagious to others.[43] If someone does become infected, it typically takes three to four weeks before the newly infected person becomes infectious enough to transmit the disease to others.[46]
Risk factors
A number of factors make individuals more susceptible to TB infection and/or disease.[47]
Active disease risk
The most important risk factor globally for developing active TB is concurrent HIV infection; 13% of those with TB are also infected with HIV.[48] This is a particular problem in sub-Saharan Africa, where HIV infection rates are high.[49][50] Of those without HIV infection who are infected with tuberculosis, about 5–10% develop active disease during their lifetimes;[18] in contrast, 30% of those co-infected with HIV develop the active disease.[18]
Use of certain medications, such as corticosteroids and infliximab (an anti-αTNF monoclonal antibody), is another important risk factor, especially in the developed world.[16]
Other risk factors include: alcoholism,[16] diabetes mellitus (3-fold increased risk),[51] silicosis (30-fold increased risk),[52] tobacco smoking (2-fold increased risk),[53] indoor air pollution, malnutrition, young age,[47] recently acquired TB infection, recreational drug use, severe kidney disease, low body weight, organ transplant, head and neck cancer,[54] and genetic susceptibility[55] (the overall importance of genetic risk factors remains undefined[16]).
Infection susceptibility
Tobacco smoking increases the risk of infections (in addition to increasing the risk of active disease and death). Additional factors increasing infection susceptibility include young age.[47]
Pathogenesis

About 90% of those infected with M. tuberculosis have asymptomatic, latent TB infections (sometimes called LTBI),[57] with only a 10% lifetime chance that the latent infection will progress to overt, active tuberculous disease.[58] In those with HIV, the risk of developing active TB increases to nearly 10% a year.[58] If effective treatment is not given, the death rate for active TB cases is up to 66%.[44]
Microscopy of tuberculous epididymitis. H&E stain
TB infection begins when the mycobacteria reach the alveolar air sacs of the lungs, where they invade and replicate within endosomes of alveolar macrophages.[15][59][60] Macrophages identify the bacterium as foreign and attempt to eliminate it by phagocytosis. During this process, the bacterium is enveloped by the macrophage and stored temporarily in a membrane-bound vesicle called a phagosome. The phagosome then combines with a lysosome to create a phagolysosome. In the phagolysosome, the cell attempts to use reactive oxygen species and acid to kill the bacterium. However, M. tuberculosis has a thick, waxy mycolic acid capsule that protects it from these toxic substances. M. tuberculosis is able to reproduce inside the macrophage and will eventually kill the immune cell.
The primary site of infection in the lungs, known as the Ghon focus, is generally located in either the upper part of the lower lobe, or the lower part of the upper lobe.[15] Tuberculosis of the lungs may also occur via infection from the blood stream. This is known as a Simon focus and is typically found in the top of the lung.[61] This hematogenous transmission can also spread infection to more distant sites, such as peripheral lymph nodes, the kidneys, the brain, and the bones.[15][62] All parts of the body can be affected by the disease, though for unknown reasons it rarely affects the heart, skeletal muscles, pancreas, or thyroid.[63]
Tuberculosis is classified as one of the granulomatous inflammatory diseases. Macrophages, epithelioid cells, T lymphocytes, B lymphocytes, and fibroblasts aggregate to form granulomas, with lymphocytes surrounding the infected macrophages. When other macrophages attack the infected macrophage, they fuse together to form a giant multinucleated cell in the alveolar lumen. The granuloma may prevent dissemination of the mycobacteria and provide a local environment for interaction of cells of the immune system.[64] However, more recent evidence suggests that the bacteria use the granulomas to avoid destruction by the host’s immune system. Macrophages and dendritic cells in the granulomas are unable to present antigen to lymphocytes; thus the immune response is suppressed.[65] Bacteria inside the granuloma can become dormant, resulting in latent infection. Another feature of the granulomas is the development of abnormal cell death (necrosis) in the center of tubercles. To the naked eye, this has the texture of soft, white cheese and is termed caseous necrosis.[64]
If TB bacteria gain entry to the blood stream from an area of damaged tissue, they can spread throughout the body and set up many foci of infection, all appearing as tiny, white tubercles in the tissues.[66] This severe form of TB disease, most common in young children and those with HIV, is called miliary tuberculosis.[67] People with this disseminated TB have a high fatality rate even with treatment (about 30%).[23][68]
In many people, the infection waxes and wanes. Tissue destruction and necrosis are often balanced by healing and fibrosis.[64] Affected tissue is replaced by scarring and cavities filled with caseous necrotic material. During active disease, some of these cavities are joined to the air passages (bronchi) and this material can be coughed up. It contains living bacteria and thus can spread the infection. Treatment with appropriate antibiotics kills bacteria and allows healing to take place. Upon cure, affected areas are eventually replaced by scar tissue.[64]
Diagnosis

Active tuberculosis
Diagnosing active tuberculosis based only on signs and symptoms is difficult,[69] as is diagnosing the disease in those who have a weakened immune system.[70] A diagnosis of TB should, however, be considered in those with signs of lung disease or constitutional symptoms lasting longer than two weeks.[70] A chest X-ray and multiple sputum cultures for acid-fast bacilli are typically part of the initial evaluation.[70] Interferon-γ release assays (IGRA) and tuberculin skin tests are of little use in most of the developing world.[71][72] IGRA have similar limitations in those with HIV.[72][73]
A definitive diagnosis of TB is made by identifying M. tuberculosis in a clinical sample (e.g., sputum, pus, or a tissue biopsy). However, the difficult culture process for this slow-growing organism can take two to six weeks for blood or sputum culture.[74] Thus, treatment is often begun before cultures are confirmed.[75]
Nucleic acid amplification tests and adenosine deaminase testing may allow rapid diagnosis of TB.[69] Blood tests to detect antibodies are not specific or sensitive, so they are not recommended.[76]
Latent tuberculosis

Mantoux tuberculin skin test
The Mantoux tuberculin skin test is often used to screen people at high risk for TB.[70] Those who have been previously immunized with the Bacille Calmette-Guerin vaccine may have a false-positive test result.[77] The test may be falsely negative in those with sarcoidosis, Hodgkin’s lymphoma, malnutrition, and most notably, active tuberculosis.[15] Interferon gamma release assays, on a blood sample, are recommended in those who are positive to the Mantoux test.[75] These are not affected by immunization or most environmental mycobacteria, so they generate fewer false-positive results.[78] However, they are affected by M. szulgai, M. marinum, and M. kansasii.[79] IGRAs may increase sensitivity when used in addition to the skin test, but may be less sensitive than the skin test when used alone.[80]
The US Preventive Services Task Force (USPSTF) has recommended screening people who are at high risk for latent tuberculosis with either tuberculin skin tests or interferon-gamma release assays.[81] While some have recommend testing health care workers, evidence of benefit for this is poor as of 2019.[82] The Centers for Disease Control and Prevention (CDC) stopped recommending yearly testing of health care workers without known exposure in 2019.[83]
Prevention

Tuberculosis public health campaign in Ireland, c. 1905
Tuberculosis prevention and control efforts rely primarily on the vaccination of infants and the detection and appropriate treatment of active cases.[16] The World Health Organization (WHO) has achieved some success with improved treatment regimens, and a small decrease in case numbers.[16] Some countries have legislation to involuntarily detain or examine those suspected to have tuberculosis, or involuntarily treat them if infected.[84]
Vaccines
The only available vaccine as of 2021 is bacillus Calmette-Guérin (BCG).[85][86] In children it decreases the risk of getting the infection by 20% and the risk of infection turning into active disease by nearly 60%.[87]
It is the most widely used vaccine worldwide, with more than 90% of all children being vaccinated.[16] The immunity it induces decreases after about ten years.[16] As tuberculosis is uncommon in most of Canada, Western Europe, and the United States, BCG is administered to only those people at high risk.[88][89][90] Part of the reasoning against the use of the vaccine is that it makes the tuberculin skin test falsely positive, reducing the test’s usefulness as a screening tool.[90] Several vaccines are being developed.[16]
Intradermal MVA85A vaccine in addition to BCG injection is not effective in preventing tuberculosis.[91]
Public health
Public health campaigns which have focused on overcrowding, public spitting and regular sanitation (including hand washing) during the 1800s helped to either interrupt or slow spread which when combined with contact tracing, isolation and treatment helped to dramatically curb the transmission of both tuberculosis and other airborne diseases which led to the elimination of tuberculosis as a major public health issue in most developed economies.[92][93] Other risk factors which worsened TB spread such as malnutrition were also ameliorated, but since the emergence of HIV a new population of immunocompromised individuals was available for TB to infect.
The World Health Organization (WHO) declared TB a «global health emergency» in 1993,[16] and in 2006, the Stop TB Partnership developed a Global Plan to Stop Tuberculosis that aimed to save 14 million lives between its launch and 2015.[94] A number of targets they set were not achieved by 2015, mostly due to the increase in HIV-associated tuberculosis and the emergence of multiple drug-resistant tuberculosis.[16] A tuberculosis classification system developed by the American Thoracic Society is used primarily in public health programs.[95] In 2015, it launched the End TB Strategy to reduce deaths by 95% and incidence by 90% before 2035. The goal of tuberculosis elimination is hampered by the lack of rapid testing, of short and effective treatment courses, and of completely effective vaccines.[96]
The benefits and risks of giving anti-tubercular drugs in those exposed to MDR-TB is unclear.[97] Making HAART therapy available to HIV-positive individuals significantly reduces the risk of progression to an active TB infection by up to 90% and can mitigate the spread through this population.[98]
Treatment

Tuberculosis phototherapy treatment on 3 March 1934, in Kuopio, Finland
Treatment of TB uses antibiotics to kill the bacteria. Effective TB treatment is difficult, due to the unusual structure and chemical composition of the mycobacterial cell wall, which hinders the entry of drugs and makes many antibiotics ineffective.[99]
Active TB is best treated with combinations of several antibiotics to reduce the risk of the bacteria developing antibiotic resistance.[16] The routine use of rifabutin instead of rifampicin in HIV-positive people with tuberculosis is of unclear benefit as of 2007.[100]
Latent TB
Latent TB is treated with either isoniazid or rifampin alone, or a combination of isoniazid with either rifampicin or rifapentine.[101][102][103]
The treatment takes three to nine months depending on the medications used.[45][101][104][103] People with latent infections are treated to prevent them from progressing to active TB disease later in life.[105]
Education or counselling may improve the latent tuberculosis treatment completion rates.[106]
New onset
The recommended treatment of new-onset pulmonary tuberculosis, as of 2010, is six months of a combination of antibiotics containing rifampicin, isoniazid, pyrazinamide, and ethambutol for the first two months, and only rifampicin and isoniazid for the last four months.[16] Where resistance to isoniazid is high, ethambutol may be added for the last four months as an alternative.[16] Treatment with anti-TB drugs for at least 6 months results in higher success rates when compared with treatment less than 6 months, even though the difference is small. Shorter treatment regimen may be recommended for those with compliance issues.[107] There is also no evidence to support shorter anti-tuberculosis treatment regimens when compared to a 6-month treatment regimen.[108] However recently, results from an international, randomized, controlled clinical trial indicate that a four-month daily treatment regimen containing high-dose, or «optimized», rifapentine with moxifloxacin (2PHZM/2PHM) is as safe and effective as the existing standard six-month daily regimen at curing drug-susceptible tuberculosis (TB) disease.[109]
Recurrent disease
If tuberculosis recurs, testing to determine which antibiotics it is sensitive to is important before determining treatment.[16] If multiple drug-resistant TB (MDR-TB) is detected, treatment with at least four effective antibiotics for 18 to 24 months is recommended.[16]
Medication administration
Directly observed therapy, i.e., having a health care provider watch the person take their medications, is recommended by the World Health Organization (WHO) in an effort to reduce the number of people not appropriately taking antibiotics.[110] The evidence to support this practice over people simply taking their medications independently is of poor quality.[111] There is no strong evidence indicating that directly observed therapy improves the number of people who were cured or the number of people who complete their medicine.[111] Moderate quality evidence suggests that there is also no difference if people are observed at home versus at a clinic, or by a family member versus a health care worker.[111] Methods to remind people of the importance of treatment and appointments may result in a small but important improvement.[112] There is also not enough evidence to support intermittent rifampicin-containing therapy given two to three times a week has equal effectiveness as daily dose regimen on improving cure rates and reducing relapsing rates.[113] There is also not enough evidence on effectiveness of giving intermittent twice or thrice weekly short course regimen compared to daily dosing regimen in treating children with tuberculosis.[114]
Medication resistance
Primary resistance occurs when a person becomes infected with a resistant strain of TB. A person with fully susceptible MTB may develop secondary (acquired) resistance during therapy because of inadequate treatment, not taking the prescribed regimen appropriately (lack of compliance), or using low-quality medication.[115] Drug-resistant TB is a serious public health issue in many developing countries, as its treatment is longer and requires more expensive drugs. MDR-TB is defined as resistance to the two most effective first-line TB drugs: rifampicin and isoniazid. Extensively drug-resistant TB is also resistant to three or more of the six classes of second-line drugs.[116] Totally drug-resistant TB is resistant to all currently used drugs.[117] It was first observed in 2003 in Italy,[118] but not widely reported until 2012,[117][119] and has also been found in Iran and India.[120] There is some efficacy for linezolid to treat those with XDR-TB but side effects and discontinuation of medications were common.[121][122] Bedaquiline is tentatively supported for use in multiple drug-resistant TB.[123]
XDR-TB is a term sometimes used to define extensively resistant TB, and constitutes one in ten cases of MDR-TB. Cases of XDR TB have been identified in more than 90% of countries.[120]
For those with known rifampicin or MDR-TB, molecular tests such as the Genotype MTBDRsl Assay (performed on culture isolates or smear positive specimens) may be useful to detect second-line anti-tubercular drug resistance.[124][125]
Prognosis

Progression from TB infection to overt TB disease occurs when the bacilli overcome the immune system defenses and begin to multiply. In primary TB disease (some 1–5% of cases), this occurs soon after the initial infection.[15] However, in the majority of cases, a latent infection occurs with no obvious symptoms.[15] These dormant bacilli produce active tuberculosis in 5–10% of these latent cases, often many years after infection.[18]
The risk of reactivation increases with immunosuppression, such as that caused by infection with HIV. In people coinfected with M. tuberculosis and HIV, the risk of reactivation increases to 10% per year.[15] Studies using DNA fingerprinting of M. tuberculosis strains have shown reinfection contributes more substantially to recurrent TB than previously thought,[127] with estimates that it might account for more than 50% of reactivated cases in areas where TB is common.[128] The chance of death from a case of tuberculosis is about 4% as of 2008, down from 8% in 1995.[16]
In people with smear-positive pulmonary TB (without HIV co-infection), after 5 years without treatment, 50-60% die while 20-25% achieve spontaneous resolution (cure). TB is almost always fatal in those with untreated HIV co-infection and death rates are increased even with antiretroviral treatment of HIV.[129]
Epidemiology
Roughly one-quarter of the world’s population has been infected with M. tuberculosis,[6] with new infections occurring in about 1% of the population each year.[12] However, most infections with M. tuberculosis do not cause disease,[130] and 90–95% of infections remain asymptomatic.[57] In 2012, an estimated 8.6 million chronic cases were active.[131] In 2010, 8.8 million new cases of tuberculosis were diagnosed, and 1.20–1.45 million deaths occurred (most of these occurring in developing countries).[48][132] Of these, about 0.35 million occur in those also infected with HIV.[133] In 2018, tuberculosis was the leading cause of death worldwide from a single infectious agent.[134] The total number of tuberculosis cases has been decreasing since 2005, while new cases have decreased since 2002.[48]
Tuberculosis[clarification needed] incidence is seasonal, with peaks occurring every spring and summer.[135][136][137][138] The reasons for this are unclear, but may be related to vitamin D deficiency during the winter.[138][139] There are also studies linking tuberculosis to different weather conditions like low temperature, low humidity and low rainfall. It has been suggested that tuberculosis incidence rates may be connected to climate change.[140]
At-risk groups
Tuberculosis is closely linked to both overcrowding and malnutrition, making it one of the principal diseases of poverty.[16] Those at high risk thus include: people who inject illicit drugs, inhabitants and employees of locales where vulnerable people gather (e.g., prisons and homeless shelters), medically underprivileged and resource-poor communities, high-risk ethnic minorities, children in close contact with high-risk category patients, and health-care providers serving these patients.[141]
The rate of tuberculosis varies with age. In Africa, it primarily affects adolescents and young adults.[142] However, in countries where incidence rates have declined dramatically (such as the United States), tuberculosis is mainly a disease of the elderly and immunocompromised (risk factors are listed above).[15][143] Worldwide, 22 «high-burden» states or countries together experience 80% of cases as well as 83% of deaths.[120]
In Canada and Australia, tuberculosis is many times more common among the Indigenous peoples, especially in remote areas.[144][145] Factors contributing to this include higher prevalence of predisposing health conditions and behaviours, and overcrowding and poverty. In some Canadian Indigenous groups, genetic susceptibility may play a role.[47]
Socioeconomic status (SES) strongly affects TB risk. People of low SES are both more likely to contract TB and to be more severely affected by the disease. Those with low SES are more likely to be affected by risk factors for developing TB (e.g., malnutrition, indoor air pollution, HIV co-infection, etc.), and are additionally more likely to be exposed to crowded and poorly ventilated spaces. Inadequate healthcare also means that people with active disease who facilitate spread are not diagnosed and treated promptly; sick people thus remain in the infectious state and (continue to) spread the infection.[47]
Geographical epidemiology
The distribution of tuberculosis is not uniform across the globe; about 80% of the population in many African, Caribbean, South Asian, and eastern European countries test positive in tuberculin tests, while only 5–10% of the U.S. population test positive.[15] Hopes of totally controlling the disease have been dramatically dampened because of many factors, including the difficulty of developing an effective vaccine, the expensive and time-consuming diagnostic process, the necessity of many months of treatment, the increase in HIV-associated tuberculosis, and the emergence of drug-resistant cases in the 1980s.[16]
In developed countries, tuberculosis is less common and is found mainly in urban areas. In Europe, deaths from TB fell from 500 out of 100,000 in 1850 to 50 out of 100,000 by 1950. Improvements in public health were reducing tuberculosis even before the arrival of antibiotics, although the disease remained a significant threat to public health, such that when the Medical Research Council was formed in Britain in 1913 its initial focus was tuberculosis research.[146]
In 2010, rates per 100,000 people in different areas of the world were: globally 178, Africa 332, the Americas 36, Eastern Mediterranean 173, Europe 63, Southeast Asia 278, and Western Pacific 139.[133]
Russia
Russia has achieved particularly dramatic progress with a decline in its TB mortality rate—from 61.9 per 100,000 in 1965 to 2.7 per 100,000 in 1993;[147][148] however, mortality rate increased to 24 per 100,000 in 2005 and then recoiled to 11 per 100,000 by 2015.[149]
China
China has achieved particularly dramatic progress, with about an 80% reduction in its TB mortality rate between 1990 and 2010.[133] The number of new cases has declined by 17% between 2004 and 2014.[120]
Africa
In 2007, the country with the highest estimated incidence rate of TB was Eswatini, with 1,200 cases per 100,000 people. In 2017, the country with the highest estimated incidence rate as a % of the population was Lesotho, with 665 cases per 100,000 people.[150]
India
As of 2017, India had the largest total incidence, with an estimated 2,740,000 cases.[150] According to the World Health Organization (WHO), in 2000–2015, India’s estimated mortality rate dropped from 55 to 36 per 100,000 population per year with estimated 480 thousand people died of TB in 2015.[151][152] In India a major proportion of tuberculosis patients are being treated by private partners and private hospitals. Evidence indicates that the tuberculosis national survey does not represent the number of cases that are diagnosed and recorded by private clinics and hospitals in India.[153]
North America
In the United States, Native Americans have a fivefold greater mortality from TB,[154] and racial and ethnic minorities accounted for 84% of all reported TB cases.[155]
In the United States, the overall tuberculosis case rate was 3 per 100,000 persons in 2017.[150] In Canada, tuberculosis is still endemic in some rural areas.[156]
Western Europe
In 2017, in the United Kingdom, the national average was 9 per 100,000 and the highest incidence rates in Western Europe were 20 per 100,000 in Portugal.
-

Number of new cases of tuberculosis per 100,000 people in 2016[157]
-

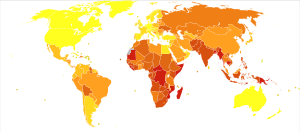
Tuberculosis deaths per million persons in 2012
-
Tuberculosis deaths by region, 1990 to 2017[158]


History

Tuberculosis has existed since antiquity.[16] The oldest unambiguously detected M. tuberculosis gives evidence of the disease in the remains of bison in Wyoming dated to around 17,000 years ago.[159] However, whether tuberculosis originated in bovines, then transferred to humans, or whether both bovine and human tuberculosis diverged from a common ancestor, remains unclear.[160] A comparison of the genes of M. tuberculosis complex (MTBC) in humans to MTBC in animals suggests humans did not acquire MTBC from animals during animal domestication, as researchers previously believed. Both strains of the tuberculosis bacteria share a common ancestor, which could have infected humans even before the Neolithic Revolution.[161] Skeletal remains show some prehistoric humans (4000 BC) had TB, and researchers have found tubercular decay in the spines of Egyptian mummies dating from 3000 to 2400 BC.[162] Genetic studies suggest the presence of TB in the Americas from about AD 100.[163]
Before the Industrial Revolution, folklore often associated tuberculosis with vampires. When one member of a family died from the disease, the other infected members would lose their health slowly. People believed this was caused by the original person with TB draining the life from the other family members.[164]
Although Richard Morton established the pulmonary form associated with tubercles as a pathology in 1689,[165][166] due to the variety of its symptoms, TB was not identified as a single disease until the 1820s. Benjamin Marten conjectured in 1720 that consumptions were caused by microbes which were spread by people living close to each other.[167] In 1819, René Laennec claimed that tubercles were the cause of pulmonary tuberculosis.[168] J. L. Schönlein first published the name «tuberculosis» (German: Tuberkulose) in 1832.[169][170] Between 1838 and 1845, John Croghan, the owner of Mammoth Cave in Kentucky from 1839 onwards, brought a number of people with tuberculosis into the cave in the hope of curing the disease with the constant temperature and purity of the cave air; each died within a year.[171] Hermann Brehmer opened the first TB sanatorium in 1859 in Görbersdorf (now Sokołowsko) in Silesia.[172] In 1865, Jean Antoine Villemin demonstrated that tuberculosis could be transmitted, via inoculation, from humans to animals and among animals.[173] (Villemin’s findings were confirmed in 1867 and 1868 by John Burdon-Sanderson.[174])

Robert Koch discovered the tuberculosis bacillus.
Robert Koch identified and described the bacillus causing tuberculosis, M. tuberculosis, on 24 March 1882.[175][176] In 1905, he was awarded the Nobel Prize in Physiology or Medicine for this discovery.[177] Koch did not believe the cattle and human tuberculosis diseases were similar, which delayed the recognition of infected milk as a source of infection. During the first half of the 1900s, the risk of transmission from this source was dramatically reduced after the application of the pasteurization process. Koch announced a glycerine extract of the tubercle bacilli as a «remedy» for tuberculosis in 1890, calling it «tuberculin». Although it was not effective, it was later successfully adapted as a screening test for the presence of pre-symptomatic tuberculosis.[178] World Tuberculosis Day is marked on 24 March each year, the anniversary of Koch’s original scientific announcement.
Albert Calmette and Camille Guérin achieved the first genuine success in immunization against tuberculosis in 1906, using attenuated bovine-strain tuberculosis. It was called bacille Calmette–Guérin (BCG). The BCG vaccine was first used on humans in 1921 in France,[179] but achieved widespread acceptance in the US, Great Britain, and Germany only after World War II.[180]
Tuberculosis caused widespread public concern in the 19th and early 20th centuries as the disease became common among the urban poor. In 1815, one in four deaths in England was due to «consumption». By 1918, TB still caused one in six deaths in France.[citation needed] After TB was determined to be contagious, in the 1880s, it was put on a notifiable-disease list in Britain; campaigns started to stop people from spitting in public places, and the infected poor were «encouraged» to enter sanatoria that resembled prisons (the sanatoria for the middle and upper classes offered excellent care and constant medical attention).[172] Whatever the benefits of the «fresh air» and labor in the sanatoria, even under the best conditions, 50% of those who entered died within five years (c. 1916).[172] When the Medical Research Council formed in Britain in 1913, it initially focused on tuberculosis research.[181]
In Europe, rates of tuberculosis began to rise in the early 1600s to a peak level in the 1800s, when it caused nearly 25% of all deaths.[182] In the 18th and 19th century, tuberculosis had become epidemic in Europe, showing a seasonal pattern.[183][184] By the 1950s mortality in Europe had decreased about 90%.[185] Improvements in sanitation, vaccination, and other public-health measures began significantly reducing rates of tuberculosis even before the arrival of streptomycin and other antibiotics, although the disease remained a significant threat.[185] In 1946, the development of the antibiotic streptomycin made effective treatment and cure of TB a reality. Prior to the introduction of this medication, the only treatment was surgical intervention, including the «pneumothorax technique», which involved collapsing an infected lung to «rest» it and to allow tuberculous lesions to heal.[186]
Because of the emergence of multidrug-resistant tuberculosis (MDR-TB), surgery has been re-introduced for certain cases of TB infections. It involves the removal of infected chest cavities («bullae») in the lungs to reduce the number of bacteria and to increase exposure of the remaining bacteria to antibiotics in the bloodstream.[187] Hopes of eliminating TB ended with the rise of drug-resistant strains in the 1980s. The subsequent resurgence of tuberculosis resulted in the declaration of a global health emergency by the World Health Organization (WHO) in 1993.[188]
Society and culture
Names
Tuberculosis has been known by many names from the technical to the familiar.[189] Phthisis (Φθισις) is a Greek word for consumption, an old term for pulmonary tuberculosis;[8] around 460 BCE, Hippocrates described phthisis as a disease of dry seasons.[190] The abbreviation TB is short for tubercle bacillus. Consumption was the most common nineteenth century English word for the disease, and was also in use well into the twentieth century. The Latin root con meaning ‘completely’ is linked to sumere meaning ‘to take up from under’.[191] In The Life and Death of Mr Badman by John Bunyan, the author calls consumption «the captain of all these men of death.»[192] «Great white plague» has also been used.[189]
Art and literature

Painting The Sick Child by Edvard Munch, 1885–1886, depicts the illness of his sister Sophie, who died of tuberculosis when Edvard was 14; his mother too died of the disease.
Tuberculosis was for centuries associated with poetic and artistic qualities among those infected, and was also known as «the romantic disease».[189][193] Major artistic figures such as the poets John Keats, Percy Bysshe Shelley, and Edgar Allan Poe, the composer Frédéric Chopin,[194] the playwright Anton Chekhov, the novelists Franz Kafka, Katherine Mansfield,[195] Charlotte Brontë, Fyodor Dostoevsky, Thomas Mann, W. Somerset Maugham,[196] George Orwell,[197] and Robert Louis Stevenson, and the artists Alice Neel,[198] Jean-Antoine Watteau, Elizabeth Siddal, Marie Bashkirtseff, Edvard Munch, Aubrey Beardsley and Amedeo Modigliani either had the disease or were surrounded by people who did. A widespread belief was that tuberculosis assisted artistic talent. Physical mechanisms proposed for this effect included the slight fever and toxaemia that it caused, allegedly helping them to see life more clearly and to act decisively.[199][200][201]
Tuberculosis formed an often-reused theme in literature, as in Thomas Mann’s The Magic Mountain, set in a sanatorium;[202] in music, as in Van Morrison’s song «T.B. Sheets»;[203] in opera, as in Puccini’s La bohème and Verdi’s La Traviata;[201] in art, as in Monet’s painting of his first wife Camille on her deathbed;[204] and in film, such as the 1945 The Bells of St. Mary’s starring Ingrid Bergman as a nun with tuberculosis.[205]
Public health efforts
In 2014, the WHO adopted the «End TB» strategy which aims to reduce TB incidence by 80% and TB deaths by 90% by 2030.[206] The strategy contains a milestone to reduce TB incidence by 20% and TB deaths by 35% by 2020.[207] However, by 2020 only a 9% reduction in incidence per population was achieved globally, with the European region achieving 19% and the African region achieving 16% reductions.[207] Similarly, the number of deaths only fell by 14%, missing the 2020 milestone of a 35% reduction, with some regions making better progress (31% reduction in Europe and 19% in Africa).[207] Correspondingly, also treatment, prevention and funding milestones were missed in 2020, for example only 6.3 million people were started on TB prevention short of the target of 30 million.[207]
The World Health Organization (WHO), the Bill and Melinda Gates Foundation, and the U.S. government are subsidizing a fast-acting diagnostic tuberculosis test for use in low- and middle-income countries as of 2012.[208][209][210] In addition to being fast-acting, the test can determine if there is resistance to the antibiotic rifampicin which may indicate multi-drug resistant tuberculosis and is accurate in those who are also infected with HIV.[208][211] Many resource-poor places as of 2011 have access to only sputum microscopy.[212]
India had the highest total number of TB cases worldwide in 2010, in part due to poor disease management within the private and public health care sector.[213] Programs such as the Revised National Tuberculosis Control Program are working to reduce TB levels among people receiving public health care.[214][215]
A 2014 EIU-healthcare report finds there is a need to address apathy and urges for increased funding. The report cites among others Lucica Ditui «[TB] is like an orphan. It has been neglected even in countries with a high burden and often forgotten by donors and those investing in health interventions.»[120]
Slow progress has led to frustration, expressed by the executive director of the Global Fund to Fight AIDS, Tuberculosis and Malaria – Mark Dybul: «we have the tools to end TB as a pandemic and public health threat on the planet, but we are not doing it.»[120] Several international organizations are pushing for more transparency in treatment, and more countries are implementing mandatory reporting of cases to the government as of 2014, although adherence is often variable. Commercial treatment providers may at times overprescribe second-line drugs as well as supplementary treatment, promoting demands for further regulations.[120] The government of Brazil provides universal TB care, which reduces this problem.[120] Conversely, falling rates of TB infection may not relate to the number of programs directed at reducing infection rates but may be tied to an increased level of education, income, and health of the population.[120] Costs of the disease, as calculated by the World Bank in 2009 may exceed US$150 billion per year in «high burden» countries.[120] Lack of progress eradicating the disease may also be due to lack of patient follow-up – as among the 250 million rural migrants in China.[120]
There is insufficient data to show that active contact tracing helps to improve case detection rates for tuberculosis.[216] Interventions such as house-to-house visits, educational leaflets, mass media strategies, educational sessions may increase tuberculosis detection rates in short-term.[217] There is no study that compares new methods of contact tracing such as social network analysis with existing contact tracing methods.[218]
Stigma
Slow progress in preventing the disease may in part be due to stigma associated with TB.[120] Stigma may be due to the fear of transmission from affected individuals. This stigma may additionally arise due to links between TB and poverty, and in Africa, AIDS.[120] Such stigmatization may be both real and perceived; for example, in Ghana, individuals with TB are banned from attending public gatherings.[219]
Stigma towards TB may result in delays in seeking treatment,[120] lower treatment compliance, and family members keeping cause of death secret[219] – allowing the disease to spread further.[120] In contrast, in Russia stigma was associated with increased treatment compliance.[219] TB stigma also affects socially marginalized individuals to a greater degree and varies between regions.[219]
One way to decrease stigma may be through the promotion of «TB clubs», where those infected may share experiences and offer support, or through counseling.[219] Some studies have shown TB education programs to be effective in decreasing stigma, and may thus be effective in increasing treatment adherence.[219] Despite this, studies on the relationship between reduced stigma and mortality are lacking as of 2010, and similar efforts to decrease stigma surrounding AIDS have been minimally effective.[219] Some have claimed the stigma to be worse than the disease, and healthcare providers may unintentionally reinforce stigma, as those with TB are often perceived as difficult or otherwise undesirable.[120] A greater understanding of the social and cultural dimensions of tuberculosis may also help with stigma reduction.[220]
Research
The BCG vaccine has limitations, and research to develop new TB vaccines is ongoing.[221] A number of potential candidates are currently in phase I and II clinical trials.[221][222] Two main approaches are used to attempt to improve the efficacy of available vaccines. One approach involves adding a subunit vaccine to BCG, while the other strategy is attempting to create new and better live vaccines.[221] MVA85A, an example of a subunit vaccine, is in trials in South Africa as of 2006, is based on a genetically modified vaccinia virus.[223] Vaccines are hoped to play a significant role in treatment of both latent and active disease.[224]
To encourage further discovery, researchers and policymakers are promoting new economic models of vaccine development as of 2006, including prizes, tax incentives, and advance market commitments.[225][226] A number of groups, including the Stop TB Partnership,[227] the South African Tuberculosis Vaccine Initiative, and the Aeras Global TB Vaccine Foundation, are involved with research.[228] Among these, the Aeras Global TB Vaccine Foundation received a gift of more than $280 million (US) from the Bill and Melinda Gates Foundation to develop and license an improved vaccine against tuberculosis for use in high burden countries.[229][230]
A number of medications are being studied as of 2012 for multidrug-resistant tuberculosis, including bedaquiline and delamanid.[231] Bedaquiline received U.S. Food and Drug Administration (FDA) approval in late 2012.[232] The safety and effectiveness of these new agents are uncertain as of 2012, because they are based on the results of relatively small studies.[231][233] However, existing data suggest that patients taking bedaquiline in addition to standard TB therapy are five times more likely to die than those without the new drug,[234] which has resulted in medical journal articles raising health policy questions about why the FDA approved the drug and whether financial ties to the company making bedaquiline influenced physicians’ support for its use.[233][235]
Steroids add-on therapy has not shown any benefits for active pulmonary tuberculosis infection.[236]
Other animals
Mycobacteria infect many different animals, including birds,[237] fish, rodents,[238] and reptiles.[239] The subspecies Mycobacterium tuberculosis, though, is rarely present in wild animals.[240] An effort to eradicate bovine tuberculosis caused by Mycobacterium bovis from the cattle and deer herds of New Zealand has been relatively successful.[241] Efforts in Great Britain have been less successful.[242][243]
As of 2015, tuberculosis appears to be widespread among captive elephants in the US. It is believed that the animals originally acquired the disease from humans, a process called reverse zoonosis. Because the disease can spread through the air to infect both humans and other animals, it is a public health concern affecting circuses and zoos.[244][245]
References
- ^ a b c d e f g h i j k l m n o p «Tuberculosis (TB)». who.int. Archived from the original on 30 July 2020. Retrieved 8 May 2020.
- ^ Ferri FF (2010). Ferri’s differential diagnosis : a practical guide to the differential diagnosis of symptoms, signs, and clinical disorders (2nd ed.). Philadelphia, PA: Elsevier/Mosby. p. Chapter T. ISBN 978-0-323-07699-9.
- ^ a b Hawn TR, Day TA, Scriba TJ, Hatherill M, Hanekom WA, Evans TG, et al. (December 2014). «Tuberculosis vaccines and prevention of infection». Microbiology and Molecular Biology Reviews. 78 (4): 650–71. doi:10.1128/MMBR.00021-14. PMC 4248657. PMID 25428938.
- ^ a b c Implementing the WHO Stop TB Strategy: a handbook for national TB control programmes. Geneva: World Health Organization (WHO). 2008. p. 179. ISBN 978-92-4-154667-6. Archived from the original on 2 June 2021. Retrieved 17 September 2017.
- ^ a b Harris RE (2013). «Epidemiology of Tuberculosis». Epidemiology of chronic disease: global perspectives. Burlington, MA: Jones & Bartlett Learning. p. 682. ISBN 978-0-7637-8047-0.
- ^ a b c «Tuberculosis (TB)». World Health Organization (WHO). 16 February 2018. Archived from the original on 30 December 2013. Retrieved 15 September 2018.
- ^ «Tuberculosis deaths rise for the first time in more than a decade due to the COVID-19 pandemic». www.who.int. Archived from the original on 16 October 2021. Retrieved 16 October 2021.
- ^ a b The Chambers Dictionary. New Delhi: Allied Chambers India Ltd. 1998. p. 352. ISBN 978-81-86062-25-8. Archived from the original on 6 September 2015.
- ^ a b c d e f g h i Adkinson NF, Bennett JE, Douglas RG, Mandell GL (2010). Mandell, Douglas, and Bennett’s principles and practice of infectious diseases (7th ed.). Philadelphia, PA: Churchill Livingstone/Elsevier. p. Chapter 250. ISBN 978-0-443-06839-3.
- ^ «Basic TB Facts». Centers for Disease Control and Prevention (CDC). 13 March 2012. Archived from the original on 6 February 2016. Retrieved 11 February 2016.
- ^ a b Konstantinos A (2010). «Testing for tuberculosis». Australian Prescriber. 33 (1): 12–18. doi:10.18773/austprescr.2010.005.
- ^ a b «Tuberculosis». World Health Organization (WHO). 2002. Archived from the original on 17 June 2013.
- ^ a b «Tuberculosis (TB)». WHO. Archived from the original on 30 July 2020. Retrieved 16 October 2021.
- ^ «Global tuberculosis report». World Health Organization (WHO). Archived from the original on 30 December 2013. Retrieved 9 November 2017.
- ^ a b c d e f g h i j k l m n o Kumar V, Robbins SL (2007). Robbins Basic Pathology (8th ed.). Philadelphia: Elsevier. ISBN 978-1-4160-2973-1. OCLC 69672074.
- ^ a b c d e f g h i j k l m n o p q r s t u v Lawn SD, Zumla AI (July 2011). «Tuberculosis». Lancet. 378 (9785): 57–72. doi:10.1016/S0140-6736(10)62173-3. PMID 21420161. S2CID 208791546. Archived from the original on 27 August 2021. Retrieved 31 January 2020.
- ^ Schiffman G (15 January 2009). «Tuberculosis Symptoms». eMedicine Health. Archived from the original on 16 May 2009.
- ^ a b c d Gibson PG, Abramson M, Wood-Baker R, Volmink J, Hensley M, Costabel U, eds. (2005). Evidence-Based Respiratory Medicine (1st ed.). BMJ Books. p. 321. ISBN 978-0-7279-1605-1. Archived from the original on 8 December 2015.
- ^ Behera D (2010). Textbook of Pulmonary Medicine (2nd ed.). New Delhi: Jaypee Brothers Medical Publishers. p. 457. ISBN 978-81-8448-749-7. Archived from the original on 6 September 2015.
- ^ Halezeroğlu S, Okur E (March 2014). «Thoracic surgery for haemoptysis in the context of tuberculosis: what is the best management approach?». Journal of Thoracic Disease. 6 (3): 182–85. doi:10.3978/j.issn.2072-1439.2013.12.25. PMC 3949181. PMID 24624281.
- ^ Jindal SK, ed. (2011). Textbook of Pulmonary and Critical Care Medicine. New Delhi: Jaypee Brothers Medical Publishers. p. 549. ISBN 978-93-5025-073-0. Archived from the original on 7 September 2015.
- ^ a b Habermann TM, Ghosh A (2008). Mayo Clinic internal medicine: concise textbook. Rochester, MN: Mayo Clinic Scientific Press. p. 789. ISBN 978-1-4200-6749-1. Archived from the original on 6 September 2015.
- ^ Southwick F (2007). «Chapter 4: Pulmonary Infections». Infectious Diseases: A Clinical Short Course, 2nd ed. McGraw-Hill Medical Publishing Division. pp. 104, 313–14. ISBN 978-0-07-147722-2.
- ^ Jindal SK (2011). Textbook of Pulmonary and Critical Care Medicine. New Delhi: Jaypee Brothers Medical Publishers. p. 525. ISBN 978-93-5025-073-0. Archived from the original on 6 September 2015.
- ^ Niederweis M, Danilchanka O, Huff J, Hoffmann C, Engelhardt H (March 2010). «Mycobacterial outer membranes: in search of proteins». Trends in Microbiology. 18 (3): 109–16. doi:10.1016/j.tim.2009.12.005. PMC 2931330. PMID 20060722.
- ^ a b Madison BM (May 2001). «Application of stains in clinical microbiology». Biotechnic & Histochemistry. 76 (3): 119–25. doi:10.1080/714028138. PMID 11475314.
- ^ Parish T, Stoker NG (December 1999). «Mycobacteria: bugs and bugbears (two steps forward and one step back)». Molecular Biotechnology. 13 (3): 191–200. doi:10.1385/MB:13:3:191. PMID 10934532. S2CID 28960959.
- ^ Medical Laboratory Science: Theory and Practice. New Delhi: Tata McGraw-Hill. 2000. p. 473. ISBN 978-0-07-463223-9. Archived from the original on 6 September 2015.
- ^ «Acid-Fast Stain Protocols». 21 August 2013. Archived from the original on 1 October 2011. Retrieved 26 March 2016.
- ^ Kommareddi S, Abramowsky CR, Swinehart GL, Hrabak L (November 1984). «Nontuberculous mycobacterial infections: comparison of the fluorescent auramine-O and Ziehl-Neelsen techniques in tissue diagnosis». Human Pathology. 15 (11): 1085–9. doi:10.1016/S0046-8177(84)80253-1. PMID 6208117.
- ^ van Lettow M, Whalen C (2008). Semba RD, Bloem MW (eds.). Nutrition and health in developing countries (2nd ed.). Totowa, N.J.: Humana Press. p. 291. ISBN 978-1-934115-24-4. Archived from the original on 6 September 2015.
- ^ van Soolingen D, Hoogenboezem T, de Haas PE, Hermans PW, Koedam MA, Teppema KS, et al. (October 1997). «A novel pathogenic taxon of the Mycobacterium tuberculosis complex, Canetti: characterization of an exceptional isolate from Africa». International Journal of Systematic Bacteriology. 47 (4): 1236–45. doi:10.1099/00207713-47-4-1236. PMID 9336935.
- ^ Niemann S, Rüsch-Gerdes S, Joloba ML, Whalen CC, Guwatudde D, Ellner JJ, et al. (September 2002). «Mycobacterium africanum subtype II is associated with two distinct genotypes and is a major cause of human tuberculosis in Kampala, Uganda». Journal of Clinical Microbiology. 40 (9): 3398–405. doi:10.1128/JCM.40.9.3398-3405.2002. PMC 130701. PMID 12202584.
- ^ Niobe-Eyangoh SN, Kuaban C, Sorlin P, Cunin P, Thonnon J, Sola C, et al. (June 2003). «Genetic biodiversity of Mycobacterium tuberculosis complex strains from patients with pulmonary tuberculosis in Cameroon». Journal of Clinical Microbiology. 41 (6): 2547–53. doi:10.1128/JCM.41.6.2547-2553.2003. PMC 156567. PMID 12791879.
- ^ Thoen C, Lobue P, de Kantor I (February 2006). «The importance of Mycobacterium bovis as a zoonosis». Veterinary Microbiology. 112 (2–4): 339–45. doi:10.1016/j.vetmic.2005.11.047. PMID 16387455.
- ^ Acton QA (2011). Mycobacterium Infections: New Insights for the Healthcare Professional. ScholarlyEditions. p. 1968. ISBN 978-1-4649-0122-5. Archived from the original on 6 September 2015.
- ^ Pfyffer GE, Auckenthaler R, van Embden JD, van Soolingen D (1998). «Mycobacterium canettii, the smooth variant of M. tuberculosis, isolated from a Swiss patient exposed in Africa». Emerging Infectious Diseases. 4 (4): 631–4. doi:10.3201/eid0404.980414. PMC 2640258. PMID 9866740.
- ^ Panteix G, Gutierrez MC, Boschiroli ML, Rouviere M, Plaidy A, Pressac D, et al. (August 2010). «Pulmonary tuberculosis due to Mycobacterium microti: a study of six recent cases in France». Journal of Medical Microbiology. 59 (Pt 8): 984–989. doi:10.1099/jmm.0.019372-0. PMID 20488936.
- ^ American Thoracic Society (August 1997). «Diagnosis and treatment of disease caused by nontuberculous mycobacteria. This official statement of the American Thoracic Society was approved by the Board of Directors, March 1997. Medical Section of the American Lung Association». American Journal of Respiratory and Critical Care Medicine. 156 (2 Pt 2): S1–25. doi:10.1164/ajrccm.156.2.atsstatement. PMID 9279284.
- ^ Cole EC, Cook CE (August 1998). «Characterization of infectious aerosols in health care facilities: an aid to effective engineering controls and preventive strategies». American Journal of Infection Control. 26 (4): 453–64. doi:10.1016/S0196-6553(98)70046-X. PMC 7132666. PMID 9721404.
- ^ Nicas M, Nazaroff WW, Hubbard A (March 2005). «Toward understanding the risk of secondary airborne infection: emission of respirable pathogens». Journal of Occupational and Environmental Hygiene. 2 (3): 143–54. doi:10.1080/15459620590918466. PMC 7196697. PMID 15764538.
- ^ a b Ahmed N, Hasnain SE (September 2011). «Molecular epidemiology of tuberculosis in India: moving forward with a systems biology approach». Tuberculosis. 91 (5): 407–13. doi:10.1016/j.tube.2011.03.006. PMID 21514230.
- ^ a b «Tuberculosis Fact sheet N°104». World Health Organization (WHO). November 2010. Archived from the original on 4 October 2006. Retrieved 26 July 2011.
- ^ a b «Core Curriculum on Tuberculosis: What the Clinician Should Know» (PDF) (5th ed.). Centers for Disease Control and Prevention (CDC), Division of Tuberculosis Elimination. 2011. p. 24. Archived (PDF) from the original on 19 May 2012.
- ^ «Causes of Tuberculosis». Mayo Clinic. 21 December 2006. Archived from the original on 18 October 2007. Retrieved 19 October 2007.
- ^ a b c d e Narasimhan P, Wood J, Macintyre CR, Mathai D (2013). «Risk factors for tuberculosis». Pulmonary Medicine. 2013: 828939. doi:10.1155/2013/828939. PMC 3583136. PMID 23476764.
- ^ a b c «The sixteenth global report on tuberculosis» (PDF). World Health Organization (WHO). 2011. Archived from the original (PDF) on 6 September 2012.
- ^ «Global tuberculosis control–surveillance, planning, financing WHO Report 2006». World Health Organization (WHO). Archived from the original on 12 December 2006. Retrieved 13 October 2006.
- ^ Chaisson RE, Martinson NA (March 2008). «Tuberculosis in Africa – combating an HIV-driven crisis». The New England Journal of Medicine. 358 (11): 1089–92. doi:10.1056/NEJMp0800809. PMID 18337598.
- ^ Restrepo BI (August 2007). «Convergence of the tuberculosis and diabetes epidemics: renewal of old acquaintances». Clinical Infectious Diseases. 45 (4): 436–38. doi:10.1086/519939. PMC 2900315. PMID 17638190.
- ^ «Targeted tuberculin testing and treatment of latent tuberculosis infection. American Thoracic Society». MMWR. Recommendations and Reports. 49 (RR-6): 1–51. June 2000. PMID 10881762. Archived from the original on 17 December 2004.
- ^ van Zyl Smit RN, Pai M, Yew WW, Leung CC, Zumla A, Bateman ED, et al. (January 2010). «Global lung health: the colliding epidemics of tuberculosis, tobacco smoking, HIV and COPD». The European Respiratory Journal. 35 (1): 27–33. doi:10.1183/09031936.00072909. PMC 5454527. PMID 20044459.
These analyses indicate that smokers are almost twice as likely to be infected with TB and to progress to active disease (RR of about 1.5 for latent TB infection (LTBI) and RR of ∼2.0 for TB disease). Smokers are also twice as likely to die from TB (RR of about 2.0 for TB mortality), but data are difficult to interpret because of heterogeneity in the results across studies.
- ^ «TB Risk Factors | Basic TB Facts | TB | CDC». cdc.gov. 26 May 2020. Archived from the original on 30 August 2020. Retrieved 25 August 2020.
- ^ Möller M, Hoal EG (March 2010). «Current findings, challenges and novel approaches in human genetic susceptibility to tuberculosis». Tuberculosis. 90 (2): 71–83. doi:10.1016/j.tube.2010.02.002. PMID 20206579.
- ^ Good JM, Cooper S, Doane AS (1835). The Study of Medicine. Harper. p. 32. Archived from the original on 10 August 2016.
- ^ a b Skolnik R (2011). Global health 101 (2nd ed.). Burlington, MA: Jones & Bartlett Learning. p. 253. ISBN 978-0-7637-9751-5.
- ^ a b Mainous III AR, Pomeroy C (2009). Management of antimicrobials in infectious diseases: impact of antibiotic resistance (2nd rev. ed.). Totowa, NJ: Humana Press. p. 74. ISBN 978-1-60327-238-4. Archived from the original on 6 September 2015.
- ^ Houben EN, Nguyen L, Pieters J (February 2006). «Interaction of pathogenic mycobacteria with the host immune system». Current Opinion in Microbiology. 9 (1): 76–85. doi:10.1016/j.mib.2005.12.014. PMID 16406837.
- ^ Queval CJ, Brosch R, Simeone R (2017). «Mycobacterium tuberculosis». Frontiers in Microbiology. 8: 2284. doi:10.3389/fmicb.2017.02284. PMC 5703847. PMID 29218036.
- ^ Khan MR (2011). Essence of Paediatrics. Elsevier India. p. 401. ISBN 978-81-312-2804-3. Archived from the original on 6 September 2015.
- ^ Herrmann JL, Lagrange PH (February 2005). «Dendritic cells and Mycobacterium tuberculosis: which is the Trojan horse?». Pathologie-Biologie. 53 (1): 35–40. doi:10.1016/j.patbio.2004.01.004. PMID 15620608.
- ^ Agarwal R, Malhotra P, Awasthi A, Kakkar N, Gupta D (April 2005). «Tuberculous dilated cardiomyopathy: an under-recognized entity?». BMC Infectious Diseases. 5 (1): 29. doi:10.1186/1471-2334-5-29. PMC 1090580. PMID 15857515.
- ^ a b c d Grosset J (March 2003). «Mycobacterium tuberculosis in the extracellular compartment: an underestimated adversary». Antimicrobial Agents and Chemotherapy. 47 (3): 833–36. doi:10.1128/AAC.47.3.833-836.2003. PMC 149338. PMID 12604509.
- ^ Bozzano F, Marras F, De Maria A (2014). «Immunology of tuberculosis». Mediterranean Journal of Hematology and Infectious Diseases. 6 (1): e2014027. doi:10.4084/MJHID.2014.027. PMC 4010607. PMID 24804000.
- ^ Crowley LV (2010). An introduction to human disease: pathology and pathophysiology correlations (8th ed.). Sudbury, MA: Jones and Bartlett. p. 374. ISBN 978-0-7637-6591-0. Archived from the original on 6 September 2015.
- ^ Anthony H (2005). TB/HIV a Clinical Manual (2nd ed.). Geneva: World Health Organization (WHO). p. 75. ISBN 978-92-4-154634-8. Archived from the original on 6 September 2015.
- ^ Jacob JT, Mehta AK, Leonard MK (January 2009). «Acute forms of tuberculosis in adults». The American Journal of Medicine. 122 (1): 12–17. doi:10.1016/j.amjmed.2008.09.018. PMID 19114163.
- ^ a b Bento J, Silva AS, Rodrigues F, Duarte R (2011). «[Diagnostic tools in tuberculosis]». Acta Médica Portuguesa. 24 (1): 145–54. doi:10.20344/amp.333. PMID 21672452. S2CID 76156550.
- ^ a b c d Escalante P (June 2009). «In the clinic. Tuberculosis». Annals of Internal Medicine. 150 (11): ITC61-614, quiz ITV616. doi:10.7326/0003-4819-150-11-200906020-01006. PMID 19487708. S2CID 639982. Archived from the original on 27 August 2021. Retrieved 31 January 2020.
- ^ Metcalfe JZ, Everett CK, Steingart KR, Cattamanchi A, Huang L, Hopewell PC, Pai M (November 2011). «Interferon-γ release assays for active pulmonary tuberculosis diagnosis in adults in low- and middle-income countries: systematic review and meta-analysis». The Journal of Infectious Diseases. 204 Suppl 4 (suppl_4): S1120-9. doi:10.1093/infdis/jir410. PMC 3192542. PMID 21996694.
- ^ a b Sester M, Sotgiu G, Lange C, Giehl C, Girardi E, Migliori GB, et al. (January 2011). «Interferon-γ release assays for the diagnosis of active tuberculosis: a systematic review and meta-analysis». The European Respiratory Journal. 37 (1): 100–11. doi:10.1183/09031936.00114810. PMID 20847080.
- ^ Chen J, Zhang R, Wang J, Liu L, Zheng Y, Shen Y, et al. (2011). Vermund SH (ed.). «Interferon-gamma release assays for the diagnosis of active tuberculosis in HIV-infected patients: a systematic review and meta-analysis». PLOS ONE. 6 (11): e26827. Bibcode:2011PLoSO…626827C. doi:10.1371/journal.pone.0026827. PMC 3206065. PMID 22069472.
- ^ Special Programme for Research & Training in Tropical Diseases (2006). Diagnostics for tuberculosis: global demand and market potential. Geneva: World Health Organization (WHO). p. 36. ISBN 978-92-4-156330-7. Archived from the original on 6 September 2015.
- ^ a b National Institute for Health and Clinical Excellence. Clinical guideline 117: Tuberculosis. London, 2011.
- ^ Steingart KR, Flores LL, Dendukuri N, Schiller I, Laal S, Ramsay A, et al. (August 2011). Evans C (ed.). «Commercial serological tests for the diagnosis of active pulmonary and extrapulmonary tuberculosis: an updated systematic review and meta-analysis». PLOS Medicine. 8 (8): e1001062. doi:10.1371/journal.pmed.1001062. PMC 3153457. PMID 21857806.
- ^ Rothel JS, Andersen P (December 2005). «Diagnosis of latent Mycobacterium tuberculosis infection: is the demise of the Mantoux test imminent?». Expert Review of Anti-Infective Therapy. 3 (6): 981–93. doi:10.1586/14787210.3.6.981. PMID 16307510. S2CID 25423684.
- ^ Pai M, Zwerling A, Menzies D (August 2008). «Systematic review: T-cell-based assays for the diagnosis of latent tuberculosis infection: an update». Annals of Internal Medicine. 149 (3): 177–84. doi:10.7326/0003-4819-149-3-200808050-00241. PMC 2951987. PMID 18593687.
- ^ Jindal SK, ed. (2011). Textbook of Pulmonary and Critical Care Medicine. New Delhi: Jaypee Brothers Medical Publishers. p. 544. ISBN 978-93-5025-073-0. Archived from the original on 6 September 2015.
- ^ Amicosante M, Ciccozzi M, Markova R (April 2010). «Rational use of immunodiagnostic tools for tuberculosis infection: guidelines and cost effectiveness studies». The New Microbiologica. 33 (2): 93–107. PMID 20518271.
- ^ Bibbins-Domingo K, Grossman DC, Curry SJ, Bauman L, Davidson KW, Epling JW, et al. (September 2016). «Screening for Latent Tuberculosis Infection in Adults: US Preventive Services Task Force Recommendation Statement». JAMA. 316 (9): 962–9. doi:10.1001/jama.2016.11046. PMID 27599331.
- ^ Gill J, Prasad V (November 2019). «Testing Healthcare Workers for Latent Tuberculosis: Is It Evidence Based, Bio-Plausible, Both, Or Neither?». The American Journal of Medicine. 132 (11): 1260–1261. doi:10.1016/j.amjmed.2019.03.017. PMID 30946831.
- ^ Sosa LE, Njie GJ, Lobato MN, Bamrah Morris S, Buchta W, Casey ML, et al. (May 2019). «Tuberculosis Screening, Testing, and Treatment of U.S. Health Care Personnel: Recommendations from the National Tuberculosis Controllers Association and CDC, 2019». MMWR. Morbidity and Mortality Weekly Report. 68 (19): 439–443. doi:10.15585/mmwr.mm6819a3. PMC 6522077. PMID 31099768.
- ^ Coker, Richard; Thomas, Marianna; Lock, Karen; Martin, Robyn (2007). «Detention and the Evolving Threat of Tuberculosis: Evidence, Ethics, and Law». Journal of Law, Medicine & Ethics. 35 (4): 609–615. doi:10.1111/j.1748-720X.2007.00184.x. ISSN 1073-1105. PMID 18076512. S2CID 19924571.
- ^ McShane H (October 2011). «Tuberculosis vaccines: beyond bacille Calmette-Guerin». Philosophical Transactions of the Royal Society of London. Series B, Biological Sciences. 366 (1579): 2782–89. doi:10.1098/rstb.2011.0097. PMC 3146779. PMID 21893541.
- ^ «Vaccines | Basic TB Facts | TB | CDC». cdc.gov. CDC. 16 June 2021. Retrieved 30 December 2021.
- ^ Roy A, Eisenhut M, Harris RJ, Rodrigues LC, Sridhar S, Habermann S, et al. (August 2014). «Effect of BCG vaccination against Mycobacterium tuberculosis infection in children: systematic review and meta-analysis». BMJ. 349: g4643. doi:10.1136/bmj.g4643. PMC 4122754. PMID 25097193.
- ^ «Vaccine and Immunizations: TB Vaccine (BCG)». Centers for Disease Control and Prevention. 2011. Archived from the original on 17 November 2011. Retrieved 26 July 2011.
- ^ «BCG Vaccine Usage in Canada – Current and Historical». Public Health Agency of Canada. September 2010. Archived from the original on 30 March 2012. Retrieved 30 December 2011.
- ^ a b Teo SS, Shingadia DV (June 2006). «Does BCG have a role in tuberculosis control and prevention in the United Kingdom?». Archives of Disease in Childhood. 91 (6): 529–31. doi:10.1136/adc.2005.085043. PMC 2082765. PMID 16714729.
- ^ Kashangura R, Jullien S, Garner P, Johnson S, et al. (Cochrane Infectious Diseases Group) (April 2019). «MVA85A vaccine to enhance BCG for preventing tuberculosis». The Cochrane Database of Systematic Reviews. 2019 (4): CD012915. doi:10.1002/14651858.CD012915.pub2. PMC 6488980. PMID 31038197.
- ^ Clark M, Riben P, Nowgesic E (October 2002). «The association of housing density, isolation and tuberculosis in Canadian First Nations communities». International Journal of Epidemiology. 31 (5): 940–945. doi:10.1093/ije/31.5.940. PMID 12435764.
- ^ Barberis I, Bragazzi NL, Galluzzo L, Martini M (March 2017). «The history of tuberculosis: from the first historical records to the isolation of Koch’s bacillus». Journal of Preventive Medicine and Hygiene. 58 (1): E9–E12. PMC 5432783. PMID 28515626.
- ^ «The Global Plan to Stop TB». World Health Organization (WHO). 2011. Archived from the original on 12 June 2011. Retrieved 13 June 2011.
- ^ Warrell DA, Cox TM, Firth JD, Benz EJ (2005). Sections 1–10 (4. ed., paperback ed.). Oxford [u.a.]: Oxford Univ. Press. p. 560. ISBN 978-0-19-857014-1. Archived from the original on 6 September 2015.
- ^ Uplekar M, Weil D, Lonnroth K, Jaramillo E, Lienhardt C, Dias HM, et al. (May 2015). «WHO’s new end TB strategy». Lancet. 385 (9979): 1799–1801. doi:10.1016/S0140-6736(15)60570-0. PMID 25814376. S2CID 39379915.
- ^ Fraser A, Paul M, Attamna A, Leibovici L, et al. (Cochrane Infectious Diseases Group) (April 2006). «Drugs for preventing tuberculosis in people at risk of multiple-drug-resistant pulmonary tuberculosis». The Cochrane Database of Systematic Reviews. 2006 (2): CD005435. doi:10.1002/14651858.CD005435.pub2. PMC 6532726. PMID 16625639.
- ^ Piggott DA, Karakousis PC (27 December 2010). «Timing of antiretroviral therapy for HIV in the setting of TB treatment». Clinical & Developmental Immunology. 2011: 103917. doi:10.1155/2011/103917. PMC 3017895. PMID 21234380.
- ^ Brennan PJ, Nikaido H (1995). «The envelope of mycobacteria». Annual Review of Biochemistry. 64: 29–63. doi:10.1146/annurev.bi.64.070195.000333. PMID 7574484.
- ^ Davies G, Cerri S, Richeldi L (October 2007). «Rifabutin for treating pulmonary tuberculosis». The Cochrane Database of Systematic Reviews. 2007 (4): CD005159. doi:10.1002/14651858.CD005159.pub2. PMC 6532710. PMID 17943842.
- ^ a b Latent tuberculosis infection. World Health Organization (WHO). 2018. p. 23. ISBN 978-92-4-155023-9. Archived from the original on 2 June 2021. Retrieved 25 July 2018.
- ^ Borisov AS, Bamrah Morris S, Njie GJ, Winston CA, Burton D, Goldberg S, et al. (June 2018). «Update of Recommendations for Use of Once-Weekly Isoniazid-Rifapentine Regimen to Treat Latent Mycobacterium tuberculosis Infection». MMWR. Morbidity and Mortality Weekly Report. 67 (25): 723–726. doi:10.15585/mmwr.mm6725a5. PMC 6023184. PMID 29953429.
- ^ a b Sterling TR, Njie G, Zenner D, Cohn DL, Reves R, Ahmed A, et al. (February 2020). «Guidelines for the Treatment of Latent Tuberculosis Infection: Recommendations from the National Tuberculosis Controllers Association and CDC, 2020». MMWR. Recommendations and Reports. 69 (1): 1–11. doi:10.15585/mmwr.rr6901a1. PMC 7041302. PMID 32053584.
- ^ Njie GJ, Morris SB, Woodruff RY, Moro RN, Vernon AA, Borisov AS (August 2018). «Isoniazid-Rifapentine for Latent Tuberculosis Infection: A Systematic Review and Meta-analysis». American Journal of Preventive Medicine. 55 (2): 244–252. doi:10.1016/j.amepre.2018.04.030. PMC 6097523. PMID 29910114.
- ^ Menzies D, Al Jahdali H, Al Otaibi B (March 2011). «Recent developments in treatment of latent tuberculosis infection». The Indian Journal of Medical Research. 133 (3): 257–66. PMC 3103149. PMID 21441678.
- ^ M’imunya JM, Kredo T, Volmink J, et al. (Cochrane Infectious Diseases Group) (May 2012). «Patient education and counselling for promoting adherence to treatment for tuberculosis». The Cochrane Database of Systematic Reviews. 2012 (5): CD006591. doi:10.1002/14651858.CD006591.pub2. PMC 6532681. PMID 22592714.
- ^ Gelband H, et al. (Cochrane Infectious Diseases Group) (25 October 1999). «Regimens of less than six months for treating tuberculosis». The Cochrane Database of Systematic Reviews. 1999 (2): CD001362. doi:10.1002/14651858.CD001362. PMC 6532732. PMID 10796641.
- ^ Grace AG, Mittal A, Jain S, Tripathy JP, Satyanarayana S, Tharyan P, Kirubakaran R, et al. (Cochrane Infectious Diseases Group) (December 2019). «Shortened treatment regimens versus the standard regimen for drug-sensitive pulmonary tuberculosis». The Cochrane Database of Systematic Reviews. 12 (12): CD012918. doi:10.1002/14651858.CD012918.pub2. PMC 6953336. PMID 31828771.
- ^ «Landmark TB Trial Identifies Shorter-Course Treatment Regimen». CDC. NCHHSTP Media Team Centers for Disease Control and Prevention. 20 October 2020. Retrieved 27 November 2021.
- ^ Mainous III AB (2010). Management of Antimicrobials in Infectious Diseases: Impact of Antibiotic Resistance. Totowa, NJ: Humana Press. p. 69. ISBN 978-1-60327-238-4. Archived from the original on 6 September 2015.
- ^ a b c Karumbi J, Garner P (May 2015). «Directly observed therapy for treating tuberculosis». The Cochrane Database of Systematic Reviews. 2015 (5): CD003343. doi:10.1002/14651858.CD003343.pub4. PMC 4460720. PMID 26022367.
- ^ Liu Q, Abba K, Alejandria MM, Sinclair D, Balanag VM, Lansang MA, et al. (Cochrane Infectious Diseases Group) (November 2014). «Reminder systems to improve patient adherence to tuberculosis clinic appointments for diagnosis and treatment». The Cochrane Database of Systematic Reviews. 2014 (11): CD006594. doi:10.1002/14651858.CD006594.pub3. PMC 4448217. PMID 25403701.
- ^ Mwandumba HC, Squire SB, et al. (Cochrane Infectious Diseases Group) (23 October 2001). «Fully intermittent dosing with drugs for treating tuberculosis in adults». The Cochrane Database of Systematic Reviews (4): CD000970. doi:10.1002/14651858.CD000970. PMC 6532565. PMID 11687088.
- ^ Bose A, Kalita S, Rose W, Tharyan P, et al. (Cochrane Infectious Diseases Group) (January 2014). «Intermittent versus daily therapy for treating tuberculosis in children». The Cochrane Database of Systematic Reviews. 2014 (1): CD007953. doi:10.1002/14651858.CD007953.pub2. PMC 6532685. PMID 24470141.
- ^ O’Brien RJ (June 1994). «Drug-resistant tuberculosis: etiology, management and prevention». Seminars in Respiratory Infections. 9 (2): 104–12. PMID 7973169.
- ^ Centers for Disease Control and Prevention (CDC) (March 2006). «Emergence of Mycobacterium tuberculosis with extensive resistance to second-line drugs—worldwide, 2000-2004». MMWR. Morbidity and Mortality Weekly Report. 55 (11): 301–5. PMID 16557213. Archived from the original on 22 May 2017.
- ^ a b McKenna M (12 January 2012). «Totally Resistant TB: Earliest Cases in Italy». Wired. Archived from the original on 14 January 2012. Retrieved 12 January 2012.
- ^ Migliori GB, De Iaco G, Besozzi G, Centis R, Cirillo DM (May 2007). «First tuberculosis cases in Italy resistant to all tested drugs». Euro Surveillance. 12 (5): E070517.1. doi:10.2807/esw.12.20.03194-en. PMID 17868596.
- ^ «Totally Drug-Resistant TB: a WHO consultation on the diagnostic definition and treatment options» (PDF). World Health Organization (WHO). Archived (PDF) from the original on 21 October 2016. Retrieved 25 March 2016.
- ^ a b c d e f g h i j k l m n o p Kielstra P (30 June 2014). Tabary Z (ed.). «Ancient enemy, modern imperative – A time for greater action against tuberculosis» (PDF). The Economist. Economist Intelligence Unit. Archived from the original (PDF) on 31 July 2014. Retrieved 22 January 2022.
- ^ Singh B, Cocker D, Ryan H, Sloan DJ, et al. (Cochrane Infectious Diseases Group) (March 2019). «Linezolid for drug-resistant pulmonary tuberculosis». The Cochrane Database of Systematic Reviews. 3 (3): CD012836. doi:10.1002/14651858.CD012836.pub2. PMC 6426281. PMID 30893466.
- ^ Velayati AA, Masjedi MR, Farnia P, Tabarsi P, Ghanavi J, ZiaZarifi AH, Hoffner SE (August 2009). «Emergence of new forms of totally drug-resistant tuberculosis bacilli: super extensively drug-resistant tuberculosis or totally drug-resistant strains in Iran». Chest. 136 (2): 420–425. doi:10.1378/chest.08-2427. PMID 19349380.
- ^ «Provisional CDC Guidelines for the Use and Safety Monitoring of Bedaquiline Fumarate (Sirturo) for the Treatment of Multidrug-Resistant Tuberculosis». Archived from the original on 4 January 2014.
- ^ Theron G, Peter J, Richardson M, Warren R, Dheda K, Steingart KR, et al. (Cochrane Infectious Diseases Group) (September 2016). «® MTBDRsl assay for resistance to second-line anti-tuberculosis drugs». The Cochrane Database of Systematic Reviews. 2016 (9): CD010705. doi:10.1002/14651858.CD010705.pub3. PMC 5034505. PMID 27605387.
- ^ «The use of molecular line probe assays for the detection of resistance to second-line anti-tuberculosis drugs» (PDF). World Health Organization. Archived (PDF) from the original on 22 September 2021. Retrieved 18 June 2021.
- ^ «WHO Disease and injury country estimates». World Health Organization (WHO). 2004. Archived from the original on 11 November 2009. Retrieved 11 November 2009.
- ^ Lambert ML, Hasker E, Van Deun A, Roberfroid D, Boelaert M, Van der Stuyft P (May 2003). «Recurrence in tuberculosis: relapse or reinfection?». The Lancet. Infectious Diseases. 3 (5): 282–7. doi:10.1016/S1473-3099(03)00607-8. PMID 12726976.
- ^ Wang JY, Lee LN, Lai HC, Hsu HL, Liaw YS, Hsueh PR, Yang PC (July 2007). «Prediction of the tuberculosis reinfection proportion from the local incidence». The Journal of Infectious Diseases. 196 (2): 281–8. doi:10.1086/518898. PMID 17570116.
- ^ «1.4 Prognosis — Tuberculosis». medicalguidelines.msf.org. Archived from the original on 2 June 2021. Retrieved 25 August 2020.
- ^ «Fact Sheets: The Difference Between Latent TB Infection and Active TB Disease». Centers for Disease Control and Prevention (CDC). 20 June 2011. Archived from the original on 4 August 2011. Retrieved 26 July 2011.
- ^ «Global tuberculosis report 2013». World Health Organization (WHO). 2013. Archived from the original on 12 December 2006.
- ^ Lozano R, Naghavi M, Foreman K, Lim S, Shibuya K, Aboyans V, et al. (December 2012). «Global and regional mortality from 235 causes of death for 20 age groups in 1990 and 2010: a systematic analysis for the Global Burden of Disease Study 2010». Lancet. 380 (9859): 2095–128. doi:10.1016/S0140-6736(12)61728-0. hdl:10536/DRO/DU:30050819. PMID 23245604. S2CID 1541253. Archived from the original on 19 May 2020. Retrieved 18 March 2020.
- ^ a b c «Global Tuberculosis Control 2011» (PDF). World Health Organization (WHO). Archived from the original (PDF) on 17 June 2012. Retrieved 15 April 2012.
- ^ «Tuberculosis». WHO. 24 March 2020. Archived from the original on 30 July 2020. Retrieved 31 May 2020.
- ^ Douglas AS, Strachan DP, Maxwell JD (September 1996). «Seasonality of tuberculosis: the reverse of other respiratory diseases in the UK». Thorax. 51 (9): 944–946. doi:10.1136/thx.51.9.944. PMC 472621. PMID 8984709.
- ^ Martineau AR, Nhamoyebonde S, Oni T, Rangaka MX, Marais S, Bangani N, et al. (November 2011). «Reciprocal seasonal variation in vitamin D status and tuberculosis notifications in Cape Town, South Africa». Proceedings of the National Academy of Sciences of the United States of America. 108 (47): 19013–19017. doi:10.1073/pnas.1111825108. PMC 3223428. PMID 22025704.
- ^ Parrinello CM, Crossa A, Harris TG (January 2012). «Seasonality of tuberculosis in New York City, 1990-2007». The International Journal of Tuberculosis and Lung Disease. 16 (1): 32–37. doi:10.5588/ijtld.11.0145. PMID 22236842.
- ^ a b Korthals Altes H, Kremer K, Erkens C, van Soolingen D, Wallinga J (May 2012). «Tuberculosis seasonality in the Netherlands differs between natives and non-natives: a role for vitamin D deficiency?». The International Journal of Tuberculosis and Lung Disease. 16 (5): 639–644. doi:10.5588/ijtld.11.0680. PMID 22410705.
- ^ Koh GC, Hawthorne G, Turner AM, Kunst H, Dedicoat M (2013). «Tuberculosis incidence correlates with sunshine: an ecological 28-year time series study». PLOS ONE. 8 (3): e57752. Bibcode:2013PLoSO…857752K. doi:10.1371/journal.pone.0057752. PMC 3590299. PMID 23483924.
- ^ Kuddus MA, McBryde ES, Adegboye OA (September 2019). «Delay effect and burden of weather-related tuberculosis cases in Rajshahi province, Bangladesh, 2007-2012». Scientific Reports. 9 (1): 12720. Bibcode:2019NatSR…912720K. doi:10.1038/s41598-019-49135-8. PMC 6722246. PMID 31481739.
- ^ Griffith DE, Kerr CM (August 1996). «Tuberculosis: disease of the past, disease of the present». Journal of PeriAnesthesia Nursing. 11 (4): 240–45. doi:10.1016/S1089-9472(96)80023-2. PMID 8964016.
- ^ «Global Tuberculosis Control Report, 2006 – Annex 1 Profiles of high-burden countries» (PDF). World Health Organization (WHO). Archived from the original (PDF) on 26 July 2009. Retrieved 13 October 2006.
- ^ «2005 Surveillance Slide Set». Centers for Disease Control and Prevention. 12 September 2006. Archived from the original on 23 November 2006. Retrieved 13 October 2006.
- ^ FitzGerald JM, Wang L, Elwood RK (February 2000). «Tuberculosis: 13. Control of the disease among aboriginal people in Canada». Canadian Medical Association Journal. 162 (3): 351–55. PMC 1231016. PMID 10693593.
- ^ Quah SR, Carrin G, Buse K, Heggenhougen K (2009). Health Systems Policy, Finance, and Organization. Boston: Academic Press. p. 424. ISBN 978-0-12-375087-7. Archived from the original on 6 September 2015.
- ^ Medical Research Council.Origins of the MRC. Archived 11 April 2008 at the Wayback Machine Accessed 7 October 2006.
- ^ DaVanzo, Julie; Farnsworth, Gwen (1 January 1996). «Russia’s Demographic».
- ^ Global Tuberculosis Control Archived 12 December 2006 at the Wayback Machine, World Health Organization, 2011.
- ^ «WHO global tuberculosis report 2016. Annex 2. Country profiles: Russian Federation». Archived from the original on 14 July 2017. Retrieved 22 August 2020.
- ^ a b c «Global Tuberculosis Report 2018» (PDF). Archived (PDF) from the original on 7 August 2020. Retrieved 27 September 2019.
- ^ «WHO Global tuberculosis report 2016: India». Archived from the original on 6 February 2018. Retrieved 22 August 2020.
- ^ «Govt revisits strategy to combat tuberculosis». Daily News and Analysis. 8 April 2017. Archived from the original on 3 June 2021. Retrieved 22 August 2020.
- ^ Mahla RS (August 2018). «Prevalence of drug-resistant tuberculosis in South Africa». The Lancet. Infectious Diseases. 18 (8): 836. doi:10.1016/S1473-3099(18)30401-8. PMID 30064674.
- ^ Birn AE (2009). Textbook of International Health: Global Health in a Dynamic World. p. 261. ISBN 978-0-19-988521-3. Archived from the original on 6 September 2015.
- ^ «CDC Surveillance Slides 2012 – TB». Centers for Disease Control and Prevention. 24 October 2018. Archived from the original on 9 November 2013. Retrieved 17 September 2017.
- ^ Al-Azem A, Kaushal Sharma M, Turenne C, Hoban D, Hershfield E, MacMorran J, Kabani A (1998). «Rural outbreaks of Mycobacterium tuberculosis in a Canadian province». Abstr Intersci Conf Antimicrob Agents Chemother. 38: 555. abstract no. L-27. Archived from the original on 18 November 2011.
- ^ «Tuberculosis incidence (per 100,000 people)». Our World in Data. Archived from the original on 26 September 2019. Retrieved 7 March 2020.
- ^ «Tuberculosis deaths by region». Our World in Data. Archived from the original on 8 May 2020. Retrieved 7 March 2020.
- ^ Rothschild BM, Martin LD, Lev G, Bercovier H, Bar-Gal GK, Greenblatt C, et al. (August 2001). «Mycobacterium tuberculosis complex DNA from an extinct bison dated 17,000 years before the present». Clinical Infectious Diseases. 33 (3): 305–11. doi:10.1086/321886. PMID 11438894.
- ^ Pearce-Duvet JM (August 2006). «The origin of human pathogens: evaluating the role of agriculture and domestic animals in the evolution of human disease». Biological Reviews of the Cambridge Philosophical Society. 81 (3): 369–82. doi:10.1017/S1464793106007020. PMID 16672105. S2CID 6577678.
- ^ Comas I, Gagneux S (October 2009). Manchester M (ed.). «The past and future of tuberculosis research». PLOS Pathogens. 5 (10): e1000600. doi:10.1371/journal.ppat.1000600. PMC 2745564. PMID 19855821.
- ^ Zink AR, Sola C, Reischl U, Grabner W, Rastogi N, Wolf H, et al. (January 2003). «Characterization of Mycobacterium tuberculosis complex DNAs from Egyptian mummies by spoligotyping». Journal of Clinical Microbiology. 41 (1): 359–67. doi:10.1128/JCM.41.1.359-367.2003. PMC 149558. PMID 12517873.
- ^ Konomi N, Lebwohl E, Mowbray K, Tattersall I, Zhang D (December 2002). «Detection of mycobacterial DNA in Andean mummies». Journal of Clinical Microbiology. 40 (12): 4738–40. doi:10.1128/JCM.40.12.4738-4740.2002. PMC 154635. PMID 12454182.
- ^ Sledzik PS, Bellantoni N (June 1994). «Brief communication: bioarcheological and biocultural evidence for the New England vampire folk belief» (PDF). American Journal of Physical Anthropology. 94 (2): 269–74. doi:10.1002/ajpa.1330940210. PMID 8085617. Archived (PDF) from the original on 18 February 2017.
- ^ Léon Charles Albert Calmette at Who Named It?
- ^ Trail RR (April 1970). «Richard Morton (1637-1698)». Medical History. 14 (2): 166–74. doi:10.1017/S0025727300015350. PMC 1034037. PMID 4914685.
- ^ Marten B (1720). A New Theory of Consumptions—More Especially a Phthisis or Consumption of the Lungs. London, England: T. Knaplock. P. 51: «The Original and Essential Cause … may possibly be some certain Species of Animalcula or wonderfully minute living Creatures, … » P. 79: «It may be therefore very likely, that by an habitual lying in the same Bed with a Consumptive Patient, constantly Eating and Drinking with him, or by very frequently conversing so nearly, as to draw in part of the Breath he emits from his Lungs, a Consumption may be caught by a sound Person; … «
- ^ Laennec RT (1819). De l’auscultation médiate … (in French). Vol. 1. Paris, France: J.-A. Brosson et J.-S Chaudé. p. 20. Archived from the original on 2 June 2021. Retrieved 6 December 2020. From p. 20: «L’existence des tubercules dans le poumon est la cause et constitue le charactère anatomique propre de la phthisie pulmonaire (a). (a) … l’effet dont cette maladie tire son nom, c’est-à-dire, la consumption.» (The existence of tubercles in the lung is the cause and constitutes the unique anatomical characteristic of pulmonary tuberculosis (a). (a) … the effect from which this malady [pulmonary tuberculosis] takes its name, that is, consumption.)
- ^ Schönlein JL (1832). Allgemeine und specielle Pathologie und Therapie [General and Special Pathology and Therapy] (in German). Vol. 3. Würzburg, (Germany): C. Etlinger. p. 103. Archived from the original on 2 June 2021. Retrieved 6 December 2020.
- ^ The word «tuberculosis» first appeared in Schönlein’s clinical notes in 1829. See: Jay SJ, Kırbıyık U, Woods JR, Steele GA, Hoyt GR, Schwengber RB, Gupta P (November 2018). «Modern theory of tuberculosis: culturomic analysis of its historical origin in Europe and North America». The International Journal of Tuberculosis and Lung Disease. 22 (11): 1249–1257. doi:10.5588/ijtld.18.0239. PMID 30355403. S2CID 53027676. See especially Appendix, p. iii.
- ^ Kentucky: Mammoth Cave long on history. Archived 13 August 2006 at the Wayback Machine CNN. 27 February 2004. Accessed 8 October 2006.
- ^ a b c McCarthy OR (August 2001). «The key to the sanatoria». Journal of the Royal Society of Medicine. 94 (8): 413–17. doi:10.1177/014107680109400813. PMC 1281640. PMID 11461990. Archived from the original on 3 August 2012. Retrieved 28 September 2011.
- ^ Villemin JA (1865). «Cause et nature de la tuberculose» [Cause and nature of tuberculosis]. Bulletin de l’Académie Impériale de Médecine (in French). 31: 211–216.
- See also: Villemin JA (1868). Etudes sur la tuberculose: preuves rationnelles et expérimentales de sa spécificité et de son inoculabilité [Studies of tuberculosis: rational and experimental evidence of its specificity and inoculability] (in French). Paris, France: J.-B. Baillière et fils.
- ^ Burdon-Sanderson, John Scott. (1870) «Introductory Report on the Intimate Pathology of Contagion.» Appendix to: Twelfth Report to the Lords of Her Majesty’s Most Honourable Privy Council of the Medical Officer of the Privy Council [for the year 1869], Parliamentary Papers (1870), vol. 38, 229–256.
- ^ Koch R (24 March 1882). «Die Ätiologie der Tuberkulose» [The Etiology of Tuberculosis]. Berliner Klinische Wochenschrift. 19: 221–30. doi:10.1007/978-3-662-56454-7_4. ISBN 978-3-662-56454-7. Archived from the original on 6 November 2018. Retrieved 15 June 2021.
- ^ «History: World TB Day». Centers for Disease Control and Prevention (CDC). 12 December 2016. Archived from the original on 7 December 2018. Retrieved 23 March 2019.
- ^ «The Nobel Prize in Physiology or Medicine 1905». NobelPrize.org. Retrieved 20 February 2023.
- ^ Waddington K (January 2004). «To stamp out ‘so terrible a malady’: bovine tuberculosis and tuberculin testing in Britain, 1890–1939». Medical History. 48 (1): 29–48. doi:10.1017/S0025727300007043. PMC 546294. PMID 14968644.
- ^ Bonah C (December 2005). «The ‘experimental stable’ of the BCG vaccine: safety, efficacy, proof, and standards, 1921–1933». Studies in History and Philosophy of Biological and Biomedical Sciences. 36 (4): 696–721. doi:10.1016/j.shpsc.2005.09.003. PMID 16337557.
- ^ Comstock GW (September 1994). «The International Tuberculosis Campaign: a pioneering venture in mass vaccination and research». Clinical Infectious Diseases. 19 (3): 528–40. doi:10.1093/clinids/19.3.528. PMID 7811874.
- ^ Hannaway C (2008). Biomedicine in the twentieth century: practices, policies, and politics. Amsterdam: IOS Press. p. 233. ISBN 978-1-58603-832-8. Archived from the original on 7 September 2015.
- ^ Bloom BR (1994). Tuberculosis: pathogenesis, protection, and control. Washington, DC: ASM Press. ISBN 978-1-55581-072-6.
- ^ Frith J. «History of Tuberculosis. Part 1 – Phthisis, consumption and the White Plague». Journal of Military and Veterans’ Health. Archived from the original on 8 April 2021. Retrieved 26 February 2021.
- ^ Zürcher K, Zwahlen M, Ballif M, Rieder HL, Egger M, Fenner L (5 October 2016). «Influenza Pandemics and Tuberculosis Mortality in 1889 and 1918: Analysis of Historical Data from Switzerland». PLOS ONE. 11 (10): e0162575. Bibcode:2016PLoSO..1162575Z. doi:10.1371/journal.pone.0162575. PMC 5051959. PMID 27706149.
- ^ a b
- ^ Shields T (2009). General thoracic surgery (7th ed.). Philadelphia: Wolters Kluwer Health/Lippincott Williams & Wilkins. p. 792. ISBN 978-0-7817-7982-1. Archived from the original on 6 September 2015.
- ^ Lalloo UG, Naidoo R, Ambaram A (May 2006). «Recent advances in the medical and surgical treatment of multi-drug resistant tuberculosis». Current Opinion in Pulmonary Medicine. 12 (3): 179–85. doi:10.1097/01.mcp.0000219266.27439.52. PMID 16582672. S2CID 24221563.
- ^ «Frequently asked questions about TB and HIV». World Health Organization (WHO). Archived from the original on 8 August 2011. Retrieved 15 April 2012.
- ^ a b c Lawlor C. «Katherine Byrne, Tuberculosis and the Victorian Literary Imagination». British Society for Literature and Science. Archived from the original on 6 November 2020. Retrieved 11 June 2017.
- ^ «Hippocrates 3.16 Classics, MIT». Archived from the original on 11 February 2005. Retrieved 15 December 2015.
{{cite web}}: CS1 maint: unfit URL (link) - ^ Caldwell M (1988). The Last Crusade. New York: Macmillan. p. 21. ISBN 978-0-689-11810-4.
- ^ Bunyan J (1808). The Life and Death of Mr. Badman. London: W. Nicholson. p. 244. Retrieved 28 September 2016 – via Internet Archive.
captain.
- ^ Byrne K (2011). Tuberculosis and the Victorian Literary Imagination. Cambridge University Press. ISBN 978-1-107-67280-2.
- ^ «About Chopin’s illness». Icons of Europe. Archived from the original on 28 September 2017. Retrieved 11 June 2017.
- ^ Vilaplana C (March 2017). «A literary approach to tuberculosis: lessons learned from Anton Chekhov, Franz Kafka, and Katherine Mansfield». International Journal of Infectious Diseases. 56: 283–85. doi:10.1016/j.ijid.2016.12.012. PMID 27993687.
- ^ Rogal SJ (1997). A William Somerset Maugham Encyclopedia. Greenwood Publishing. p. 245. ISBN 978-0-313-29916-2. Archived from the original on 2 June 2021. Retrieved 4 October 2017.
- ^ Eschner K. «George Orwell Wrote ‘1984’ While Dying of Tuberculosis». Smithsonian. Archived from the original on 24 March 2019. Retrieved 25 March 2019.
- ^ «Tuberculosis (whole issue)». Journal of the American Medical Association. 293 (22): cover. 8 June 2005. Archived from the original on 24 August 2020. Retrieved 4 October 2017.
- ^ Lemlein RF (1981). «Influence of Tuberculosis on the Work of Visual Artists: Several Prominent Examples». Leonardo. 14 (2): 114–11. doi:10.2307/1574402. JSTOR 1574402. S2CID 191371443. Archived from the original on 27 August 2021. Retrieved 31 January 2020.
- ^ Wilsey AM (May 2012). ‘Half in Love with Easeful Death:’ Tuberculosis in Literature. Humanities Capstone Projects (PhD Thesis thesis). Pacific University. Archived from the original on 11 October 2017. Retrieved 28 September 2017.
- ^ a b Morens DM (November 2002). «At the deathbed of consumptive art». Emerging Infectious Diseases. 8 (11): 1353–8. doi:10.3201/eid0811.020549. PMC 2738548. PMID 12463180.
- ^ «Pulmonary Tuberculosis/In Literature and Art». McMaster University History of Diseases. Retrieved 9 June 2017.
- ^ Thomson G (1 June 2016). «Van Morrison – 10 of the best». The Guardian. Archived from the original on 14 August 2020. Retrieved 28 September 2017.
- ^ «Tuberculosis Throughout History: The Arts» (PDF). United States Agency for International Development (USAID). Archived (PDF) from the original on 30 June 2017. Retrieved 12 June 2017.
- ^ Corliss R (22 December 2008). «Top 10 Worst Christmas Movies». Time. Archived from the original on 22 September 2020. Retrieved 28 September 2017.
‘If you don’t cry when Bing Crosby tells Ingrid Bergman she has tuberculosis’, Joseph McBride wrote in 1973, ‘I never want to meet you, and that’s that.’
- ^ «The End TB Strategy». who.int. Archived from the original on 22 July 2021. Retrieved 22 July 2021.
- ^ a b c d Global tuberculosis report 2020. World Health Organization. 2020. ISBN 978-92-4-001313-1. Archived from the original on 22 July 2021. Retrieved 22 July 2021.
- ^ a b «Public–Private Partnership Announces Immediate 40 Percent Cost Reduction for Rapid TB Test» (PDF). World Health Organization (WHO). 6 August 2012. Archived (PDF) from the original on 29 October 2013.
- ^ Lawn SD, Nicol MP (September 2011). «Xpert® MTB/RIF assay: development, evaluation and implementation of a new rapid molecular diagnostic for tuberculosis and rifampicin resistance». Future Microbiology. 6 (9): 1067–82. doi:10.2217/fmb.11.84. PMC 3252681. PMID 21958145.
- ^ «WHO says Cepheid rapid test will transform TB care». Reuters. 8 December 2010. Archived from the original on 11 December 2010.
- ^ STOPTB (5 April 2013). «The Stop TB Partnership, which operates through a secretariat hosted by the World Health Organization (WHO) in Geneva, Switzerland» (PDF). Archived (PDF) from the original on 24 January 2014.
- ^ Lienhardt C, Espinal M, Pai M, Maher D, Raviglione MC (November 2011). «What research is needed to stop TB? Introducing the TB Research Movement». PLOS Medicine. 8 (11): e1001135. doi:10.1371/journal.pmed.1001135. PMC 3226454. PMID 22140369.
- ^ Sandhu GK (2011). «Tuberculosis: Current Situation, Challenges and Overview of its Control Programs in India». Journal of Global Infectious Diseases. 3 (2): 143–150. doi:10.4103/0974-777X.81691. ISSN 0974-777X. PMC 3125027. PMID 21731301.
- ^ Bhargava A, Pinto L, Pai M (2011). «Mismanagement of tuberculosis in India: Causes, consequences, and the way forward» (PDF). Hypothesis. 9 (1): e7. Archived from the original on 14 March 2016.
{{cite journal}}: CS1 maint: unfit URL (link) - ^ Amdekar Y (July 2009). «Changes in the management of tuberculosis». Indian Journal of Pediatrics. 76 (7): 739–42. doi:10.1007/s12098-009-0164-4. PMID 19693453. S2CID 41788291. Archived from the original on 27 August 2021. Retrieved 31 January 2020.
- ^ Fox GJ, Dobler CC, Marks GB (September 2011). «Active case finding in contacts of people with tuberculosis». The Cochrane Database of Systematic Reviews. 2011 (9): CD008477. doi:10.1002/14651858.CD008477.pub2. PMC 6532613. PMID 21901723.
- ^ Mhimbira FA, Cuevas LE, Dacombe R, Mkopi A, Sinclair D, et al. (Cochrane Infectious Diseases Group) (November 2017). «Interventions to increase tuberculosis case detection at primary healthcare or community-level services». The Cochrane Database of Systematic Reviews. 2017 (11): CD011432. doi:10.1002/14651858.CD011432.pub2. PMC 5721626. PMID 29182800.
- ^ Braganza Menezes D, Menezes B, Dedicoat M, et al. (Cochrane Infectious Diseases Group) (August 2019). «Contact tracing strategies in household and congregate environments to identify cases of tuberculosis in low- and moderate-incidence populations». The Cochrane Database of Systematic Reviews. 2019 (8): CD013077. doi:10.1002/14651858.CD013077.pub2. PMC 6713498. PMID 31461540.
- ^ a b c d e f g Courtwright A, Turner AN (July–August 2010). «Tuberculosis and stigmatization: pathways and interventions». Public Health Reports. 125 Suppl 4 (4_suppl): 34–42. doi:10.1177/00333549101250S407. PMC 2882973. PMID 20626191.
- ^ Mason PH, Roy A, Spillane J, Singh P (March 2016). «Social, Historical and Cultural Dimensions of Tuberculosis». Journal of Biosocial Science. 48 (2): 206–32. doi:10.1017/S0021932015000115. PMID 25997539.
- ^ a b c Martín Montañés C, Gicquel B (March 2011). «New tuberculosis vaccines». Enfermedades Infecciosas y Microbiologia Clinica. 29 Suppl 1: 57–62. doi:10.1016/S0213-005X(11)70019-2. PMID 21420568.
- ^ Zhu B, Dockrell HM, Ottenhoff TH, Evans TG, Zhang Y (April 2018). «Tuberculosis vaccines: Opportunities and challenges». Respirology. 23 (4): 359–368. doi:10.1111/resp.13245. PMID 29341430.
- ^ Ibanga HB, Brookes RH, Hill PC, Owiafe PK, Fletcher HA, Lienhardt C, et al. (August 2006). «Early clinical trials with a new tuberculosis vaccine, MVA85A, in tuberculosis-endemic countries: issues in study design». The Lancet. Infectious Diseases. 6 (8): 522–8. doi:10.1016/S1473-3099(06)70552-7. PMID 16870530.
- ^ Kaufmann SH (October 2010). «Future vaccination strategies against tuberculosis: thinking outside the box». Immunity. 33 (4): 567–77. doi:10.1016/j.immuni.2010.09.015. PMID 21029966.
- ^ Webber D, Kremer M (2001). «Stimulating Industrial R&D for Neglected Infectious Diseases: Economic Perspectives» (PDF). Bulletin of the World Health Organization. 79 (8): 693–801. Archived (PDF) from the original on 26 September 2007.
- ^ Barder O, Kremer M, Williams H (2006). «Advance Market Commitments: A Policy to Stimulate Investment in Vaccines for Neglected Diseases». The Economists’ Voice. 3 (3). doi:10.2202/1553-3832.1144. S2CID 154454583. Archived from the original on 5 November 2006.
- ^ Department of Economic and Social Affairs (2009). Achieving the global public health agenda: dialogues at the Economic and Social Council. New York: United Nations. p. 103. ISBN 978-92-1-104596-3. Archived from the original on 6 September 2015.
- ^ Jong EC, Zuckerman JN (2010). Travelers’ vaccines (2nd ed.). Shelton, CT: People’s Medical Publishing House. p. 319. ISBN 978-1-60795-045-5. Archived from the original on 6 September 2015.
- ^ Bill and Melinda Gates Foundation Announcement (12 February 2004). «Gates Foundation Commits $82.9 Million to Develop New Tuberculosis Vaccines». Archived from the original on 10 October 2009.
- ^ Nightingale K (19 September 2007). «Gates foundation gives US$280 million to fight TB». Archived from the original on 1 December 2008.
- ^ a b Zumla A, Hafner R, Lienhardt C, Hoelscher M, Nunn A (March 2012). «Advancing the development of tuberculosis therapy». Nature Reviews. Drug Discovery. 11 (3): 171–2. doi:10.1038/nrd3694. PMID 22378254. S2CID 7232434. Archived from the original on 12 January 2020. Retrieved 8 May 2020.
- ^ «J&J Sirturo Wins FDA Approval to Treat Drug-Resistant TB». Bloomberg News. 31 December 2012. Archived from the original on 4 January 2013. Retrieved 1 January 2013.
- ^ a b Avorn J (April 2013). «Approval of a tuberculosis drug based on a paradoxical surrogate measure». JAMA. 309 (13): 1349–50. doi:10.1001/jama.2013.623. PMID 23430122.
- ^ US Food and Drug Administration. «Briefing Package: NDA 204–384: Sirturo» (PDF). Food and Drug Administration. Archived (PDF) from the original on 4 January 2014.
- ^ Zuckerman D, Yttri J (January 2013). «Antibiotics: When science and wishful thinking collide». Health Affairs. doi:10.1377/forefront.20130125.027503.
- ^ Critchley JA, Orton LC, Pearson F (November 2014). «Adjunctive steroid therapy for managing pulmonary tuberculosis». The Cochrane Database of Systematic Reviews. 2014 (11): CD011370. doi:10.1002/14651858.CD011370. PMC 6532561. PMID 25387839.
- ^ Shivaprasad HL, Palmieri C (January 2012). «Pathology of mycobacteriosis in birds». The Veterinary Clinics of North America. Exotic Animal Practice. 15 (1): 41–55, v–vi. doi:10.1016/j.cvex.2011.11.004. PMID 22244112.
- ^ Reavill DR, Schmidt RE (January 2012). «Mycobacterial lesions in fish, amphibians, reptiles, rodents, lagomorphs, and ferrets with reference to animal models». The Veterinary Clinics of North America. Exotic Animal Practice. 15 (1): 25–40, v. doi:10.1016/j.cvex.2011.10.001. PMID 22244111.
- ^ Mitchell MA (January 2012). «Mycobacterial infections in reptiles». The Veterinary Clinics of North America. Exotic Animal Practice. 15 (1): 101–11, vii. doi:10.1016/j.cvex.2011.10.002. PMID 22244116.
- ^ Wobeser GA (2006). Essentials of disease in wild animals (1st ed.). Ames, IO [u.a.]: Blackwell Publishing. p. 170. ISBN 978-0-8138-0589-4. Archived from the original on 6 September 2015.
- ^ Ryan TJ, Livingstone PG, Ramsey DS, de Lisle GW, Nugent G, Collins DM, et al. (February 2006). «Advances in understanding disease epidemiology and implications for control and eradication of tuberculosis in livestock: the experience from New Zealand». Veterinary Microbiology. 112 (2–4): 211–19. doi:10.1016/j.vetmic.2005.11.025. PMID 16330161.
- ^ White PC, Böhm M, Marion G, Hutchings MR (September 2008). «Control of bovine tuberculosis in British livestock: there is no ‘silver bullet’«. Trends in Microbiology. 16 (9): 420–7. CiteSeerX 10.1.1.566.5547. doi:10.1016/j.tim.2008.06.005. PMID 18706814.
- ^ Ward AI, Judge J, Delahay RJ (January 2010). «Farm husbandry and badger behaviour: opportunities to manage badger to cattle transmission of Mycobacterium bovis?». Preventive Veterinary Medicine. 93 (1): 2–10. doi:10.1016/j.prevetmed.2009.09.014. PMID 19846226.
- ^ Holt N (24 March 2015). «The Infected Elephant in the Room». Slate. Archived from the original on 14 April 2016. Retrieved 5 April 2016.
- ^ Mikota SK. «A Brief History of TB in Elephants» (PDF). Animal and Plant Health Inspection Service (APHIS). Archived (PDF) from the original on 6 October 2016. Retrieved 5 April 2016.
External links
- Tuberculosis at Curlie
- «Tuberculosis (TB)». Centers for Disease Control and Prevention (CDC). 24 October 2018.
- «Tuberculosis (TB)». London: Health Protection Agency. Archived from the original on 5 July 2007.
- WHO global 2016 TB report (infographic)
- WHO tuberculosis country profiles
- «Tuberculosis Among African Americans», 1990-11-01, In Black America; KUT Radio, American Archive of Public Broadcasting (WGBH and the Library of Congress)
- Working Group on New TB drugs, tracking clinical trials and drug candidates
| Tuberculosis | |
|---|---|
| Other names | Phthisis, phthisis pulmonalis, consumption, great white plague |
|
|
| Chest X-ray of a person with advanced tuberculosis: Infection in both lungs is marked by white arrow-heads, and the formation of a cavity is marked by black arrows. | |
| Specialty | Infectious disease, pulmonology |
| Symptoms | Chronic cough, fever, cough with bloody mucus, weight loss[1] |
| Causes | Mycobacterium tuberculosis[1] |
| Risk factors | Smoking, HIV/AIDS[1] |
| Diagnostic method | CXR, culture, tuberculin skin test, QuantiFERON[1] |
| Differential diagnosis | Pneumonia, histoplasmosis, sarcoidosis, coccidioidomycosis[2] |
| Prevention | Screening those at high risk, treatment of those infected, vaccination with bacillus Calmette-Guérin (BCG)[3][4][5] |
| Treatment | Antibiotics[1] |
| Frequency | 25% of people (latent TB)[6] |
| Deaths | 1.5 million (2020)[7] |
Depiction of a man with tuberculosis
Tuberculosis (TB) is an infectious disease usually caused by Mycobacterium tuberculosis (MTB) bacteria.[1] Tuberculosis generally affects the lungs, but it can also affect other parts of the body.[1] Most infections show no symptoms, in which case it is known as latent tuberculosis.[1] Around 10% of latent infections progress to active disease which, if left untreated, kill about half of those affected.[1] Typical symptoms of active TB are chronic cough with blood-containing mucus, fever, night sweats, and weight loss.[1] It was historically referred to as consumption due to the weight loss associated with the disease.[8] Infection of other organs can cause a wide range of symptoms.[9]
Tuberculosis is spread from one person to the next through the air when people who have active TB in their lungs cough, spit, speak, or sneeze.[1][10] People with Latent TB do not spread the disease.[1] Active infection occurs more often in people with HIV/AIDS and in those who smoke.[1] Diagnosis of active TB is based on chest X-rays, as well as microscopic examination and culture of body fluids.[11] Diagnosis of Latent TB relies on the tuberculin skin test (TST) or blood tests.[11]
Prevention of TB involves screening those at high risk, early detection and treatment of cases, and vaccination with the bacillus Calmette-Guérin (BCG) vaccine.[3][4][5] Those at high risk include household, workplace, and social contacts of people with active TB.[4] Treatment requires the use of multiple antibiotics over a long period of time.[1] Antibiotic resistance is a growing problem with increasing rates of multiple drug-resistant tuberculosis (MDR-TB).[1]
In 2018, one quarter of the world’s population was thought to have a latent infection of TB.[6] New infections occur in about 1% of the population each year.[12] In 2020, an estimated 10 million people developed active TB, resulting in 1.5 million deaths, making it the second leading cause of death from an infectious disease after COVID-19.[13] As of 2018, most TB cases occurred in the regions of South-East Asia (44%), Africa (24%), and the Western Pacific (18%), with more than 50% of cases being diagnosed in seven countries: India (27%), China (9%), Indonesia (8%), the Philippines (6%), Pakistan (6%), Nigeria (4%), and Bangladesh (4%).[14] By 2021 the number of new cases each year was decreasing by around 2% annually.[13][1] About 80% of people in many Asian and African countries test positive while 5–10% of people in the United States population test positive via the tuberculin test.[15] Tuberculosis has been present in humans since ancient times.[16]
Signs and symptoms
The main symptoms of variants and stages of tuberculosis are given,[17] with many symptoms overlapping with other variants, while others are more (but not entirely) specific for certain variants. Multiple variants may be present simultaneously.
Tuberculosis may infect any part of the body, but most commonly occurs in the lungs (known as pulmonary tuberculosis).[9] Extrapulmonary TB occurs when tuberculosis develops outside of the lungs, although extrapulmonary TB may coexist with pulmonary TB.[9]
General signs and symptoms include fever, chills, night sweats, loss of appetite, weight loss, and fatigue.[9] Significant nail clubbing may also occur.[18]
Pulmonary
If a tuberculosis infection does become active, it most commonly involves the lungs (in about 90% of cases).[16][19] Symptoms may include chest pain and a prolonged cough producing sputum. About 25% of people may not have any symptoms (i.e., they remain asymptomatic).[16] Occasionally, people may cough up blood in small amounts, and in very rare cases, the infection may erode into the pulmonary artery or a Rasmussen’s aneurysm, resulting in massive bleeding.[9][20] Tuberculosis may become a chronic illness and cause extensive scarring in the upper lobes of the lungs. The upper lung lobes are more frequently affected by tuberculosis than the lower ones.[9] The reason for this difference is not clear.[15] It may be due to either better air flow,[15] or poor lymph drainage within the upper lungs.[9]
In 15–20% of active cases, the infection spreads outside the lungs, causing other kinds of TB.[21] These are collectively denoted as extrapulmonary tuberculosis. Extrapulmonary TB occurs more commonly in people with a weakened immune system and young children. In those with HIV, this occurs in more than 50% of cases. Notable extrapulmonary infection sites include the pleura (in tuberculous pleurisy), the central nervous system (in tuberculous meningitis), the lymphatic system (in scrofula of the neck), the genitourinary system (in urogenital tuberculosis), and the bones and joints (in Pott disease of the spine), among others. A potentially more serious, widespread form of TB is called «disseminated tuberculosis», it is also known as miliary tuberculosis.[9] Miliary TB currently makes up about 10% of extrapulmonary cases.[23]
Causes
Mycobacteria
The main cause of TB is Mycobacterium tuberculosis (MTB), a small, aerobic, nonmotile bacillus.[9] The high lipid content of this pathogen accounts for many of its unique clinical characteristics.[24] It divides every 16 to 20 hours, which is an extremely slow rate compared with other bacteria, which usually divide in less than an hour.[25] Mycobacteria have an outer membrane lipid bilayer.[26] If a Gram stain is performed, MTB either stains very weakly «Gram-positive» or does not retain dye as a result of the high lipid and mycolic acid content of its cell wall.[27] MTB can withstand weak disinfectants and survive in a dry state for weeks. In nature, the bacterium can grow only within the cells of a host organism, but M. tuberculosis can be cultured in the laboratory.[28]
Using histological stains on expectorated samples from phlegm (also called sputum), scientists can identify MTB under a microscope. Since MTB retains certain stains even after being treated with acidic solution, it is classified as an acid-fast bacillus.[15][27] The most common acid-fast staining techniques are the Ziehl–Neelsen stain[29] and the Kinyoun stain, which dye acid-fast bacilli a bright red that stands out against a blue background.[30] Auramine-rhodamine staining[31] and fluorescence microscopy[32] are also used.
The M. tuberculosis complex (MTBC) includes four other TB-causing mycobacteria: M. bovis, M. africanum, M. canetti, and M. microti.[33] M. africanum is not widespread, but it is a significant cause of tuberculosis in parts of Africa.[34][35] M. bovis was once a common cause of tuberculosis, but the introduction of pasteurized milk has almost eliminated this as a public health problem in developed countries.[15][36] M. canetti is rare and seems to be limited to the Horn of Africa, although a few cases have been seen in African emigrants.[37][38] M. microti is also rare and is seen almost only in immunodeficient people, although its prevalence may be significantly underestimated.[39]
Other known pathogenic mycobacteria include M. leprae, M. avium, and M. kansasii. The latter two species are classified as «nontuberculous mycobacteria» (NTM) or atypical mycobacteria. NTM cause neither TB nor leprosy, but they do cause lung diseases that resemble TB.[40]
Public health campaigns in the 1920s tried to halt the spread of TB.
Transmission
When people with active pulmonary TB cough, sneeze, speak, sing, or spit, they expel infectious aerosol droplets 0.5 to 5.0 µm in diameter. A single sneeze can release up to 40,000 droplets.[41] Each one of these droplets may transmit the disease, since the infectious dose of tuberculosis is very small (the inhalation of fewer than 10 bacteria may cause an infection).[42]
Risk of transmission
People with prolonged, frequent, or close contact with people with TB are at particularly high risk of becoming infected, with an estimated 22% infection rate.[43] A person with active but untreated tuberculosis may infect 10–15 (or more) other people per year.[44] Transmission should occur from only people with active TB – those with latent infection are not thought to be contagious.[15] The probability of transmission from one person to another depends upon several factors, including the number of infectious droplets expelled by the carrier, the effectiveness of ventilation, the duration of exposure, the virulence of the M. tuberculosis strain, the level of immunity in the uninfected person, and others.[45] The cascade of person-to-person spread can be circumvented by segregating those with active («overt») TB and putting them on anti-TB drug regimens. After about two weeks of effective treatment, subjects with nonresistant active infections generally do not remain contagious to others.[43] If someone does become infected, it typically takes three to four weeks before the newly infected person becomes infectious enough to transmit the disease to others.[46]
Risk factors
A number of factors make individuals more susceptible to TB infection and/or disease.[47]
Active disease risk
The most important risk factor globally for developing active TB is concurrent HIV infection; 13% of those with TB are also infected with HIV.[48] This is a particular problem in sub-Saharan Africa, where HIV infection rates are high.[49][50] Of those without HIV infection who are infected with tuberculosis, about 5–10% develop active disease during their lifetimes;[18] in contrast, 30% of those co-infected with HIV develop the active disease.[18]
Use of certain medications, such as corticosteroids and infliximab (an anti-αTNF monoclonal antibody), is another important risk factor, especially in the developed world.[16]
Other risk factors include: alcoholism,[16] diabetes mellitus (3-fold increased risk),[51] silicosis (30-fold increased risk),[52] tobacco smoking (2-fold increased risk),[53] indoor air pollution, malnutrition, young age,[47] recently acquired TB infection, recreational drug use, severe kidney disease, low body weight, organ transplant, head and neck cancer,[54] and genetic susceptibility[55] (the overall importance of genetic risk factors remains undefined[16]).
Infection susceptibility
Tobacco smoking increases the risk of infections (in addition to increasing the risk of active disease and death). Additional factors increasing infection susceptibility include young age.[47]
Pathogenesis
About 90% of those infected with M. tuberculosis have asymptomatic, latent TB infections (sometimes called LTBI),[57] with only a 10% lifetime chance that the latent infection will progress to overt, active tuberculous disease.[58] In those with HIV, the risk of developing active TB increases to nearly 10% a year.[58] If effective treatment is not given, the death rate for active TB cases is up to 66%.[44]
Microscopy of tuberculous epididymitis. H&E stain
TB infection begins when the mycobacteria reach the alveolar air sacs of the lungs, where they invade and replicate within endosomes of alveolar macrophages.[15][59][60] Macrophages identify the bacterium as foreign and attempt to eliminate it by phagocytosis. During this process, the bacterium is enveloped by the macrophage and stored temporarily in a membrane-bound vesicle called a phagosome. The phagosome then combines with a lysosome to create a phagolysosome. In the phagolysosome, the cell attempts to use reactive oxygen species and acid to kill the bacterium. However, M. tuberculosis has a thick, waxy mycolic acid capsule that protects it from these toxic substances. M. tuberculosis is able to reproduce inside the macrophage and will eventually kill the immune cell.
The primary site of infection in the lungs, known as the Ghon focus, is generally located in either the upper part of the lower lobe, or the lower part of the upper lobe.[15] Tuberculosis of the lungs may also occur via infection from the blood stream. This is known as a Simon focus and is typically found in the top of the lung.[61] This hematogenous transmission can also spread infection to more distant sites, such as peripheral lymph nodes, the kidneys, the brain, and the bones.[15][62] All parts of the body can be affected by the disease, though for unknown reasons it rarely affects the heart, skeletal muscles, pancreas, or thyroid.[63]
Tuberculosis is classified as one of the granulomatous inflammatory diseases. Macrophages, epithelioid cells, T lymphocytes, B lymphocytes, and fibroblasts aggregate to form granulomas, with lymphocytes surrounding the infected macrophages. When other macrophages attack the infected macrophage, they fuse together to form a giant multinucleated cell in the alveolar lumen. The granuloma may prevent dissemination of the mycobacteria and provide a local environment for interaction of cells of the immune system.[64] However, more recent evidence suggests that the bacteria use the granulomas to avoid destruction by the host’s immune system. Macrophages and dendritic cells in the granulomas are unable to present antigen to lymphocytes; thus the immune response is suppressed.[65] Bacteria inside the granuloma can become dormant, resulting in latent infection. Another feature of the granulomas is the development of abnormal cell death (necrosis) in the center of tubercles. To the naked eye, this has the texture of soft, white cheese and is termed caseous necrosis.[64]
If TB bacteria gain entry to the blood stream from an area of damaged tissue, they can spread throughout the body and set up many foci of infection, all appearing as tiny, white tubercles in the tissues.[66] This severe form of TB disease, most common in young children and those with HIV, is called miliary tuberculosis.[67] People with this disseminated TB have a high fatality rate even with treatment (about 30%).[23][68]
In many people, the infection waxes and wanes. Tissue destruction and necrosis are often balanced by healing and fibrosis.[64] Affected tissue is replaced by scarring and cavities filled with caseous necrotic material. During active disease, some of these cavities are joined to the air passages (bronchi) and this material can be coughed up. It contains living bacteria and thus can spread the infection. Treatment with appropriate antibiotics kills bacteria and allows healing to take place. Upon cure, affected areas are eventually replaced by scar tissue.[64]
Diagnosis
Active tuberculosis
Diagnosing active tuberculosis based only on signs and symptoms is difficult,[69] as is diagnosing the disease in those who have a weakened immune system.[70] A diagnosis of TB should, however, be considered in those with signs of lung disease or constitutional symptoms lasting longer than two weeks.[70] A chest X-ray and multiple sputum cultures for acid-fast bacilli are typically part of the initial evaluation.[70] Interferon-γ release assays (IGRA) and tuberculin skin tests are of little use in most of the developing world.[71][72] IGRA have similar limitations in those with HIV.[72][73]
A definitive diagnosis of TB is made by identifying M. tuberculosis in a clinical sample (e.g., sputum, pus, or a tissue biopsy). However, the difficult culture process for this slow-growing organism can take two to six weeks for blood or sputum culture.[74] Thus, treatment is often begun before cultures are confirmed.[75]
Nucleic acid amplification tests and adenosine deaminase testing may allow rapid diagnosis of TB.[69] Blood tests to detect antibodies are not specific or sensitive, so they are not recommended.[76]
Latent tuberculosis
Mantoux tuberculin skin test
The Mantoux tuberculin skin test is often used to screen people at high risk for TB.[70] Those who have been previously immunized with the Bacille Calmette-Guerin vaccine may have a false-positive test result.[77] The test may be falsely negative in those with sarcoidosis, Hodgkin’s lymphoma, malnutrition, and most notably, active tuberculosis.[15] Interferon gamma release assays, on a blood sample, are recommended in those who are positive to the Mantoux test.[75] These are not affected by immunization or most environmental mycobacteria, so they generate fewer false-positive results.[78] However, they are affected by M. szulgai, M. marinum, and M. kansasii.[79] IGRAs may increase sensitivity when used in addition to the skin test, but may be less sensitive than the skin test when used alone.[80]
The US Preventive Services Task Force (USPSTF) has recommended screening people who are at high risk for latent tuberculosis with either tuberculin skin tests or interferon-gamma release assays.[81] While some have recommend testing health care workers, evidence of benefit for this is poor as of 2019.[82] The Centers for Disease Control and Prevention (CDC) stopped recommending yearly testing of health care workers without known exposure in 2019.[83]
Prevention
Tuberculosis public health campaign in Ireland, c. 1905
Tuberculosis prevention and control efforts rely primarily on the vaccination of infants and the detection and appropriate treatment of active cases.[16] The World Health Organization (WHO) has achieved some success with improved treatment regimens, and a small decrease in case numbers.[16] Some countries have legislation to involuntarily detain or examine those suspected to have tuberculosis, or involuntarily treat them if infected.[84]
Vaccines
The only available vaccine as of 2021 is bacillus Calmette-Guérin (BCG).[85][86] In children it decreases the risk of getting the infection by 20% and the risk of infection turning into active disease by nearly 60%.[87]
It is the most widely used vaccine worldwide, with more than 90% of all children being vaccinated.[16] The immunity it induces decreases after about ten years.[16] As tuberculosis is uncommon in most of Canada, Western Europe, and the United States, BCG is administered to only those people at high risk.[88][89][90] Part of the reasoning against the use of the vaccine is that it makes the tuberculin skin test falsely positive, reducing the test’s usefulness as a screening tool.[90] Several vaccines are being developed.[16]
Intradermal MVA85A vaccine in addition to BCG injection is not effective in preventing tuberculosis.[91]
Public health
Public health campaigns which have focused on overcrowding, public spitting and regular sanitation (including hand washing) during the 1800s helped to either interrupt or slow spread which when combined with contact tracing, isolation and treatment helped to dramatically curb the transmission of both tuberculosis and other airborne diseases which led to the elimination of tuberculosis as a major public health issue in most developed economies.[92][93] Other risk factors which worsened TB spread such as malnutrition were also ameliorated, but since the emergence of HIV a new population of immunocompromised individuals was available for TB to infect.
The World Health Organization (WHO) declared TB a «global health emergency» in 1993,[16] and in 2006, the Stop TB Partnership developed a Global Plan to Stop Tuberculosis that aimed to save 14 million lives between its launch and 2015.[94] A number of targets they set were not achieved by 2015, mostly due to the increase in HIV-associated tuberculosis and the emergence of multiple drug-resistant tuberculosis.[16] A tuberculosis classification system developed by the American Thoracic Society is used primarily in public health programs.[95] In 2015, it launched the End TB Strategy to reduce deaths by 95% and incidence by 90% before 2035. The goal of tuberculosis elimination is hampered by the lack of rapid testing, of short and effective treatment courses, and of completely effective vaccines.[96]
The benefits and risks of giving anti-tubercular drugs in those exposed to MDR-TB is unclear.[97] Making HAART therapy available to HIV-positive individuals significantly reduces the risk of progression to an active TB infection by up to 90% and can mitigate the spread through this population.[98]
Treatment
Tuberculosis phototherapy treatment on 3 March 1934, in Kuopio, Finland
Treatment of TB uses antibiotics to kill the bacteria. Effective TB treatment is difficult, due to the unusual structure and chemical composition of the mycobacterial cell wall, which hinders the entry of drugs and makes many antibiotics ineffective.[99]
Active TB is best treated with combinations of several antibiotics to reduce the risk of the bacteria developing antibiotic resistance.[16] The routine use of rifabutin instead of rifampicin in HIV-positive people with tuberculosis is of unclear benefit as of 2007.[100]
Latent TB
Latent TB is treated with either isoniazid or rifampin alone, or a combination of isoniazid with either rifampicin or rifapentine.[101][102][103]
The treatment takes three to nine months depending on the medications used.[45][101][104][103] People with latent infections are treated to prevent them from progressing to active TB disease later in life.[105]
Education or counselling may improve the latent tuberculosis treatment completion rates.[106]
New onset
The recommended treatment of new-onset pulmonary tuberculosis, as of 2010, is six months of a combination of antibiotics containing rifampicin, isoniazid, pyrazinamide, and ethambutol for the first two months, and only rifampicin and isoniazid for the last four months.[16] Where resistance to isoniazid is high, ethambutol may be added for the last four months as an alternative.[16] Treatment with anti-TB drugs for at least 6 months results in higher success rates when compared with treatment less than 6 months, even though the difference is small. Shorter treatment regimen may be recommended for those with compliance issues.[107] There is also no evidence to support shorter anti-tuberculosis treatment regimens when compared to a 6-month treatment regimen.[108] However recently, results from an international, randomized, controlled clinical trial indicate that a four-month daily treatment regimen containing high-dose, or «optimized», rifapentine with moxifloxacin (2PHZM/2PHM) is as safe and effective as the existing standard six-month daily regimen at curing drug-susceptible tuberculosis (TB) disease.[109]
Recurrent disease
If tuberculosis recurs, testing to determine which antibiotics it is sensitive to is important before determining treatment.[16] If multiple drug-resistant TB (MDR-TB) is detected, treatment with at least four effective antibiotics for 18 to 24 months is recommended.[16]
Medication administration
Directly observed therapy, i.e., having a health care provider watch the person take their medications, is recommended by the World Health Organization (WHO) in an effort to reduce the number of people not appropriately taking antibiotics.[110] The evidence to support this practice over people simply taking their medications independently is of poor quality.[111] There is no strong evidence indicating that directly observed therapy improves the number of people who were cured or the number of people who complete their medicine.[111] Moderate quality evidence suggests that there is also no difference if people are observed at home versus at a clinic, or by a family member versus a health care worker.[111] Methods to remind people of the importance of treatment and appointments may result in a small but important improvement.[112] There is also not enough evidence to support intermittent rifampicin-containing therapy given two to three times a week has equal effectiveness as daily dose regimen on improving cure rates and reducing relapsing rates.[113] There is also not enough evidence on effectiveness of giving intermittent twice or thrice weekly short course regimen compared to daily dosing regimen in treating children with tuberculosis.[114]
Medication resistance
Primary resistance occurs when a person becomes infected with a resistant strain of TB. A person with fully susceptible MTB may develop secondary (acquired) resistance during therapy because of inadequate treatment, not taking the prescribed regimen appropriately (lack of compliance), or using low-quality medication.[115] Drug-resistant TB is a serious public health issue in many developing countries, as its treatment is longer and requires more expensive drugs. MDR-TB is defined as resistance to the two most effective first-line TB drugs: rifampicin and isoniazid. Extensively drug-resistant TB is also resistant to three or more of the six classes of second-line drugs.[116] Totally drug-resistant TB is resistant to all currently used drugs.[117] It was first observed in 2003 in Italy,[118] but not widely reported until 2012,[117][119] and has also been found in Iran and India.[120] There is some efficacy for linezolid to treat those with XDR-TB but side effects and discontinuation of medications were common.[121][122] Bedaquiline is tentatively supported for use in multiple drug-resistant TB.[123]
XDR-TB is a term sometimes used to define extensively resistant TB, and constitutes one in ten cases of MDR-TB. Cases of XDR TB have been identified in more than 90% of countries.[120]
For those with known rifampicin or MDR-TB, molecular tests such as the Genotype MTBDRsl Assay (performed on culture isolates or smear positive specimens) may be useful to detect second-line anti-tubercular drug resistance.[124][125]
Prognosis
Progression from TB infection to overt TB disease occurs when the bacilli overcome the immune system defenses and begin to multiply. In primary TB disease (some 1–5% of cases), this occurs soon after the initial infection.[15] However, in the majority of cases, a latent infection occurs with no obvious symptoms.[15] These dormant bacilli produce active tuberculosis in 5–10% of these latent cases, often many years after infection.[18]
The risk of reactivation increases with immunosuppression, such as that caused by infection with HIV. In people coinfected with M. tuberculosis and HIV, the risk of reactivation increases to 10% per year.[15] Studies using DNA fingerprinting of M. tuberculosis strains have shown reinfection contributes more substantially to recurrent TB than previously thought,[127] with estimates that it might account for more than 50% of reactivated cases in areas where TB is common.[128] The chance of death from a case of tuberculosis is about 4% as of 2008, down from 8% in 1995.[16]
In people with smear-positive pulmonary TB (without HIV co-infection), after 5 years without treatment, 50-60% die while 20-25% achieve spontaneous resolution (cure). TB is almost always fatal in those with untreated HIV co-infection and death rates are increased even with antiretroviral treatment of HIV.[129]
Epidemiology
Roughly one-quarter of the world’s population has been infected with M. tuberculosis,[6] with new infections occurring in about 1% of the population each year.[12] However, most infections with M. tuberculosis do not cause disease,[130] and 90–95% of infections remain asymptomatic.[57] In 2012, an estimated 8.6 million chronic cases were active.[131] In 2010, 8.8 million new cases of tuberculosis were diagnosed, and 1.20–1.45 million deaths occurred (most of these occurring in developing countries).[48][132] Of these, about 0.35 million occur in those also infected with HIV.[133] In 2018, tuberculosis was the leading cause of death worldwide from a single infectious agent.[134] The total number of tuberculosis cases has been decreasing since 2005, while new cases have decreased since 2002.[48]
Tuberculosis[clarification needed] incidence is seasonal, with peaks occurring every spring and summer.[135][136][137][138] The reasons for this are unclear, but may be related to vitamin D deficiency during the winter.[138][139] There are also studies linking tuberculosis to different weather conditions like low temperature, low humidity and low rainfall. It has been suggested that tuberculosis incidence rates may be connected to climate change.[140]
At-risk groups
Tuberculosis is closely linked to both overcrowding and malnutrition, making it one of the principal diseases of poverty.[16] Those at high risk thus include: people who inject illicit drugs, inhabitants and employees of locales where vulnerable people gather (e.g., prisons and homeless shelters), medically underprivileged and resource-poor communities, high-risk ethnic minorities, children in close contact with high-risk category patients, and health-care providers serving these patients.[141]
The rate of tuberculosis varies with age. In Africa, it primarily affects adolescents and young adults.[142] However, in countries where incidence rates have declined dramatically (such as the United States), tuberculosis is mainly a disease of the elderly and immunocompromised (risk factors are listed above).[15][143] Worldwide, 22 «high-burden» states or countries together experience 80% of cases as well as 83% of deaths.[120]
In Canada and Australia, tuberculosis is many times more common among the Indigenous peoples, especially in remote areas.[144][145] Factors contributing to this include higher prevalence of predisposing health conditions and behaviours, and overcrowding and poverty. In some Canadian Indigenous groups, genetic susceptibility may play a role.[47]
Socioeconomic status (SES) strongly affects TB risk. People of low SES are both more likely to contract TB and to be more severely affected by the disease. Those with low SES are more likely to be affected by risk factors for developing TB (e.g., malnutrition, indoor air pollution, HIV co-infection, etc.), and are additionally more likely to be exposed to crowded and poorly ventilated spaces. Inadequate healthcare also means that people with active disease who facilitate spread are not diagnosed and treated promptly; sick people thus remain in the infectious state and (continue to) spread the infection.[47]
Geographical epidemiology
The distribution of tuberculosis is not uniform across the globe; about 80% of the population in many African, Caribbean, South Asian, and eastern European countries test positive in tuberculin tests, while only 5–10% of the U.S. population test positive.[15] Hopes of totally controlling the disease have been dramatically dampened because of many factors, including the difficulty of developing an effective vaccine, the expensive and time-consuming diagnostic process, the necessity of many months of treatment, the increase in HIV-associated tuberculosis, and the emergence of drug-resistant cases in the 1980s.[16]
In developed countries, tuberculosis is less common and is found mainly in urban areas. In Europe, deaths from TB fell from 500 out of 100,000 in 1850 to 50 out of 100,000 by 1950. Improvements in public health were reducing tuberculosis even before the arrival of antibiotics, although the disease remained a significant threat to public health, such that when the Medical Research Council was formed in Britain in 1913 its initial focus was tuberculosis research.[146]
In 2010, rates per 100,000 people in different areas of the world were: globally 178, Africa 332, the Americas 36, Eastern Mediterranean 173, Europe 63, Southeast Asia 278, and Western Pacific 139.[133]
Russia
Russia has achieved particularly dramatic progress with a decline in its TB mortality rate—from 61.9 per 100,000 in 1965 to 2.7 per 100,000 in 1993;[147][148] however, mortality rate increased to 24 per 100,000 in 2005 and then recoiled to 11 per 100,000 by 2015.[149]
China
China has achieved particularly dramatic progress, with about an 80% reduction in its TB mortality rate between 1990 and 2010.[133] The number of new cases has declined by 17% between 2004 and 2014.[120]
Africa
In 2007, the country with the highest estimated incidence rate of TB was Eswatini, with 1,200 cases per 100,000 people. In 2017, the country with the highest estimated incidence rate as a % of the population was Lesotho, with 665 cases per 100,000 people.[150]
India
As of 2017, India had the largest total incidence, with an estimated 2,740,000 cases.[150] According to the World Health Organization (WHO), in 2000–2015, India’s estimated mortality rate dropped from 55 to 36 per 100,000 population per year with estimated 480 thousand people died of TB in 2015.[151][152] In India a major proportion of tuberculosis patients are being treated by private partners and private hospitals. Evidence indicates that the tuberculosis national survey does not represent the number of cases that are diagnosed and recorded by private clinics and hospitals in India.[153]
North America
In the United States, Native Americans have a fivefold greater mortality from TB,[154] and racial and ethnic minorities accounted for 84% of all reported TB cases.[155]
In the United States, the overall tuberculosis case rate was 3 per 100,000 persons in 2017.[150] In Canada, tuberculosis is still endemic in some rural areas.[156]
Western Europe
In 2017, in the United Kingdom, the national average was 9 per 100,000 and the highest incidence rates in Western Europe were 20 per 100,000 in Portugal.
-
Number of new cases of tuberculosis per 100,000 people in 2016[157]
-
Tuberculosis deaths per million persons in 2012
-
Tuberculosis deaths by region, 1990 to 2017[158]
History
Tuberculosis has existed since antiquity.[16] The oldest unambiguously detected M. tuberculosis gives evidence of the disease in the remains of bison in Wyoming dated to around 17,000 years ago.[159] However, whether tuberculosis originated in bovines, then transferred to humans, or whether both bovine and human tuberculosis diverged from a common ancestor, remains unclear.[160] A comparison of the genes of M. tuberculosis complex (MTBC) in humans to MTBC in animals suggests humans did not acquire MTBC from animals during animal domestication, as researchers previously believed. Both strains of the tuberculosis bacteria share a common ancestor, which could have infected humans even before the Neolithic Revolution.[161] Skeletal remains show some prehistoric humans (4000 BC) had TB, and researchers have found tubercular decay in the spines of Egyptian mummies dating from 3000 to 2400 BC.[162] Genetic studies suggest the presence of TB in the Americas from about AD 100.[163]
Before the Industrial Revolution, folklore often associated tuberculosis with vampires. When one member of a family died from the disease, the other infected members would lose their health slowly. People believed this was caused by the original person with TB draining the life from the other family members.[164]
Although Richard Morton established the pulmonary form associated with tubercles as a pathology in 1689,[165][166] due to the variety of its symptoms, TB was not identified as a single disease until the 1820s. Benjamin Marten conjectured in 1720 that consumptions were caused by microbes which were spread by people living close to each other.[167] In 1819, René Laennec claimed that tubercles were the cause of pulmonary tuberculosis.[168] J. L. Schönlein first published the name «tuberculosis» (German: Tuberkulose) in 1832.[169][170] Between 1838 and 1845, John Croghan, the owner of Mammoth Cave in Kentucky from 1839 onwards, brought a number of people with tuberculosis into the cave in the hope of curing the disease with the constant temperature and purity of the cave air; each died within a year.[171] Hermann Brehmer opened the first TB sanatorium in 1859 in Görbersdorf (now Sokołowsko) in Silesia.[172] In 1865, Jean Antoine Villemin demonstrated that tuberculosis could be transmitted, via inoculation, from humans to animals and among animals.[173] (Villemin’s findings were confirmed in 1867 and 1868 by John Burdon-Sanderson.[174])
Robert Koch discovered the tuberculosis bacillus.
Robert Koch identified and described the bacillus causing tuberculosis, M. tuberculosis, on 24 March 1882.[175][176] In 1905, he was awarded the Nobel Prize in Physiology or Medicine for this discovery.[177] Koch did not believe the cattle and human tuberculosis diseases were similar, which delayed the recognition of infected milk as a source of infection. During the first half of the 1900s, the risk of transmission from this source was dramatically reduced after the application of the pasteurization process. Koch announced a glycerine extract of the tubercle bacilli as a «remedy» for tuberculosis in 1890, calling it «tuberculin». Although it was not effective, it was later successfully adapted as a screening test for the presence of pre-symptomatic tuberculosis.[178] World Tuberculosis Day is marked on 24 March each year, the anniversary of Koch’s original scientific announcement.
Albert Calmette and Camille Guérin achieved the first genuine success in immunization against tuberculosis in 1906, using attenuated bovine-strain tuberculosis. It was called bacille Calmette–Guérin (BCG). The BCG vaccine was first used on humans in 1921 in France,[179] but achieved widespread acceptance in the US, Great Britain, and Germany only after World War II.[180]
Tuberculosis caused widespread public concern in the 19th and early 20th centuries as the disease became common among the urban poor. In 1815, one in four deaths in England was due to «consumption». By 1918, TB still caused one in six deaths in France.[citation needed] After TB was determined to be contagious, in the 1880s, it was put on a notifiable-disease list in Britain; campaigns started to stop people from spitting in public places, and the infected poor were «encouraged» to enter sanatoria that resembled prisons (the sanatoria for the middle and upper classes offered excellent care and constant medical attention).[172] Whatever the benefits of the «fresh air» and labor in the sanatoria, even under the best conditions, 50% of those who entered died within five years (c. 1916).[172] When the Medical Research Council formed in Britain in 1913, it initially focused on tuberculosis research.[181]
In Europe, rates of tuberculosis began to rise in the early 1600s to a peak level in the 1800s, when it caused nearly 25% of all deaths.[182] In the 18th and 19th century, tuberculosis had become epidemic in Europe, showing a seasonal pattern.[183][184] By the 1950s mortality in Europe had decreased about 90%.[185] Improvements in sanitation, vaccination, and other public-health measures began significantly reducing rates of tuberculosis even before the arrival of streptomycin and other antibiotics, although the disease remained a significant threat.[185] In 1946, the development of the antibiotic streptomycin made effective treatment and cure of TB a reality. Prior to the introduction of this medication, the only treatment was surgical intervention, including the «pneumothorax technique», which involved collapsing an infected lung to «rest» it and to allow tuberculous lesions to heal.[186]
Because of the emergence of multidrug-resistant tuberculosis (MDR-TB), surgery has been re-introduced for certain cases of TB infections. It involves the removal of infected chest cavities («bullae») in the lungs to reduce the number of bacteria and to increase exposure of the remaining bacteria to antibiotics in the bloodstream.[187] Hopes of eliminating TB ended with the rise of drug-resistant strains in the 1980s. The subsequent resurgence of tuberculosis resulted in the declaration of a global health emergency by the World Health Organization (WHO) in 1993.[188]
Society and culture
Names
Tuberculosis has been known by many names from the technical to the familiar.[189] Phthisis (Φθισις) is a Greek word for consumption, an old term for pulmonary tuberculosis;[8] around 460 BCE, Hippocrates described phthisis as a disease of dry seasons.[190] The abbreviation TB is short for tubercle bacillus. Consumption was the most common nineteenth century English word for the disease, and was also in use well into the twentieth century. The Latin root con meaning ‘completely’ is linked to sumere meaning ‘to take up from under’.[191] In The Life and Death of Mr Badman by John Bunyan, the author calls consumption «the captain of all these men of death.»[192] «Great white plague» has also been used.[189]
Art and literature
Painting The Sick Child by Edvard Munch, 1885–1886, depicts the illness of his sister Sophie, who died of tuberculosis when Edvard was 14; his mother too died of the disease.
Tuberculosis was for centuries associated with poetic and artistic qualities among those infected, and was also known as «the romantic disease».[189][193] Major artistic figures such as the poets John Keats, Percy Bysshe Shelley, and Edgar Allan Poe, the composer Frédéric Chopin,[194] the playwright Anton Chekhov, the novelists Franz Kafka, Katherine Mansfield,[195] Charlotte Brontë, Fyodor Dostoevsky, Thomas Mann, W. Somerset Maugham,[196] George Orwell,[197] and Robert Louis Stevenson, and the artists Alice Neel,[198] Jean-Antoine Watteau, Elizabeth Siddal, Marie Bashkirtseff, Edvard Munch, Aubrey Beardsley and Amedeo Modigliani either had the disease or were surrounded by people who did. A widespread belief was that tuberculosis assisted artistic talent. Physical mechanisms proposed for this effect included the slight fever and toxaemia that it caused, allegedly helping them to see life more clearly and to act decisively.[199][200][201]
Tuberculosis formed an often-reused theme in literature, as in Thomas Mann’s The Magic Mountain, set in a sanatorium;[202] in music, as in Van Morrison’s song «T.B. Sheets»;[203] in opera, as in Puccini’s La bohème and Verdi’s La Traviata;[201] in art, as in Monet’s painting of his first wife Camille on her deathbed;[204] and in film, such as the 1945 The Bells of St. Mary’s starring Ingrid Bergman as a nun with tuberculosis.[205]
Public health efforts
In 2014, the WHO adopted the «End TB» strategy which aims to reduce TB incidence by 80% and TB deaths by 90% by 2030.[206] The strategy contains a milestone to reduce TB incidence by 20% and TB deaths by 35% by 2020.[207] However, by 2020 only a 9% reduction in incidence per population was achieved globally, with the European region achieving 19% and the African region achieving 16% reductions.[207] Similarly, the number of deaths only fell by 14%, missing the 2020 milestone of a 35% reduction, with some regions making better progress (31% reduction in Europe and 19% in Africa).[207] Correspondingly, also treatment, prevention and funding milestones were missed in 2020, for example only 6.3 million people were started on TB prevention short of the target of 30 million.[207]
The World Health Organization (WHO), the Bill and Melinda Gates Foundation, and the U.S. government are subsidizing a fast-acting diagnostic tuberculosis test for use in low- and middle-income countries as of 2012.[208][209][210] In addition to being fast-acting, the test can determine if there is resistance to the antibiotic rifampicin which may indicate multi-drug resistant tuberculosis and is accurate in those who are also infected with HIV.[208][211] Many resource-poor places as of 2011 have access to only sputum microscopy.[212]
India had the highest total number of TB cases worldwide in 2010, in part due to poor disease management within the private and public health care sector.[213] Programs such as the Revised National Tuberculosis Control Program are working to reduce TB levels among people receiving public health care.[214][215]
A 2014 EIU-healthcare report finds there is a need to address apathy and urges for increased funding. The report cites among others Lucica Ditui «[TB] is like an orphan. It has been neglected even in countries with a high burden and often forgotten by donors and those investing in health interventions.»[120]
Slow progress has led to frustration, expressed by the executive director of the Global Fund to Fight AIDS, Tuberculosis and Malaria – Mark Dybul: «we have the tools to end TB as a pandemic and public health threat on the planet, but we are not doing it.»[120] Several international organizations are pushing for more transparency in treatment, and more countries are implementing mandatory reporting of cases to the government as of 2014, although adherence is often variable. Commercial treatment providers may at times overprescribe second-line drugs as well as supplementary treatment, promoting demands for further regulations.[120] The government of Brazil provides universal TB care, which reduces this problem.[120] Conversely, falling rates of TB infection may not relate to the number of programs directed at reducing infection rates but may be tied to an increased level of education, income, and health of the population.[120] Costs of the disease, as calculated by the World Bank in 2009 may exceed US$150 billion per year in «high burden» countries.[120] Lack of progress eradicating the disease may also be due to lack of patient follow-up – as among the 250 million rural migrants in China.[120]
There is insufficient data to show that active contact tracing helps to improve case detection rates for tuberculosis.[216] Interventions such as house-to-house visits, educational leaflets, mass media strategies, educational sessions may increase tuberculosis detection rates in short-term.[217] There is no study that compares new methods of contact tracing such as social network analysis with existing contact tracing methods.[218]
Stigma
Slow progress in preventing the disease may in part be due to stigma associated with TB.[120] Stigma may be due to the fear of transmission from affected individuals. This stigma may additionally arise due to links between TB and poverty, and in Africa, AIDS.[120] Such stigmatization may be both real and perceived; for example, in Ghana, individuals with TB are banned from attending public gatherings.[219]
Stigma towards TB may result in delays in seeking treatment,[120] lower treatment compliance, and family members keeping cause of death secret[219] – allowing the disease to spread further.[120] In contrast, in Russia stigma was associated with increased treatment compliance.[219] TB stigma also affects socially marginalized individuals to a greater degree and varies between regions.[219]
One way to decrease stigma may be through the promotion of «TB clubs», where those infected may share experiences and offer support, or through counseling.[219] Some studies have shown TB education programs to be effective in decreasing stigma, and may thus be effective in increasing treatment adherence.[219] Despite this, studies on the relationship between reduced stigma and mortality are lacking as of 2010, and similar efforts to decrease stigma surrounding AIDS have been minimally effective.[219] Some have claimed the stigma to be worse than the disease, and healthcare providers may unintentionally reinforce stigma, as those with TB are often perceived as difficult or otherwise undesirable.[120] A greater understanding of the social and cultural dimensions of tuberculosis may also help with stigma reduction.[220]
Research
The BCG vaccine has limitations, and research to develop new TB vaccines is ongoing.[221] A number of potential candidates are currently in phase I and II clinical trials.[221][222] Two main approaches are used to attempt to improve the efficacy of available vaccines. One approach involves adding a subunit vaccine to BCG, while the other strategy is attempting to create new and better live vaccines.[221] MVA85A, an example of a subunit vaccine, is in trials in South Africa as of 2006, is based on a genetically modified vaccinia virus.[223] Vaccines are hoped to play a significant role in treatment of both latent and active disease.[224]
To encourage further discovery, researchers and policymakers are promoting new economic models of vaccine development as of 2006, including prizes, tax incentives, and advance market commitments.[225][226] A number of groups, including the Stop TB Partnership,[227] the South African Tuberculosis Vaccine Initiative, and the Aeras Global TB Vaccine Foundation, are involved with research.[228] Among these, the Aeras Global TB Vaccine Foundation received a gift of more than $280 million (US) from the Bill and Melinda Gates Foundation to develop and license an improved vaccine against tuberculosis for use in high burden countries.[229][230]
A number of medications are being studied as of 2012 for multidrug-resistant tuberculosis, including bedaquiline and delamanid.[231] Bedaquiline received U.S. Food and Drug Administration (FDA) approval in late 2012.[232] The safety and effectiveness of these new agents are uncertain as of 2012, because they are based on the results of relatively small studies.[231][233] However, existing data suggest that patients taking bedaquiline in addition to standard TB therapy are five times more likely to die than those without the new drug,[234] which has resulted in medical journal articles raising health policy questions about why the FDA approved the drug and whether financial ties to the company making bedaquiline influenced physicians’ support for its use.[233][235]
Steroids add-on therapy has not shown any benefits for active pulmonary tuberculosis infection.[236]
Other animals
Mycobacteria infect many different animals, including birds,[237] fish, rodents,[238] and reptiles.[239] The subspecies Mycobacterium tuberculosis, though, is rarely present in wild animals.[240] An effort to eradicate bovine tuberculosis caused by Mycobacterium bovis from the cattle and deer herds of New Zealand has been relatively successful.[241] Efforts in Great Britain have been less successful.[242][243]
As of 2015, tuberculosis appears to be widespread among captive elephants in the US. It is believed that the animals originally acquired the disease from humans, a process called reverse zoonosis. Because the disease can spread through the air to infect both humans and other animals, it is a public health concern affecting circuses and zoos.[244][245]
References
- ^ a b c d e f g h i j k l m n o p «Tuberculosis (TB)». who.int. Archived from the original on 30 July 2020. Retrieved 8 May 2020.
- ^ Ferri FF (2010). Ferri’s differential diagnosis : a practical guide to the differential diagnosis of symptoms, signs, and clinical disorders (2nd ed.). Philadelphia, PA: Elsevier/Mosby. p. Chapter T. ISBN 978-0-323-07699-9.
- ^ a b Hawn TR, Day TA, Scriba TJ, Hatherill M, Hanekom WA, Evans TG, et al. (December 2014). «Tuberculosis vaccines and prevention of infection». Microbiology and Molecular Biology Reviews. 78 (4): 650–71. doi:10.1128/MMBR.00021-14. PMC 4248657. PMID 25428938.
- ^ a b c Implementing the WHO Stop TB Strategy: a handbook for national TB control programmes. Geneva: World Health Organization (WHO). 2008. p. 179. ISBN 978-92-4-154667-6. Archived from the original on 2 June 2021. Retrieved 17 September 2017.
- ^ a b Harris RE (2013). «Epidemiology of Tuberculosis». Epidemiology of chronic disease: global perspectives. Burlington, MA: Jones & Bartlett Learning. p. 682. ISBN 978-0-7637-8047-0.
- ^ a b c «Tuberculosis (TB)». World Health Organization (WHO). 16 February 2018. Archived from the original on 30 December 2013. Retrieved 15 September 2018.
- ^ «Tuberculosis deaths rise for the first time in more than a decade due to the COVID-19 pandemic». www.who.int. Archived from the original on 16 October 2021. Retrieved 16 October 2021.
- ^ a b The Chambers Dictionary. New Delhi: Allied Chambers India Ltd. 1998. p. 352. ISBN 978-81-86062-25-8. Archived from the original on 6 September 2015.
- ^ a b c d e f g h i Adkinson NF, Bennett JE, Douglas RG, Mandell GL (2010). Mandell, Douglas, and Bennett’s principles and practice of infectious diseases (7th ed.). Philadelphia, PA: Churchill Livingstone/Elsevier. p. Chapter 250. ISBN 978-0-443-06839-3.
- ^ «Basic TB Facts». Centers for Disease Control and Prevention (CDC). 13 March 2012. Archived from the original on 6 February 2016. Retrieved 11 February 2016.
- ^ a b Konstantinos A (2010). «Testing for tuberculosis». Australian Prescriber. 33 (1): 12–18. doi:10.18773/austprescr.2010.005.
- ^ a b «Tuberculosis». World Health Organization (WHO). 2002. Archived from the original on 17 June 2013.
- ^ a b «Tuberculosis (TB)». WHO. Archived from the original on 30 July 2020. Retrieved 16 October 2021.
- ^ «Global tuberculosis report». World Health Organization (WHO). Archived from the original on 30 December 2013. Retrieved 9 November 2017.
- ^ a b c d e f g h i j k l m n o Kumar V, Robbins SL (2007). Robbins Basic Pathology (8th ed.). Philadelphia: Elsevier. ISBN 978-1-4160-2973-1. OCLC 69672074.
- ^ a b c d e f g h i j k l m n o p q r s t u v Lawn SD, Zumla AI (July 2011). «Tuberculosis». Lancet. 378 (9785): 57–72. doi:10.1016/S0140-6736(10)62173-3. PMID 21420161. S2CID 208791546. Archived from the original on 27 August 2021. Retrieved 31 January 2020.
- ^ Schiffman G (15 January 2009). «Tuberculosis Symptoms». eMedicine Health. Archived from the original on 16 May 2009.
- ^ a b c d Gibson PG, Abramson M, Wood-Baker R, Volmink J, Hensley M, Costabel U, eds. (2005). Evidence-Based Respiratory Medicine (1st ed.). BMJ Books. p. 321. ISBN 978-0-7279-1605-1. Archived from the original on 8 December 2015.
- ^ Behera D (2010). Textbook of Pulmonary Medicine (2nd ed.). New Delhi: Jaypee Brothers Medical Publishers. p. 457. ISBN 978-81-8448-749-7. Archived from the original on 6 September 2015.
- ^ Halezeroğlu S, Okur E (March 2014). «Thoracic surgery for haemoptysis in the context of tuberculosis: what is the best management approach?». Journal of Thoracic Disease. 6 (3): 182–85. doi:10.3978/j.issn.2072-1439.2013.12.25. PMC 3949181. PMID 24624281.
- ^ Jindal SK, ed. (2011). Textbook of Pulmonary and Critical Care Medicine. New Delhi: Jaypee Brothers Medical Publishers. p. 549. ISBN 978-93-5025-073-0. Archived from the original on 7 September 2015.
- ^ a b Habermann TM, Ghosh A (2008). Mayo Clinic internal medicine: concise textbook. Rochester, MN: Mayo Clinic Scientific Press. p. 789. ISBN 978-1-4200-6749-1. Archived from the original on 6 September 2015.
- ^ Southwick F (2007). «Chapter 4: Pulmonary Infections». Infectious Diseases: A Clinical Short Course, 2nd ed. McGraw-Hill Medical Publishing Division. pp. 104, 313–14. ISBN 978-0-07-147722-2.
- ^ Jindal SK (2011). Textbook of Pulmonary and Critical Care Medicine. New Delhi: Jaypee Brothers Medical Publishers. p. 525. ISBN 978-93-5025-073-0. Archived from the original on 6 September 2015.
- ^ Niederweis M, Danilchanka O, Huff J, Hoffmann C, Engelhardt H (March 2010). «Mycobacterial outer membranes: in search of proteins». Trends in Microbiology. 18 (3): 109–16. doi:10.1016/j.tim.2009.12.005. PMC 2931330. PMID 20060722.
- ^ a b Madison BM (May 2001). «Application of stains in clinical microbiology». Biotechnic & Histochemistry. 76 (3): 119–25. doi:10.1080/714028138. PMID 11475314.
- ^ Parish T, Stoker NG (December 1999). «Mycobacteria: bugs and bugbears (two steps forward and one step back)». Molecular Biotechnology. 13 (3): 191–200. doi:10.1385/MB:13:3:191. PMID 10934532. S2CID 28960959.
- ^ Medical Laboratory Science: Theory and Practice. New Delhi: Tata McGraw-Hill. 2000. p. 473. ISBN 978-0-07-463223-9. Archived from the original on 6 September 2015.
- ^ «Acid-Fast Stain Protocols». 21 August 2013. Archived from the original on 1 October 2011. Retrieved 26 March 2016.
- ^ Kommareddi S, Abramowsky CR, Swinehart GL, Hrabak L (November 1984). «Nontuberculous mycobacterial infections: comparison of the fluorescent auramine-O and Ziehl-Neelsen techniques in tissue diagnosis». Human Pathology. 15 (11): 1085–9. doi:10.1016/S0046-8177(84)80253-1. PMID 6208117.
- ^ van Lettow M, Whalen C (2008). Semba RD, Bloem MW (eds.). Nutrition and health in developing countries (2nd ed.). Totowa, N.J.: Humana Press. p. 291. ISBN 978-1-934115-24-4. Archived from the original on 6 September 2015.
- ^ van Soolingen D, Hoogenboezem T, de Haas PE, Hermans PW, Koedam MA, Teppema KS, et al. (October 1997). «A novel pathogenic taxon of the Mycobacterium tuberculosis complex, Canetti: characterization of an exceptional isolate from Africa». International Journal of Systematic Bacteriology. 47 (4): 1236–45. doi:10.1099/00207713-47-4-1236. PMID 9336935.
- ^ Niemann S, Rüsch-Gerdes S, Joloba ML, Whalen CC, Guwatudde D, Ellner JJ, et al. (September 2002). «Mycobacterium africanum subtype II is associated with two distinct genotypes and is a major cause of human tuberculosis in Kampala, Uganda». Journal of Clinical Microbiology. 40 (9): 3398–405. doi:10.1128/JCM.40.9.3398-3405.2002. PMC 130701. PMID 12202584.
- ^ Niobe-Eyangoh SN, Kuaban C, Sorlin P, Cunin P, Thonnon J, Sola C, et al. (June 2003). «Genetic biodiversity of Mycobacterium tuberculosis complex strains from patients with pulmonary tuberculosis in Cameroon». Journal of Clinical Microbiology. 41 (6): 2547–53. doi:10.1128/JCM.41.6.2547-2553.2003. PMC 156567. PMID 12791879.
- ^ Thoen C, Lobue P, de Kantor I (February 2006). «The importance of Mycobacterium bovis as a zoonosis». Veterinary Microbiology. 112 (2–4): 339–45. doi:10.1016/j.vetmic.2005.11.047. PMID 16387455.
- ^ Acton QA (2011). Mycobacterium Infections: New Insights for the Healthcare Professional. ScholarlyEditions. p. 1968. ISBN 978-1-4649-0122-5. Archived from the original on 6 September 2015.
- ^ Pfyffer GE, Auckenthaler R, van Embden JD, van Soolingen D (1998). «Mycobacterium canettii, the smooth variant of M. tuberculosis, isolated from a Swiss patient exposed in Africa». Emerging Infectious Diseases. 4 (4): 631–4. doi:10.3201/eid0404.980414. PMC 2640258. PMID 9866740.
- ^ Panteix G, Gutierrez MC, Boschiroli ML, Rouviere M, Plaidy A, Pressac D, et al. (August 2010). «Pulmonary tuberculosis due to Mycobacterium microti: a study of six recent cases in France». Journal of Medical Microbiology. 59 (Pt 8): 984–989. doi:10.1099/jmm.0.019372-0. PMID 20488936.
- ^ American Thoracic Society (August 1997). «Diagnosis and treatment of disease caused by nontuberculous mycobacteria. This official statement of the American Thoracic Society was approved by the Board of Directors, March 1997. Medical Section of the American Lung Association». American Journal of Respiratory and Critical Care Medicine. 156 (2 Pt 2): S1–25. doi:10.1164/ajrccm.156.2.atsstatement. PMID 9279284.
- ^ Cole EC, Cook CE (August 1998). «Characterization of infectious aerosols in health care facilities: an aid to effective engineering controls and preventive strategies». American Journal of Infection Control. 26 (4): 453–64. doi:10.1016/S0196-6553(98)70046-X. PMC 7132666. PMID 9721404.
- ^ Nicas M, Nazaroff WW, Hubbard A (March 2005). «Toward understanding the risk of secondary airborne infection: emission of respirable pathogens». Journal of Occupational and Environmental Hygiene. 2 (3): 143–54. doi:10.1080/15459620590918466. PMC 7196697. PMID 15764538.
- ^ a b Ahmed N, Hasnain SE (September 2011). «Molecular epidemiology of tuberculosis in India: moving forward with a systems biology approach». Tuberculosis. 91 (5): 407–13. doi:10.1016/j.tube.2011.03.006. PMID 21514230.
- ^ a b «Tuberculosis Fact sheet N°104». World Health Organization (WHO). November 2010. Archived from the original on 4 October 2006. Retrieved 26 July 2011.
- ^ a b «Core Curriculum on Tuberculosis: What the Clinician Should Know» (PDF) (5th ed.). Centers for Disease Control and Prevention (CDC), Division of Tuberculosis Elimination. 2011. p. 24. Archived (PDF) from the original on 19 May 2012.
- ^ «Causes of Tuberculosis». Mayo Clinic. 21 December 2006. Archived from the original on 18 October 2007. Retrieved 19 October 2007.
- ^ a b c d e Narasimhan P, Wood J, Macintyre CR, Mathai D (2013). «Risk factors for tuberculosis». Pulmonary Medicine. 2013: 828939. doi:10.1155/2013/828939. PMC 3583136. PMID 23476764.
- ^ a b c «The sixteenth global report on tuberculosis» (PDF). World Health Organization (WHO). 2011. Archived from the original (PDF) on 6 September 2012.
- ^ «Global tuberculosis control–surveillance, planning, financing WHO Report 2006». World Health Organization (WHO). Archived from the original on 12 December 2006. Retrieved 13 October 2006.
- ^ Chaisson RE, Martinson NA (March 2008). «Tuberculosis in Africa – combating an HIV-driven crisis». The New England Journal of Medicine. 358 (11): 1089–92. doi:10.1056/NEJMp0800809. PMID 18337598.
- ^ Restrepo BI (August 2007). «Convergence of the tuberculosis and diabetes epidemics: renewal of old acquaintances». Clinical Infectious Diseases. 45 (4): 436–38. doi:10.1086/519939. PMC 2900315. PMID 17638190.
- ^ «Targeted tuberculin testing and treatment of latent tuberculosis infection. American Thoracic Society». MMWR. Recommendations and Reports. 49 (RR-6): 1–51. June 2000. PMID 10881762. Archived from the original on 17 December 2004.
- ^ van Zyl Smit RN, Pai M, Yew WW, Leung CC, Zumla A, Bateman ED, et al. (January 2010). «Global lung health: the colliding epidemics of tuberculosis, tobacco smoking, HIV and COPD». The European Respiratory Journal. 35 (1): 27–33. doi:10.1183/09031936.00072909. PMC 5454527. PMID 20044459.
These analyses indicate that smokers are almost twice as likely to be infected with TB and to progress to active disease (RR of about 1.5 for latent TB infection (LTBI) and RR of ∼2.0 for TB disease). Smokers are also twice as likely to die from TB (RR of about 2.0 for TB mortality), but data are difficult to interpret because of heterogeneity in the results across studies.
- ^ «TB Risk Factors | Basic TB Facts | TB | CDC». cdc.gov. 26 May 2020. Archived from the original on 30 August 2020. Retrieved 25 August 2020.
- ^ Möller M, Hoal EG (March 2010). «Current findings, challenges and novel approaches in human genetic susceptibility to tuberculosis». Tuberculosis. 90 (2): 71–83. doi:10.1016/j.tube.2010.02.002. PMID 20206579.
- ^ Good JM, Cooper S, Doane AS (1835). The Study of Medicine. Harper. p. 32. Archived from the original on 10 August 2016.
- ^ a b Skolnik R (2011). Global health 101 (2nd ed.). Burlington, MA: Jones & Bartlett Learning. p. 253. ISBN 978-0-7637-9751-5.
- ^ a b Mainous III AR, Pomeroy C (2009). Management of antimicrobials in infectious diseases: impact of antibiotic resistance (2nd rev. ed.). Totowa, NJ: Humana Press. p. 74. ISBN 978-1-60327-238-4. Archived from the original on 6 September 2015.
- ^ Houben EN, Nguyen L, Pieters J (February 2006). «Interaction of pathogenic mycobacteria with the host immune system». Current Opinion in Microbiology. 9 (1): 76–85. doi:10.1016/j.mib.2005.12.014. PMID 16406837.
- ^ Queval CJ, Brosch R, Simeone R (2017). «Mycobacterium tuberculosis». Frontiers in Microbiology. 8: 2284. doi:10.3389/fmicb.2017.02284. PMC 5703847. PMID 29218036.
- ^ Khan MR (2011). Essence of Paediatrics. Elsevier India. p. 401. ISBN 978-81-312-2804-3. Archived from the original on 6 September 2015.
- ^ Herrmann JL, Lagrange PH (February 2005). «Dendritic cells and Mycobacterium tuberculosis: which is the Trojan horse?». Pathologie-Biologie. 53 (1): 35–40. doi:10.1016/j.patbio.2004.01.004. PMID 15620608.
- ^ Agarwal R, Malhotra P, Awasthi A, Kakkar N, Gupta D (April 2005). «Tuberculous dilated cardiomyopathy: an under-recognized entity?». BMC Infectious Diseases. 5 (1): 29. doi:10.1186/1471-2334-5-29. PMC 1090580. PMID 15857515.
- ^ a b c d Grosset J (March 2003). «Mycobacterium tuberculosis in the extracellular compartment: an underestimated adversary». Antimicrobial Agents and Chemotherapy. 47 (3): 833–36. doi:10.1128/AAC.47.3.833-836.2003. PMC 149338. PMID 12604509.
- ^ Bozzano F, Marras F, De Maria A (2014). «Immunology of tuberculosis». Mediterranean Journal of Hematology and Infectious Diseases. 6 (1): e2014027. doi:10.4084/MJHID.2014.027. PMC 4010607. PMID 24804000.
- ^ Crowley LV (2010). An introduction to human disease: pathology and pathophysiology correlations (8th ed.). Sudbury, MA: Jones and Bartlett. p. 374. ISBN 978-0-7637-6591-0. Archived from the original on 6 September 2015.
- ^ Anthony H (2005). TB/HIV a Clinical Manual (2nd ed.). Geneva: World Health Organization (WHO). p. 75. ISBN 978-92-4-154634-8. Archived from the original on 6 September 2015.
- ^ Jacob JT, Mehta AK, Leonard MK (January 2009). «Acute forms of tuberculosis in adults». The American Journal of Medicine. 122 (1): 12–17. doi:10.1016/j.amjmed.2008.09.018. PMID 19114163.
- ^ a b Bento J, Silva AS, Rodrigues F, Duarte R (2011). «[Diagnostic tools in tuberculosis]». Acta Médica Portuguesa. 24 (1): 145–54. doi:10.20344/amp.333. PMID 21672452. S2CID 76156550.
- ^ a b c d Escalante P (June 2009). «In the clinic. Tuberculosis». Annals of Internal Medicine. 150 (11): ITC61-614, quiz ITV616. doi:10.7326/0003-4819-150-11-200906020-01006. PMID 19487708. S2CID 639982. Archived from the original on 27 August 2021. Retrieved 31 January 2020.
- ^ Metcalfe JZ, Everett CK, Steingart KR, Cattamanchi A, Huang L, Hopewell PC, Pai M (November 2011). «Interferon-γ release assays for active pulmonary tuberculosis diagnosis in adults in low- and middle-income countries: systematic review and meta-analysis». The Journal of Infectious Diseases. 204 Suppl 4 (suppl_4): S1120-9. doi:10.1093/infdis/jir410. PMC 3192542. PMID 21996694.
- ^ a b Sester M, Sotgiu G, Lange C, Giehl C, Girardi E, Migliori GB, et al. (January 2011). «Interferon-γ release assays for the diagnosis of active tuberculosis: a systematic review and meta-analysis». The European Respiratory Journal. 37 (1): 100–11. doi:10.1183/09031936.00114810. PMID 20847080.
- ^ Chen J, Zhang R, Wang J, Liu L, Zheng Y, Shen Y, et al. (2011). Vermund SH (ed.). «Interferon-gamma release assays for the diagnosis of active tuberculosis in HIV-infected patients: a systematic review and meta-analysis». PLOS ONE. 6 (11): e26827. Bibcode:2011PLoSO…626827C. doi:10.1371/journal.pone.0026827. PMC 3206065. PMID 22069472.
- ^ Special Programme for Research & Training in Tropical Diseases (2006). Diagnostics for tuberculosis: global demand and market potential. Geneva: World Health Organization (WHO). p. 36. ISBN 978-92-4-156330-7. Archived from the original on 6 September 2015.
- ^ a b National Institute for Health and Clinical Excellence. Clinical guideline 117: Tuberculosis. London, 2011.
- ^ Steingart KR, Flores LL, Dendukuri N, Schiller I, Laal S, Ramsay A, et al. (August 2011). Evans C (ed.). «Commercial serological tests for the diagnosis of active pulmonary and extrapulmonary tuberculosis: an updated systematic review and meta-analysis». PLOS Medicine. 8 (8): e1001062. doi:10.1371/journal.pmed.1001062. PMC 3153457. PMID 21857806.
- ^ Rothel JS, Andersen P (December 2005). «Diagnosis of latent Mycobacterium tuberculosis infection: is the demise of the Mantoux test imminent?». Expert Review of Anti-Infective Therapy. 3 (6): 981–93. doi:10.1586/14787210.3.6.981. PMID 16307510. S2CID 25423684.
- ^ Pai M, Zwerling A, Menzies D (August 2008). «Systematic review: T-cell-based assays for the diagnosis of latent tuberculosis infection: an update». Annals of Internal Medicine. 149 (3): 177–84. doi:10.7326/0003-4819-149-3-200808050-00241. PMC 2951987. PMID 18593687.
- ^ Jindal SK, ed. (2011). Textbook of Pulmonary and Critical Care Medicine. New Delhi: Jaypee Brothers Medical Publishers. p. 544. ISBN 978-93-5025-073-0. Archived from the original on 6 September 2015.
- ^ Amicosante M, Ciccozzi M, Markova R (April 2010). «Rational use of immunodiagnostic tools for tuberculosis infection: guidelines and cost effectiveness studies». The New Microbiologica. 33 (2): 93–107. PMID 20518271.
- ^ Bibbins-Domingo K, Grossman DC, Curry SJ, Bauman L, Davidson KW, Epling JW, et al. (September 2016). «Screening for Latent Tuberculosis Infection in Adults: US Preventive Services Task Force Recommendation Statement». JAMA. 316 (9): 962–9. doi:10.1001/jama.2016.11046. PMID 27599331.
- ^ Gill J, Prasad V (November 2019). «Testing Healthcare Workers for Latent Tuberculosis: Is It Evidence Based, Bio-Plausible, Both, Or Neither?». The American Journal of Medicine. 132 (11): 1260–1261. doi:10.1016/j.amjmed.2019.03.017. PMID 30946831.
- ^ Sosa LE, Njie GJ, Lobato MN, Bamrah Morris S, Buchta W, Casey ML, et al. (May 2019). «Tuberculosis Screening, Testing, and Treatment of U.S. Health Care Personnel: Recommendations from the National Tuberculosis Controllers Association and CDC, 2019». MMWR. Morbidity and Mortality Weekly Report. 68 (19): 439–443. doi:10.15585/mmwr.mm6819a3. PMC 6522077. PMID 31099768.
- ^ Coker, Richard; Thomas, Marianna; Lock, Karen; Martin, Robyn (2007). «Detention and the Evolving Threat of Tuberculosis: Evidence, Ethics, and Law». Journal of Law, Medicine & Ethics. 35 (4): 609–615. doi:10.1111/j.1748-720X.2007.00184.x. ISSN 1073-1105. PMID 18076512. S2CID 19924571.
- ^ McShane H (October 2011). «Tuberculosis vaccines: beyond bacille Calmette-Guerin». Philosophical Transactions of the Royal Society of London. Series B, Biological Sciences. 366 (1579): 2782–89. doi:10.1098/rstb.2011.0097. PMC 3146779. PMID 21893541.
- ^ «Vaccines | Basic TB Facts | TB | CDC». cdc.gov. CDC. 16 June 2021. Retrieved 30 December 2021.
- ^ Roy A, Eisenhut M, Harris RJ, Rodrigues LC, Sridhar S, Habermann S, et al. (August 2014). «Effect of BCG vaccination against Mycobacterium tuberculosis infection in children: systematic review and meta-analysis». BMJ. 349: g4643. doi:10.1136/bmj.g4643. PMC 4122754. PMID 25097193.
- ^ «Vaccine and Immunizations: TB Vaccine (BCG)». Centers for Disease Control and Prevention. 2011. Archived from the original on 17 November 2011. Retrieved 26 July 2011.
- ^ «BCG Vaccine Usage in Canada – Current and Historical». Public Health Agency of Canada. September 2010. Archived from the original on 30 March 2012. Retrieved 30 December 2011.
- ^ a b Teo SS, Shingadia DV (June 2006). «Does BCG have a role in tuberculosis control and prevention in the United Kingdom?». Archives of Disease in Childhood. 91 (6): 529–31. doi:10.1136/adc.2005.085043. PMC 2082765. PMID 16714729.
- ^ Kashangura R, Jullien S, Garner P, Johnson S, et al. (Cochrane Infectious Diseases Group) (April 2019). «MVA85A vaccine to enhance BCG for preventing tuberculosis». The Cochrane Database of Systematic Reviews. 2019 (4): CD012915. doi:10.1002/14651858.CD012915.pub2. PMC 6488980. PMID 31038197.
- ^ Clark M, Riben P, Nowgesic E (October 2002). «The association of housing density, isolation and tuberculosis in Canadian First Nations communities». International Journal of Epidemiology. 31 (5): 940–945. doi:10.1093/ije/31.5.940. PMID 12435764.
- ^ Barberis I, Bragazzi NL, Galluzzo L, Martini M (March 2017). «The history of tuberculosis: from the first historical records to the isolation of Koch’s bacillus». Journal of Preventive Medicine and Hygiene. 58 (1): E9–E12. PMC 5432783. PMID 28515626.
- ^ «The Global Plan to Stop TB». World Health Organization (WHO). 2011. Archived from the original on 12 June 2011. Retrieved 13 June 2011.
- ^ Warrell DA, Cox TM, Firth JD, Benz EJ (2005). Sections 1–10 (4. ed., paperback ed.). Oxford [u.a.]: Oxford Univ. Press. p. 560. ISBN 978-0-19-857014-1. Archived from the original on 6 September 2015.
- ^ Uplekar M, Weil D, Lonnroth K, Jaramillo E, Lienhardt C, Dias HM, et al. (May 2015). «WHO’s new end TB strategy». Lancet. 385 (9979): 1799–1801. doi:10.1016/S0140-6736(15)60570-0. PMID 25814376. S2CID 39379915.
- ^ Fraser A, Paul M, Attamna A, Leibovici L, et al. (Cochrane Infectious Diseases Group) (April 2006). «Drugs for preventing tuberculosis in people at risk of multiple-drug-resistant pulmonary tuberculosis». The Cochrane Database of Systematic Reviews. 2006 (2): CD005435. doi:10.1002/14651858.CD005435.pub2. PMC 6532726. PMID 16625639.
- ^ Piggott DA, Karakousis PC (27 December 2010). «Timing of antiretroviral therapy for HIV in the setting of TB treatment». Clinical & Developmental Immunology. 2011: 103917. doi:10.1155/2011/103917. PMC 3017895. PMID 21234380.
- ^ Brennan PJ, Nikaido H (1995). «The envelope of mycobacteria». Annual Review of Biochemistry. 64: 29–63. doi:10.1146/annurev.bi.64.070195.000333. PMID 7574484.
- ^ Davies G, Cerri S, Richeldi L (October 2007). «Rifabutin for treating pulmonary tuberculosis». The Cochrane Database of Systematic Reviews. 2007 (4): CD005159. doi:10.1002/14651858.CD005159.pub2. PMC 6532710. PMID 17943842.
- ^ a b Latent tuberculosis infection. World Health Organization (WHO). 2018. p. 23. ISBN 978-92-4-155023-9. Archived from the original on 2 June 2021. Retrieved 25 July 2018.
- ^ Borisov AS, Bamrah Morris S, Njie GJ, Winston CA, Burton D, Goldberg S, et al. (June 2018). «Update of Recommendations for Use of Once-Weekly Isoniazid-Rifapentine Regimen to Treat Latent Mycobacterium tuberculosis Infection». MMWR. Morbidity and Mortality Weekly Report. 67 (25): 723–726. doi:10.15585/mmwr.mm6725a5. PMC 6023184. PMID 29953429.
- ^ a b Sterling TR, Njie G, Zenner D, Cohn DL, Reves R, Ahmed A, et al. (February 2020). «Guidelines for the Treatment of Latent Tuberculosis Infection: Recommendations from the National Tuberculosis Controllers Association and CDC, 2020». MMWR. Recommendations and Reports. 69 (1): 1–11. doi:10.15585/mmwr.rr6901a1. PMC 7041302. PMID 32053584.
- ^ Njie GJ, Morris SB, Woodruff RY, Moro RN, Vernon AA, Borisov AS (August 2018). «Isoniazid-Rifapentine for Latent Tuberculosis Infection: A Systematic Review and Meta-analysis». American Journal of Preventive Medicine. 55 (2): 244–252. doi:10.1016/j.amepre.2018.04.030. PMC 6097523. PMID 29910114.
- ^ Menzies D, Al Jahdali H, Al Otaibi B (March 2011). «Recent developments in treatment of latent tuberculosis infection». The Indian Journal of Medical Research. 133 (3): 257–66. PMC 3103149. PMID 21441678.
- ^ M’imunya JM, Kredo T, Volmink J, et al. (Cochrane Infectious Diseases Group) (May 2012). «Patient education and counselling for promoting adherence to treatment for tuberculosis». The Cochrane Database of Systematic Reviews. 2012 (5): CD006591. doi:10.1002/14651858.CD006591.pub2. PMC 6532681. PMID 22592714.
- ^ Gelband H, et al. (Cochrane Infectious Diseases Group) (25 October 1999). «Regimens of less than six months for treating tuberculosis». The Cochrane Database of Systematic Reviews. 1999 (2): CD001362. doi:10.1002/14651858.CD001362. PMC 6532732. PMID 10796641.
- ^ Grace AG, Mittal A, Jain S, Tripathy JP, Satyanarayana S, Tharyan P, Kirubakaran R, et al. (Cochrane Infectious Diseases Group) (December 2019). «Shortened treatment regimens versus the standard regimen for drug-sensitive pulmonary tuberculosis». The Cochrane Database of Systematic Reviews. 12 (12): CD012918. doi:10.1002/14651858.CD012918.pub2. PMC 6953336. PMID 31828771.
- ^ «Landmark TB Trial Identifies Shorter-Course Treatment Regimen». CDC. NCHHSTP Media Team Centers for Disease Control and Prevention. 20 October 2020. Retrieved 27 November 2021.
- ^ Mainous III AB (2010). Management of Antimicrobials in Infectious Diseases: Impact of Antibiotic Resistance. Totowa, NJ: Humana Press. p. 69. ISBN 978-1-60327-238-4. Archived from the original on 6 September 2015.
- ^ a b c Karumbi J, Garner P (May 2015). «Directly observed therapy for treating tuberculosis». The Cochrane Database of Systematic Reviews. 2015 (5): CD003343. doi:10.1002/14651858.CD003343.pub4. PMC 4460720. PMID 26022367.
- ^ Liu Q, Abba K, Alejandria MM, Sinclair D, Balanag VM, Lansang MA, et al. (Cochrane Infectious Diseases Group) (November 2014). «Reminder systems to improve patient adherence to tuberculosis clinic appointments for diagnosis and treatment». The Cochrane Database of Systematic Reviews. 2014 (11): CD006594. doi:10.1002/14651858.CD006594.pub3. PMC 4448217. PMID 25403701.
- ^ Mwandumba HC, Squire SB, et al. (Cochrane Infectious Diseases Group) (23 October 2001). «Fully intermittent dosing with drugs for treating tuberculosis in adults». The Cochrane Database of Systematic Reviews (4): CD000970. doi:10.1002/14651858.CD000970. PMC 6532565. PMID 11687088.
- ^ Bose A, Kalita S, Rose W, Tharyan P, et al. (Cochrane Infectious Diseases Group) (January 2014). «Intermittent versus daily therapy for treating tuberculosis in children». The Cochrane Database of Systematic Reviews. 2014 (1): CD007953. doi:10.1002/14651858.CD007953.pub2. PMC 6532685. PMID 24470141.
- ^ O’Brien RJ (June 1994). «Drug-resistant tuberculosis: etiology, management and prevention». Seminars in Respiratory Infections. 9 (2): 104–12. PMID 7973169.
- ^ Centers for Disease Control and Prevention (CDC) (March 2006). «Emergence of Mycobacterium tuberculosis with extensive resistance to second-line drugs—worldwide, 2000-2004». MMWR. Morbidity and Mortality Weekly Report. 55 (11): 301–5. PMID 16557213. Archived from the original on 22 May 2017.
- ^ a b McKenna M (12 January 2012). «Totally Resistant TB: Earliest Cases in Italy». Wired. Archived from the original on 14 January 2012. Retrieved 12 January 2012.
- ^ Migliori GB, De Iaco G, Besozzi G, Centis R, Cirillo DM (May 2007). «First tuberculosis cases in Italy resistant to all tested drugs». Euro Surveillance. 12 (5): E070517.1. doi:10.2807/esw.12.20.03194-en. PMID 17868596.
- ^ «Totally Drug-Resistant TB: a WHO consultation on the diagnostic definition and treatment options» (PDF). World Health Organization (WHO). Archived (PDF) from the original on 21 October 2016. Retrieved 25 March 2016.
- ^ a b c d e f g h i j k l m n o p Kielstra P (30 June 2014). Tabary Z (ed.). «Ancient enemy, modern imperative – A time for greater action against tuberculosis» (PDF). The Economist. Economist Intelligence Unit. Archived from the original (PDF) on 31 July 2014. Retrieved 22 January 2022.
- ^ Singh B, Cocker D, Ryan H, Sloan DJ, et al. (Cochrane Infectious Diseases Group) (March 2019). «Linezolid for drug-resistant pulmonary tuberculosis». The Cochrane Database of Systematic Reviews. 3 (3): CD012836. doi:10.1002/14651858.CD012836.pub2. PMC 6426281. PMID 30893466.
- ^ Velayati AA, Masjedi MR, Farnia P, Tabarsi P, Ghanavi J, ZiaZarifi AH, Hoffner SE (August 2009). «Emergence of new forms of totally drug-resistant tuberculosis bacilli: super extensively drug-resistant tuberculosis or totally drug-resistant strains in Iran». Chest. 136 (2): 420–425. doi:10.1378/chest.08-2427. PMID 19349380.
- ^ «Provisional CDC Guidelines for the Use and Safety Monitoring of Bedaquiline Fumarate (Sirturo) for the Treatment of Multidrug-Resistant Tuberculosis». Archived from the original on 4 January 2014.
- ^ Theron G, Peter J, Richardson M, Warren R, Dheda K, Steingart KR, et al. (Cochrane Infectious Diseases Group) (September 2016). «® MTBDRsl assay for resistance to second-line anti-tuberculosis drugs». The Cochrane Database of Systematic Reviews. 2016 (9): CD010705. doi:10.1002/14651858.CD010705.pub3. PMC 5034505. PMID 27605387.
- ^ «The use of molecular line probe assays for the detection of resistance to second-line anti-tuberculosis drugs» (PDF). World Health Organization. Archived (PDF) from the original on 22 September 2021. Retrieved 18 June 2021.
- ^ «WHO Disease and injury country estimates». World Health Organization (WHO). 2004. Archived from the original on 11 November 2009. Retrieved 11 November 2009.
- ^ Lambert ML, Hasker E, Van Deun A, Roberfroid D, Boelaert M, Van der Stuyft P (May 2003). «Recurrence in tuberculosis: relapse or reinfection?». The Lancet. Infectious Diseases. 3 (5): 282–7. doi:10.1016/S1473-3099(03)00607-8. PMID 12726976.
- ^ Wang JY, Lee LN, Lai HC, Hsu HL, Liaw YS, Hsueh PR, Yang PC (July 2007). «Prediction of the tuberculosis reinfection proportion from the local incidence». The Journal of Infectious Diseases. 196 (2): 281–8. doi:10.1086/518898. PMID 17570116.
- ^ «1.4 Prognosis — Tuberculosis». medicalguidelines.msf.org. Archived from the original on 2 June 2021. Retrieved 25 August 2020.
- ^ «Fact Sheets: The Difference Between Latent TB Infection and Active TB Disease». Centers for Disease Control and Prevention (CDC). 20 June 2011. Archived from the original on 4 August 2011. Retrieved 26 July 2011.
- ^ «Global tuberculosis report 2013». World Health Organization (WHO). 2013. Archived from the original on 12 December 2006.
- ^ Lozano R, Naghavi M, Foreman K, Lim S, Shibuya K, Aboyans V, et al. (December 2012). «Global and regional mortality from 235 causes of death for 20 age groups in 1990 and 2010: a systematic analysis for the Global Burden of Disease Study 2010». Lancet. 380 (9859): 2095–128. doi:10.1016/S0140-6736(12)61728-0. hdl:10536/DRO/DU:30050819. PMID 23245604. S2CID 1541253. Archived from the original on 19 May 2020. Retrieved 18 March 2020.
- ^ a b c «Global Tuberculosis Control 2011» (PDF). World Health Organization (WHO). Archived from the original (PDF) on 17 June 2012. Retrieved 15 April 2012.
- ^ «Tuberculosis». WHO. 24 March 2020. Archived from the original on 30 July 2020. Retrieved 31 May 2020.
- ^ Douglas AS, Strachan DP, Maxwell JD (September 1996). «Seasonality of tuberculosis: the reverse of other respiratory diseases in the UK». Thorax. 51 (9): 944–946. doi:10.1136/thx.51.9.944. PMC 472621. PMID 8984709.
- ^ Martineau AR, Nhamoyebonde S, Oni T, Rangaka MX, Marais S, Bangani N, et al. (November 2011). «Reciprocal seasonal variation in vitamin D status and tuberculosis notifications in Cape Town, South Africa». Proceedings of the National Academy of Sciences of the United States of America. 108 (47): 19013–19017. doi:10.1073/pnas.1111825108. PMC 3223428. PMID 22025704.
- ^ Parrinello CM, Crossa A, Harris TG (January 2012). «Seasonality of tuberculosis in New York City, 1990-2007». The International Journal of Tuberculosis and Lung Disease. 16 (1): 32–37. doi:10.5588/ijtld.11.0145. PMID 22236842.
- ^ a b Korthals Altes H, Kremer K, Erkens C, van Soolingen D, Wallinga J (May 2012). «Tuberculosis seasonality in the Netherlands differs between natives and non-natives: a role for vitamin D deficiency?». The International Journal of Tuberculosis and Lung Disease. 16 (5): 639–644. doi:10.5588/ijtld.11.0680. PMID 22410705.
- ^ Koh GC, Hawthorne G, Turner AM, Kunst H, Dedicoat M (2013). «Tuberculosis incidence correlates with sunshine: an ecological 28-year time series study». PLOS ONE. 8 (3): e57752. Bibcode:2013PLoSO…857752K. doi:10.1371/journal.pone.0057752. PMC 3590299. PMID 23483924.
- ^ Kuddus MA, McBryde ES, Adegboye OA (September 2019). «Delay effect and burden of weather-related tuberculosis cases in Rajshahi province, Bangladesh, 2007-2012». Scientific Reports. 9 (1): 12720. Bibcode:2019NatSR…912720K. doi:10.1038/s41598-019-49135-8. PMC 6722246. PMID 31481739.
- ^ Griffith DE, Kerr CM (August 1996). «Tuberculosis: disease of the past, disease of the present». Journal of PeriAnesthesia Nursing. 11 (4): 240–45. doi:10.1016/S1089-9472(96)80023-2. PMID 8964016.
- ^ «Global Tuberculosis Control Report, 2006 – Annex 1 Profiles of high-burden countries» (PDF). World Health Organization (WHO). Archived from the original (PDF) on 26 July 2009. Retrieved 13 October 2006.
- ^ «2005 Surveillance Slide Set». Centers for Disease Control and Prevention. 12 September 2006. Archived from the original on 23 November 2006. Retrieved 13 October 2006.
- ^ FitzGerald JM, Wang L, Elwood RK (February 2000). «Tuberculosis: 13. Control of the disease among aboriginal people in Canada». Canadian Medical Association Journal. 162 (3): 351–55. PMC 1231016. PMID 10693593.
- ^ Quah SR, Carrin G, Buse K, Heggenhougen K (2009). Health Systems Policy, Finance, and Organization. Boston: Academic Press. p. 424. ISBN 978-0-12-375087-7. Archived from the original on 6 September 2015.
- ^ Medical Research Council.Origins of the MRC. Archived 11 April 2008 at the Wayback Machine Accessed 7 October 2006.
- ^ DaVanzo, Julie; Farnsworth, Gwen (1 January 1996). «Russia’s Demographic».
- ^ Global Tuberculosis Control Archived 12 December 2006 at the Wayback Machine, World Health Organization, 2011.
- ^ «WHO global tuberculosis report 2016. Annex 2. Country profiles: Russian Federation». Archived from the original on 14 July 2017. Retrieved 22 August 2020.
- ^ a b c «Global Tuberculosis Report 2018» (PDF). Archived (PDF) from the original on 7 August 2020. Retrieved 27 September 2019.
- ^ «WHO Global tuberculosis report 2016: India». Archived from the original on 6 February 2018. Retrieved 22 August 2020.
- ^ «Govt revisits strategy to combat tuberculosis». Daily News and Analysis. 8 April 2017. Archived from the original on 3 June 2021. Retrieved 22 August 2020.
- ^ Mahla RS (August 2018). «Prevalence of drug-resistant tuberculosis in South Africa». The Lancet. Infectious Diseases. 18 (8): 836. doi:10.1016/S1473-3099(18)30401-8. PMID 30064674.
- ^ Birn AE (2009). Textbook of International Health: Global Health in a Dynamic World. p. 261. ISBN 978-0-19-988521-3. Archived from the original on 6 September 2015.
- ^ «CDC Surveillance Slides 2012 – TB». Centers for Disease Control and Prevention. 24 October 2018. Archived from the original on 9 November 2013. Retrieved 17 September 2017.
- ^ Al-Azem A, Kaushal Sharma M, Turenne C, Hoban D, Hershfield E, MacMorran J, Kabani A (1998). «Rural outbreaks of Mycobacterium tuberculosis in a Canadian province». Abstr Intersci Conf Antimicrob Agents Chemother. 38: 555. abstract no. L-27. Archived from the original on 18 November 2011.
- ^ «Tuberculosis incidence (per 100,000 people)». Our World in Data. Archived from the original on 26 September 2019. Retrieved 7 March 2020.
- ^ «Tuberculosis deaths by region». Our World in Data. Archived from the original on 8 May 2020. Retrieved 7 March 2020.
- ^ Rothschild BM, Martin LD, Lev G, Bercovier H, Bar-Gal GK, Greenblatt C, et al. (August 2001). «Mycobacterium tuberculosis complex DNA from an extinct bison dated 17,000 years before the present». Clinical Infectious Diseases. 33 (3): 305–11. doi:10.1086/321886. PMID 11438894.
- ^ Pearce-Duvet JM (August 2006). «The origin of human pathogens: evaluating the role of agriculture and domestic animals in the evolution of human disease». Biological Reviews of the Cambridge Philosophical Society. 81 (3): 369–82. doi:10.1017/S1464793106007020. PMID 16672105. S2CID 6577678.
- ^ Comas I, Gagneux S (October 2009). Manchester M (ed.). «The past and future of tuberculosis research». PLOS Pathogens. 5 (10): e1000600. doi:10.1371/journal.ppat.1000600. PMC 2745564. PMID 19855821.
- ^ Zink AR, Sola C, Reischl U, Grabner W, Rastogi N, Wolf H, et al. (January 2003). «Characterization of Mycobacterium tuberculosis complex DNAs from Egyptian mummies by spoligotyping». Journal of Clinical Microbiology. 41 (1): 359–67. doi:10.1128/JCM.41.1.359-367.2003. PMC 149558. PMID 12517873.
- ^ Konomi N, Lebwohl E, Mowbray K, Tattersall I, Zhang D (December 2002). «Detection of mycobacterial DNA in Andean mummies». Journal of Clinical Microbiology. 40 (12): 4738–40. doi:10.1128/JCM.40.12.4738-4740.2002. PMC 154635. PMID 12454182.
- ^ Sledzik PS, Bellantoni N (June 1994). «Brief communication: bioarcheological and biocultural evidence for the New England vampire folk belief» (PDF). American Journal of Physical Anthropology. 94 (2): 269–74. doi:10.1002/ajpa.1330940210. PMID 8085617. Archived (PDF) from the original on 18 February 2017.
- ^ Léon Charles Albert Calmette at Who Named It?
- ^ Trail RR (April 1970). «Richard Morton (1637-1698)». Medical History. 14 (2): 166–74. doi:10.1017/S0025727300015350. PMC 1034037. PMID 4914685.
- ^ Marten B (1720). A New Theory of Consumptions—More Especially a Phthisis or Consumption of the Lungs. London, England: T. Knaplock. P. 51: «The Original and Essential Cause … may possibly be some certain Species of Animalcula or wonderfully minute living Creatures, … » P. 79: «It may be therefore very likely, that by an habitual lying in the same Bed with a Consumptive Patient, constantly Eating and Drinking with him, or by very frequently conversing so nearly, as to draw in part of the Breath he emits from his Lungs, a Consumption may be caught by a sound Person; … «
- ^ Laennec RT (1819). De l’auscultation médiate … (in French). Vol. 1. Paris, France: J.-A. Brosson et J.-S Chaudé. p. 20. Archived from the original on 2 June 2021. Retrieved 6 December 2020. From p. 20: «L’existence des tubercules dans le poumon est la cause et constitue le charactère anatomique propre de la phthisie pulmonaire (a). (a) … l’effet dont cette maladie tire son nom, c’est-à-dire, la consumption.» (The existence of tubercles in the lung is the cause and constitutes the unique anatomical characteristic of pulmonary tuberculosis (a). (a) … the effect from which this malady [pulmonary tuberculosis] takes its name, that is, consumption.)
- ^ Schönlein JL (1832). Allgemeine und specielle Pathologie und Therapie [General and Special Pathology and Therapy] (in German). Vol. 3. Würzburg, (Germany): C. Etlinger. p. 103. Archived from the original on 2 June 2021. Retrieved 6 December 2020.
- ^ The word «tuberculosis» first appeared in Schönlein’s clinical notes in 1829. See: Jay SJ, Kırbıyık U, Woods JR, Steele GA, Hoyt GR, Schwengber RB, Gupta P (November 2018). «Modern theory of tuberculosis: culturomic analysis of its historical origin in Europe and North America». The International Journal of Tuberculosis and Lung Disease. 22 (11): 1249–1257. doi:10.5588/ijtld.18.0239. PMID 30355403. S2CID 53027676. See especially Appendix, p. iii.
- ^ Kentucky: Mammoth Cave long on history. Archived 13 August 2006 at the Wayback Machine CNN. 27 February 2004. Accessed 8 October 2006.
- ^ a b c McCarthy OR (August 2001). «The key to the sanatoria». Journal of the Royal Society of Medicine. 94 (8): 413–17. doi:10.1177/014107680109400813. PMC 1281640. PMID 11461990. Archived from the original on 3 August 2012. Retrieved 28 September 2011.
- ^ Villemin JA (1865). «Cause et nature de la tuberculose» [Cause and nature of tuberculosis]. Bulletin de l’Académie Impériale de Médecine (in French). 31: 211–216.
- See also: Villemin JA (1868). Etudes sur la tuberculose: preuves rationnelles et expérimentales de sa spécificité et de son inoculabilité [Studies of tuberculosis: rational and experimental evidence of its specificity and inoculability] (in French). Paris, France: J.-B. Baillière et fils.
- ^ Burdon-Sanderson, John Scott. (1870) «Introductory Report on the Intimate Pathology of Contagion.» Appendix to: Twelfth Report to the Lords of Her Majesty’s Most Honourable Privy Council of the Medical Officer of the Privy Council [for the year 1869], Parliamentary Papers (1870), vol. 38, 229–256.
- ^ Koch R (24 March 1882). «Die Ätiologie der Tuberkulose» [The Etiology of Tuberculosis]. Berliner Klinische Wochenschrift. 19: 221–30. doi:10.1007/978-3-662-56454-7_4. ISBN 978-3-662-56454-7. Archived from the original on 6 November 2018. Retrieved 15 June 2021.
- ^ «History: World TB Day». Centers for Disease Control and Prevention (CDC). 12 December 2016. Archived from the original on 7 December 2018. Retrieved 23 March 2019.
- ^ «The Nobel Prize in Physiology or Medicine 1905». NobelPrize.org. Retrieved 20 February 2023.
- ^ Waddington K (January 2004). «To stamp out ‘so terrible a malady’: bovine tuberculosis and tuberculin testing in Britain, 1890–1939». Medical History. 48 (1): 29–48. doi:10.1017/S0025727300007043. PMC 546294. PMID 14968644.
- ^ Bonah C (December 2005). «The ‘experimental stable’ of the BCG vaccine: safety, efficacy, proof, and standards, 1921–1933». Studies in History and Philosophy of Biological and Biomedical Sciences. 36 (4): 696–721. doi:10.1016/j.shpsc.2005.09.003. PMID 16337557.
- ^ Comstock GW (September 1994). «The International Tuberculosis Campaign: a pioneering venture in mass vaccination and research». Clinical Infectious Diseases. 19 (3): 528–40. doi:10.1093/clinids/19.3.528. PMID 7811874.
- ^ Hannaway C (2008). Biomedicine in the twentieth century: practices, policies, and politics. Amsterdam: IOS Press. p. 233. ISBN 978-1-58603-832-8. Archived from the original on 7 September 2015.
- ^ Bloom BR (1994). Tuberculosis: pathogenesis, protection, and control. Washington, DC: ASM Press. ISBN 978-1-55581-072-6.
- ^ Frith J. «History of Tuberculosis. Part 1 – Phthisis, consumption and the White Plague». Journal of Military and Veterans’ Health. Archived from the original on 8 April 2021. Retrieved 26 February 2021.
- ^ Zürcher K, Zwahlen M, Ballif M, Rieder HL, Egger M, Fenner L (5 October 2016). «Influenza Pandemics and Tuberculosis Mortality in 1889 and 1918: Analysis of Historical Data from Switzerland». PLOS ONE. 11 (10): e0162575. Bibcode:2016PLoSO..1162575Z. doi:10.1371/journal.pone.0162575. PMC 5051959. PMID 27706149.
- ^ a b
- ^ Shields T (2009). General thoracic surgery (7th ed.). Philadelphia: Wolters Kluwer Health/Lippincott Williams & Wilkins. p. 792. ISBN 978-0-7817-7982-1. Archived from the original on 6 September 2015.
- ^ Lalloo UG, Naidoo R, Ambaram A (May 2006). «Recent advances in the medical and surgical treatment of multi-drug resistant tuberculosis». Current Opinion in Pulmonary Medicine. 12 (3): 179–85. doi:10.1097/01.mcp.0000219266.27439.52. PMID 16582672. S2CID 24221563.
- ^ «Frequently asked questions about TB and HIV». World Health Organization (WHO). Archived from the original on 8 August 2011. Retrieved 15 April 2012.
- ^ a b c Lawlor C. «Katherine Byrne, Tuberculosis and the Victorian Literary Imagination». British Society for Literature and Science. Archived from the original on 6 November 2020. Retrieved 11 June 2017.
- ^ «Hippocrates 3.16 Classics, MIT». Archived from the original on 11 February 2005. Retrieved 15 December 2015.
{{cite web}}: CS1 maint: unfit URL (link) - ^ Caldwell M (1988). The Last Crusade. New York: Macmillan. p. 21. ISBN 978-0-689-11810-4.
- ^ Bunyan J (1808). The Life and Death of Mr. Badman. London: W. Nicholson. p. 244. Retrieved 28 September 2016 – via Internet Archive.
captain.
- ^ Byrne K (2011). Tuberculosis and the Victorian Literary Imagination. Cambridge University Press. ISBN 978-1-107-67280-2.
- ^ «About Chopin’s illness». Icons of Europe. Archived from the original on 28 September 2017. Retrieved 11 June 2017.
- ^ Vilaplana C (March 2017). «A literary approach to tuberculosis: lessons learned from Anton Chekhov, Franz Kafka, and Katherine Mansfield». International Journal of Infectious Diseases. 56: 283–85. doi:10.1016/j.ijid.2016.12.012. PMID 27993687.
- ^ Rogal SJ (1997). A William Somerset Maugham Encyclopedia. Greenwood Publishing. p. 245. ISBN 978-0-313-29916-2. Archived from the original on 2 June 2021. Retrieved 4 October 2017.
- ^ Eschner K. «George Orwell Wrote ‘1984’ While Dying of Tuberculosis». Smithsonian. Archived from the original on 24 March 2019. Retrieved 25 March 2019.
- ^ «Tuberculosis (whole issue)». Journal of the American Medical Association. 293 (22): cover. 8 June 2005. Archived from the original on 24 August 2020. Retrieved 4 October 2017.
- ^ Lemlein RF (1981). «Influence of Tuberculosis on the Work of Visual Artists: Several Prominent Examples». Leonardo. 14 (2): 114–11. doi:10.2307/1574402. JSTOR 1574402. S2CID 191371443. Archived from the original on 27 August 2021. Retrieved 31 January 2020.
- ^ Wilsey AM (May 2012). ‘Half in Love with Easeful Death:’ Tuberculosis in Literature. Humanities Capstone Projects (PhD Thesis thesis). Pacific University. Archived from the original on 11 October 2017. Retrieved 28 September 2017.
- ^ a b Morens DM (November 2002). «At the deathbed of consumptive art». Emerging Infectious Diseases. 8 (11): 1353–8. doi:10.3201/eid0811.020549. PMC 2738548. PMID 12463180.
- ^ «Pulmonary Tuberculosis/In Literature and Art». McMaster University History of Diseases. Retrieved 9 June 2017.
- ^ Thomson G (1 June 2016). «Van Morrison – 10 of the best». The Guardian. Archived from the original on 14 August 2020. Retrieved 28 September 2017.
- ^ «Tuberculosis Throughout History: The Arts» (PDF). United States Agency for International Development (USAID). Archived (PDF) from the original on 30 June 2017. Retrieved 12 June 2017.
- ^ Corliss R (22 December 2008). «Top 10 Worst Christmas Movies». Time. Archived from the original on 22 September 2020. Retrieved 28 September 2017.
‘If you don’t cry when Bing Crosby tells Ingrid Bergman she has tuberculosis’, Joseph McBride wrote in 1973, ‘I never want to meet you, and that’s that.’
- ^ «The End TB Strategy». who.int. Archived from the original on 22 July 2021. Retrieved 22 July 2021.
- ^ a b c d Global tuberculosis report 2020. World Health Organization. 2020. ISBN 978-92-4-001313-1. Archived from the original on 22 July 2021. Retrieved 22 July 2021.
- ^ a b «Public–Private Partnership Announces Immediate 40 Percent Cost Reduction for Rapid TB Test» (PDF). World Health Organization (WHO). 6 August 2012. Archived (PDF) from the original on 29 October 2013.
- ^ Lawn SD, Nicol MP (September 2011). «Xpert® MTB/RIF assay: development, evaluation and implementation of a new rapid molecular diagnostic for tuberculosis and rifampicin resistance». Future Microbiology. 6 (9): 1067–82. doi:10.2217/fmb.11.84. PMC 3252681. PMID 21958145.
- ^ «WHO says Cepheid rapid test will transform TB care». Reuters. 8 December 2010. Archived from the original on 11 December 2010.
- ^ STOPTB (5 April 2013). «The Stop TB Partnership, which operates through a secretariat hosted by the World Health Organization (WHO) in Geneva, Switzerland» (PDF). Archived (PDF) from the original on 24 January 2014.
- ^ Lienhardt C, Espinal M, Pai M, Maher D, Raviglione MC (November 2011). «What research is needed to stop TB? Introducing the TB Research Movement». PLOS Medicine. 8 (11): e1001135. doi:10.1371/journal.pmed.1001135. PMC 3226454. PMID 22140369.
- ^ Sandhu GK (2011). «Tuberculosis: Current Situation, Challenges and Overview of its Control Programs in India». Journal of Global Infectious Diseases. 3 (2): 143–150. doi:10.4103/0974-777X.81691. ISSN 0974-777X. PMC 3125027. PMID 21731301.
- ^ Bhargava A, Pinto L, Pai M (2011). «Mismanagement of tuberculosis in India: Causes, consequences, and the way forward» (PDF). Hypothesis. 9 (1): e7. Archived from the original on 14 March 2016.
{{cite journal}}: CS1 maint: unfit URL (link) - ^ Amdekar Y (July 2009). «Changes in the management of tuberculosis». Indian Journal of Pediatrics. 76 (7): 739–42. doi:10.1007/s12098-009-0164-4. PMID 19693453. S2CID 41788291. Archived from the original on 27 August 2021. Retrieved 31 January 2020.
- ^ Fox GJ, Dobler CC, Marks GB (September 2011). «Active case finding in contacts of people with tuberculosis». The Cochrane Database of Systematic Reviews. 2011 (9): CD008477. doi:10.1002/14651858.CD008477.pub2. PMC 6532613. PMID 21901723.
- ^ Mhimbira FA, Cuevas LE, Dacombe R, Mkopi A, Sinclair D, et al. (Cochrane Infectious Diseases Group) (November 2017). «Interventions to increase tuberculosis case detection at primary healthcare or community-level services». The Cochrane Database of Systematic Reviews. 2017 (11): CD011432. doi:10.1002/14651858.CD011432.pub2. PMC 5721626. PMID 29182800.
- ^ Braganza Menezes D, Menezes B, Dedicoat M, et al. (Cochrane Infectious Diseases Group) (August 2019). «Contact tracing strategies in household and congregate environments to identify cases of tuberculosis in low- and moderate-incidence populations». The Cochrane Database of Systematic Reviews. 2019 (8): CD013077. doi:10.1002/14651858.CD013077.pub2. PMC 6713498. PMID 31461540.
- ^ a b c d e f g Courtwright A, Turner AN (July–August 2010). «Tuberculosis and stigmatization: pathways and interventions». Public Health Reports. 125 Suppl 4 (4_suppl): 34–42. doi:10.1177/00333549101250S407. PMC 2882973. PMID 20626191.
- ^ Mason PH, Roy A, Spillane J, Singh P (March 2016). «Social, Historical and Cultural Dimensions of Tuberculosis». Journal of Biosocial Science. 48 (2): 206–32. doi:10.1017/S0021932015000115. PMID 25997539.
- ^ a b c Martín Montañés C, Gicquel B (March 2011). «New tuberculosis vaccines». Enfermedades Infecciosas y Microbiologia Clinica. 29 Suppl 1: 57–62. doi:10.1016/S0213-005X(11)70019-2. PMID 21420568.
- ^ Zhu B, Dockrell HM, Ottenhoff TH, Evans TG, Zhang Y (April 2018). «Tuberculosis vaccines: Opportunities and challenges». Respirology. 23 (4): 359–368. doi:10.1111/resp.13245. PMID 29341430.
- ^ Ibanga HB, Brookes RH, Hill PC, Owiafe PK, Fletcher HA, Lienhardt C, et al. (August 2006). «Early clinical trials with a new tuberculosis vaccine, MVA85A, in tuberculosis-endemic countries: issues in study design». The Lancet. Infectious Diseases. 6 (8): 522–8. doi:10.1016/S1473-3099(06)70552-7. PMID 16870530.
- ^ Kaufmann SH (October 2010). «Future vaccination strategies against tuberculosis: thinking outside the box». Immunity. 33 (4): 567–77. doi:10.1016/j.immuni.2010.09.015. PMID 21029966.
- ^ Webber D, Kremer M (2001). «Stimulating Industrial R&D for Neglected Infectious Diseases: Economic Perspectives» (PDF). Bulletin of the World Health Organization. 79 (8): 693–801. Archived (PDF) from the original on 26 September 2007.
- ^ Barder O, Kremer M, Williams H (2006). «Advance Market Commitments: A Policy to Stimulate Investment in Vaccines for Neglected Diseases». The Economists’ Voice. 3 (3). doi:10.2202/1553-3832.1144. S2CID 154454583. Archived from the original on 5 November 2006.
- ^ Department of Economic and Social Affairs (2009). Achieving the global public health agenda: dialogues at the Economic and Social Council. New York: United Nations. p. 103. ISBN 978-92-1-104596-3. Archived from the original on 6 September 2015.
- ^ Jong EC, Zuckerman JN (2010). Travelers’ vaccines (2nd ed.). Shelton, CT: People’s Medical Publishing House. p. 319. ISBN 978-1-60795-045-5. Archived from the original on 6 September 2015.
- ^ Bill and Melinda Gates Foundation Announcement (12 February 2004). «Gates Foundation Commits $82.9 Million to Develop New Tuberculosis Vaccines». Archived from the original on 10 October 2009.
- ^ Nightingale K (19 September 2007). «Gates foundation gives US$280 million to fight TB». Archived from the original on 1 December 2008.
- ^ a b Zumla A, Hafner R, Lienhardt C, Hoelscher M, Nunn A (March 2012). «Advancing the development of tuberculosis therapy». Nature Reviews. Drug Discovery. 11 (3): 171–2. doi:10.1038/nrd3694. PMID 22378254. S2CID 7232434. Archived from the original on 12 January 2020. Retrieved 8 May 2020.
- ^ «J&J Sirturo Wins FDA Approval to Treat Drug-Resistant TB». Bloomberg News. 31 December 2012. Archived from the original on 4 January 2013. Retrieved 1 January 2013.
- ^ a b Avorn J (April 2013). «Approval of a tuberculosis drug based on a paradoxical surrogate measure». JAMA. 309 (13): 1349–50. doi:10.1001/jama.2013.623. PMID 23430122.
- ^ US Food and Drug Administration. «Briefing Package: NDA 204–384: Sirturo» (PDF). Food and Drug Administration. Archived (PDF) from the original on 4 January 2014.
- ^ Zuckerman D, Yttri J (January 2013). «Antibiotics: When science and wishful thinking collide». Health Affairs. doi:10.1377/forefront.20130125.027503.
- ^ Critchley JA, Orton LC, Pearson F (November 2014). «Adjunctive steroid therapy for managing pulmonary tuberculosis». The Cochrane Database of Systematic Reviews. 2014 (11): CD011370. doi:10.1002/14651858.CD011370. PMC 6532561. PMID 25387839.
- ^ Shivaprasad HL, Palmieri C (January 2012). «Pathology of mycobacteriosis in birds». The Veterinary Clinics of North America. Exotic Animal Practice. 15 (1): 41–55, v–vi. doi:10.1016/j.cvex.2011.11.004. PMID 22244112.
- ^ Reavill DR, Schmidt RE (January 2012). «Mycobacterial lesions in fish, amphibians, reptiles, rodents, lagomorphs, and ferrets with reference to animal models». The Veterinary Clinics of North America. Exotic Animal Practice. 15 (1): 25–40, v. doi:10.1016/j.cvex.2011.10.001. PMID 22244111.
- ^ Mitchell MA (January 2012). «Mycobacterial infections in reptiles». The Veterinary Clinics of North America. Exotic Animal Practice. 15 (1): 101–11, vii. doi:10.1016/j.cvex.2011.10.002. PMID 22244116.
- ^ Wobeser GA (2006). Essentials of disease in wild animals (1st ed.). Ames, IO [u.a.]: Blackwell Publishing. p. 170. ISBN 978-0-8138-0589-4. Archived from the original on 6 September 2015.
- ^ Ryan TJ, Livingstone PG, Ramsey DS, de Lisle GW, Nugent G, Collins DM, et al. (February 2006). «Advances in understanding disease epidemiology and implications for control and eradication of tuberculosis in livestock: the experience from New Zealand». Veterinary Microbiology. 112 (2–4): 211–19. doi:10.1016/j.vetmic.2005.11.025. PMID 16330161.
- ^ White PC, Böhm M, Marion G, Hutchings MR (September 2008). «Control of bovine tuberculosis in British livestock: there is no ‘silver bullet’«. Trends in Microbiology. 16 (9): 420–7. CiteSeerX 10.1.1.566.5547. doi:10.1016/j.tim.2008.06.005. PMID 18706814.
- ^ Ward AI, Judge J, Delahay RJ (January 2010). «Farm husbandry and badger behaviour: opportunities to manage badger to cattle transmission of Mycobacterium bovis?». Preventive Veterinary Medicine. 93 (1): 2–10. doi:10.1016/j.prevetmed.2009.09.014. PMID 19846226.
- ^ Holt N (24 March 2015). «The Infected Elephant in the Room». Slate. Archived from the original on 14 April 2016. Retrieved 5 April 2016.
- ^ Mikota SK. «A Brief History of TB in Elephants» (PDF). Animal and Plant Health Inspection Service (APHIS). Archived (PDF) from the original on 6 October 2016. Retrieved 5 April 2016.
External links
- Tuberculosis at Curlie
- «Tuberculosis (TB)». Centers for Disease Control and Prevention (CDC). 24 October 2018.
- «Tuberculosis (TB)». London: Health Protection Agency. Archived from the original on 5 July 2007.
- WHO global 2016 TB report (infographic)
- WHO tuberculosis country profiles
- «Tuberculosis Among African Americans», 1990-11-01, In Black America; KUT Radio, American Archive of Public Broadcasting (WGBH and the Library of Congress)
- Working Group on New TB drugs, tracking clinical trials and drug candidates
Опубликовано: 27.07.2021 12:30:00 Обновлено: 27.07.2021 Просмотров: 233672

Туберкулез – это инфекционное заболевание, вызываемое палочкой Коха (Mycobacterium tuberculosis). Патоген чаще всего поражает легкие, но существуют и другие формы: туберкулез костей, суставов, почек, кожи и других органов.
Процент смертности от туберкулеза по всему миру высок, он входит в десятку заболеваний, приводящих к летальным исходам [1]. Это не только медицинская, но и социальная проблема, поскольку на заболеваемость, помимо состояния здоровья, также влияют социальные и экономические причины, качество питания и образ жизни. Ключевыми факторами риска считаются вредные привычки, ослабленная иммунная система и хронический стресс.
Как передается туберкулез
Возбудитель передается от человека к человеку воздушно-капельным путем при чихании и кашле и просто при разговоре, а также иногда контактно (через поврежденную кожу или внутриутробно). Бактерии туберкулеза долго сохраняются активными во внешней среде в плохо проветриваемом помещении и попадают в организм здорового человека через предметы быта и продукты питания.
Заражение туберкулезом еще не означает начало заболевания: оно развивается только у 5-15% инфицированных. До развития первых симптомов может пройти несколько недель или месяцев, и основным фактором риска считается ослабление иммунных сил организма [1].
Классификация туберкулеза
Это заболевание классифицируют по многим параметрам. В первую очередь туберкулез бывает первичным (впервые возникший) и вторичным (повторное заражение). По степени заразности туберкулеза различают две формы:
- открытая форма (больной активно выделяет микобактерии в воздух и заражает других людей);
- закрытая форма (больной является носителем и не выделяет возбудителя в окружающую среду).
По течению заболевания разделяют три стадии туберкулеза:
- первичное заражение с локальным воспалением в области проникновения и вовлечением близлежащих лимфоузлов;
- латентный период с образованием очагов воспаления в других органах;
- активная инфекция с ухудшением общего состояния здоровья, образованием каверн (полостей) в легких и множественными поражениями в других органах [2].
Симптомы туберкулеза
Признаки заражения различаются в зависимости от органа, пораженного микобактерией. Общие симптомы включают утомляемость, сниженную трудоспособность, плохой аппетит, повышенную температуру тела, потерю веса, появление румянца на щеках.
Для туберкулеза легких у взрослых характерны следующие основные симптомы:
- затяжной кашель на протяжении нескольких недель (сухой или мокрый);
- кровохаркание;
- боль в области груди;
- затрудненное дыхание;
- увеличение периферических лимфоузлов (в области головы, шеи и конечностей);
- ночная потливость;
- периодическое повышение температуры.
Вторичное (повторное) заражение протекает хронически в виде слабовыраженной аллергии, поскольку пациент уже обладает противотуберкулезным иммунитетом.
Клинические признаки туберкулеза у детей развиваются быстрее и более выражены. Риск заражения у этой группы пациентов выше. Это связано с возрастными особенностями строения органов и нестойкостью иммунитета ребенка к агрессивным инфекциям. Помимо «взрослых» симптомов у детей также отмечаются капризность, плаксивость, необоснованная беспокойность и нарушения сна.
Диагностика туберкулеза
Это заболевание, особенно закрытая форма, сложно диагностируется. Переход из латентной фазы в активную смазанный, а клинические симптомы не позволяют установить точный диагноз или отсутствуют. В связи с этим решающее значение имеет лабораторная диагностика.
Проба Манту (или туберкулиновая проба). Для проведения этого классического анализа на туберкулез пациенту подкожно в области предплечья вводят очищенный туберкулин – смесь белков, характерных для микобактерий. Оценку иммунологической реакции проводят через 48-72 часов на основании диаметра папулы (узелка над поверхностью кожи) или участка покраснения в месте введения туберкулина. У людей, неинфицированных бактерией, папулы не образуются или их размеры незначительны. К основным недостаткам метода относятся непереносимость туберкулина и ложноположительная реакция у людей, вакцинированных от туберкулеза вакциной БЦЖ.
Квантифероновый тест на туберкулез. Этот современный иммунологический метод позволяет выявить латентный туберкулез, а также туберкулезное поражение других органов. Введения туберкулина не требуется, поэтому этот тест подходит уязвимым группам пациентов (беременные и кормящие женщины, пожилые люди, ВИЧ-инфицированные, люди с непереносимостью туберкулина). Для диагностики используется венозная кровь. Наличие в организме активного туберкулеза обуславливает появление в крови особых белков, входящих в состав микобактерий. Т-лимфоциты реагируют на присутствие этих белков и в результате такой сенсибилизации начинают усиленно вырабатывать интерферон-гамма. Квантифероновый тест основан на измерении уровня интерферона-гамма, повышение которого указывает на наличие туберкулезной инфекции в пробе крови.
Метод T-SPOT.TB. Позволяет диагностировать латентную и активную формы легочного и внелегочного туберкулеза. Для исследования используют венозную кровь. В основе метода лежит оценка количества самих сенсибилизированных Т-лимфоцитов. Он также не дает ложноположительных результатов и подходит уязвимым группам пациентов.
Анализ мокроты. Для проведения теста необходимо собрать утреннюю мокроту, которая отделяется при кашле. Во взятом образце определяют наличие самих микобактерий. Анализ подходит только для диагностики туберкулеза легких.
Анализ мочи. Выявляют изменения параметров, характерные для туберкулеза: появление лейкоцитов, эритроцитов, бактерий, белка, гноя, сдвиг реакции мочи в кислую сторону.
Отрицательные лабораторные анализы не гарантируют отсутствие туберкулеза. Пациенты с подозрением на заболевание проходят флюорографию и/или рентгенографию легких. Для выявления внелегочных форм туберкулеза проводят МРТ, КТ и другие инструментальные исследования. Также применяют биопсию (взятие образца тканей) для микроскопических исследований и посевов на питательные среды.
Дифференциальную диагностику проводят с широким рядом заболеваний в тех случаях, когда ни одно исследование не подтвердило наличие микобактерий, присутствуют атипичные симптомы или отсутствует адекватный ответ на противотуберкулезное лечение.
Лечение туберкулеза
Туберкулез излечим на начальных стадиях. Необходима комплексная и непрерывная терапия в зависимости от пораженного органа, состояния иммунной системы и стадии заболевания:
- Медикаментозная терапия. Противотуберкулезные препараты разделяют на основные (назначаются пациентам с первичным заражением), резервные (назначаются при неэффективности препаратов основной группы или их непереносимости) и комбинированные (многокомпонентные препараты с фиксированной дозой отдельных компонентов).
- Химиотерапия. Направлена на уничтожение микобактерий или подавление их размножения.
- Симптоматическое лечение конкретных нарушений и симптомов.
- Физиотерапия при туберкулезе легких с целью улучшения питания тканей и стимуляции их восстановления (ингаляции, ароматерапия, электролечение, лазеротерапия, дарсонвализация, магнитотерапия) [3].
На запущенных стадиях туберкулеза проводят операцию по удалению пораженного органа или его части (доля легкого, мочеточники, нефрэктомия).
Полное выздоровление не гарантирует отсутствие рецидива заболевания в будущем.
Профилактика туберкулеза
Полностью оградить себя от контакта с возможными распространителями туберкулеза невозможно, поэтому на первое место выходят общие правила профилактики:
- регулярные медицинские осмотры (в первую очередь ежегодная флюорография легких);
- вакцинация (вакцина БЦЖ);
- укрепление иммунитета;
- контроль хронических заболеваний;
- здоровый образ жизни и режим дня;
- хорошая среда обитания (надлежащие влажность, температура и вентиляция воздуха);
- соблюдение гигиены.
Список литературы
- Всемирная организация здравоохранения. Туберкулез.
https://www.who.int/ru/news-room/fact-sheets/detail/tuberculosis. - В. С. Самцов, И. Н. Горбач. Курс лекция по фтизиатрии. ВГМУ. Витебск, 2001.
- М. И. Перельман. Общие принципы лечения туберкулеза. Фтизиатрия: национальное руководство. Москва, 2007.
| Туберкулёз | ||
|---|---|---|
|
|
||
| Рентгенограмма органов грудной клетки больного туберкулёзом легких с распадом | ||
| МКБ-10 | A1515.-A1919. | |
| МКБ-9 | 010010—018018 | |
| OMIM | 607948 | 607948 |
| DiseasesDB | 8515 | 8515 |

Туберкулёз (от лат. tuberculum «бугорок») — широко распространённое в мире инфекционное заболевание человека и животных, вызываемое различными видами микобактерий из группы Mycobacterium tuberculosis complex (M. tuberculosis и другими близкородственными видами).[1] Туберкулёз обычно поражает лёгкие, реже затрагивая другие органы и системы. Mycobacterium tuberculosis передаётся воздушно-капельным путём при разговоре, кашле и чихании больного.[2] Чаще всего после инфицирования микобактериями заболевание протекает в бессимптомной, скрытой форме (тубинфицированность), но примерно один из десяти случаев скрытой инфекции, в конце концов, переходит в активную форму.[3]
Классические симптомы туберкулёза лёгких — длительный кашель с мокротой, иногда с кровохарканьем, появляющимся на более поздних стадиях, лихорадка, слабость, ночная потливость и значительное похудение.
Различают открытую и закрытую формы туберкулёза. При открытой форме в мокроте или в других естественных выделениях больного — моче, свищевом отделяемом, кале (как правило при туберкулёзе пищеварительного тракта, редко при туберкулёзе лёгочной ткани) обнаруживаются микобактерии туберкулёза. Открытой формой считаются также те виды туберкулеза органов дыхания, при которых, даже в отсутствие бактериовыделения, имеются явные признаки сообщения очага поражения с внешней средой: каверна (распад) в лёгком, туберкулёз бронха (особенно язвенная форма), бронхиальный или торакальный свищ, туберкулёз верхних дыхательных путей. Если больной не соблюдает гигиенических мер предосторожности, он может стать заразным для окружающих. При «закрытой» форме туберкулёза микобактерии в мокроте доступными методами не обнаруживаются, больные такой формой эпидемиологически не опасны или малоопасны для окружающих.
Диагностика туберкулёза основана на флюорографии, рентгенографии и компьютерной томографии поражённых органов и систем, микробиологическом исследовании различного биологического материала, кожной туберкулиновой пробе (реакции Манту), а также методе молекулярно-генетического анализа (метод ПЦР) и др. Лечение сложное и длительное, требующее приёма препаратов в течение минимум шести месяцев. Лиц, контактировавших с больным, обследуют рентгенологически или с помощью реакции Манту, с возможностью назначения профилактического лечения противотуберкулёзными препаратами.
Заметные сложности в лечении туберкулёза возникают при наличии устойчивости возбудителя к противотуберкулёзным препаратам основного и, реже, резервного ряда, которая может быть выявлена только при микробиологическом исследовании. Устойчивость к изониазиду и рифампицину также может быть установлена методом ПЦР. Профилактика туберкулёза основана на скрининговых программах, профосмотрах, а также на вакцинации детей вакциной БЦЖ или БЦЖ-М.
Существует мнение, что M. tuberculosis инфицирована примерно треть населения Земли,[4] и примерно каждую секунду возникает новый случай инфекции.[5] Доля людей, которые заболевают туберкулёзом каждый год во всем мире, не изменяется или снижается, однако из-за роста численности населения абсолютное число новых случаев продолжает расти.[5] В 2007 году насчитывалось 13,7 миллионов зарегистрированных случаев хронического активного туберкулёза, 9,3 миллиона новых случаев заболевания и 1,8 миллиона случаев смерти, главным образом в развивающихся странах.[6] Кроме того, всё больше людей в развитых странах заражаются туберкулёзом, потому что их иммунная система ослабевает из-за приёма иммуносупрессивных препаратов, злоупотребления психоактивными веществами и особенно при ВИЧ-инфекции. Распространение туберкулёза неравномерно по всему миру, около 80 % населения во многих азиатских и африканских странах имеют положительный результат туберкулиновых проб, и только среди 5—10 % населения США такой тест положителен.[1] По некоторым данным, на территории России тубинфицированность взрослого населения приблизительно в 10 раз выше, чем в развитых странах.[7]
Устаревшее название туберкулёза лёгких — чахо́тка (от слова чахнуть). В качестве названия туберкулёза почек и некоторых других внутренних паренхиматозных органов (печени, селезёнки), а также желёз (например, слюнных) ранее использовалось слово «бугорчатка». Наружный туберкулёз (кожи, слизистых, лимфоузлов) назывался золотухой.
Для человека заболевание является социально зависимым.[8] До XX века туберкулёз был практически неизлечим. В настоящее время разработана комплексная программа, позволяющая выявить и вылечить заболевание на ранних стадиях его развития.[9][10]
Содержание
- 1 Исторические сведения
- 2 Эпидемиология
- 2.1 Туберкулёз в России
- 2.2 Туберкулёз в Белоруссии
- 2.3 Туберкулёз на Украине
- 2.4 Карты
- 3 Этиология
- 4 Патогенез и патологическая анатомия
- 4.1 Первичное инфицирование микобактериями туберкулёза и скрытое течение туберкулёзной инфекции
- 4.2 Приобретённый клеточный иммунитет
- 4.3 Возникновение клинически выраженного туберкулёза
- 5 Клинические формы туберкулёза
- 5.1 Туберкулёз лёгких
- 5.2 Внелёгочный туберкулёз
- 6 Основные клинические проявления
- 7 Профилактика
- 8 Лечение туберкулёза
- 8.1 Виды лекарственной устойчивости у возбудителя туберкулёза
- 8.2 Трёхкомпонентная схема лечения
- 8.3 Четырёхкомпонентная схема лечения
- 8.4 Пятикомпонентная схема лечения
- 9 Прогноз
- 10 В произведениях искусства
- 11 Об ущербной пользе туберкулёза
- 12 Примечания
- 13 Литература
- 14 Ссылки
Исторические сведения[править | править вики-текст]
Ещё задолго до открытия природы инфекционных заболеваний предполагали, что туберкулёз — заразная болезнь. В вавилонском Кодексе Хаммурапи было закреплено право на развод с больной женой, у которой имелись симптомы лёгочного туберкулёза. В Индии, Португалии и Венеции были законы, требующие сообщать обо всех подобных случаях.
В XVII веке Франциск Сильвий впервые связал гранулёмы, обнаруженные в различных тканях при вскрытии трупа, с признаками чахотки.
В 1819 году французский врач Рене Лаэннек предложил метод аускультации лёгких, что имело большое значение в разработке методов диагностики туберкулёза.
В 1822 году английский врач Джеймс Карсон высказал идею и предпринял первую, правда, неудачную, попытку лечения лёгочного туберкулёза искусственным пневмотораксом (введением воздуха в плевральную полость).[11] Спустя шесть десятилетий, в 1882 году, итальянцу Карло Форланини удалось ввести этот метод в практику. В России искусственный пневмоторакс впервые применил А. Н. Рубель в 1910 году.
В 1863 году Герман Бремер основал в Германии туберкулёзный санаторий.
В 1865 году французский морской врач Жан-Антуан Вильмен наблюдал распространение туберкулёза на корабле от одного больного матроса. В доказательство инфекционной природы врач собрал мокроту больных и пропитал ею подстилку для морских свинок. Свинки заболевали туберкулёзом и умирали — исследователь доказал, что туберкулёз — заразная («вирулентная») болезнь. Инфекционную природу туберкулёза подтвердил немецкий патолог Юлиус Конгейм в 1879 году. Он помещал кусочки органов больных туберкулёзом в переднюю камеру глаза кролика и наблюдал образование туберкулёзных бугорков.
В 1868 году немецкий патолог Теодор Лангганс обнаружил в туберкулёзном бугорке гигантские клетки, позже названные в его честь.
В 1882 году в Германии Роберт Кох после 17 лет работы в лаборатории открыл возбудителя туберкулёза, которого назвали бациллой Коха (БК). Он обнаружил возбудителя при микроскопическом исследовании мокроты больного туберкулёзом после окраски препарата везувином и метиленовым синим. Впоследствии он выделил чистую культуру возбудителя и вызвал ею туберкулёз у подопытных животных. В настоящее время фтизиатры пользуются термином МБТ (микобактерия туберкулёза).
В 1882—1884 годах Франц Циль и Фридрих Нельсен (Германия) предложили эффективный метод окраски кислотоустойчивых микобактерий туберкулёза.
В 1887 году в Эдинбурге открыт первый противотуберкулёзный диспансер.
В 1890 году Роберт Кох впервые получил туберкулин, который описал как «водно-глицериновую вытяжку туберкулёзных культур». В диагностических целях Кох предложил делать подкожную пробу с введением туберкулина. На конгрессе врачей в Берлине Кох сообщил о возможном профилактическом и даже лечебном действии туберкулина, испытанного в опытах на морских свинках и применённого на себе и своей сотруднице (которая впоследствии стала его женой). Через год в Берлине было сделано официальное заключение о высокой эффективности туберкулина в диагностике, однако лечебные свойства туберкулина были названы противоречивыми, поскольку резко обострялось течение болезни.
В 1902 году в Берлине проведена первая Международная конференция по туберкулёзу.
В 1904 году А. И. Абрикосов опубликовал работы, в которых описал картину очаговых изменений в лёгких на рентгенограмме при начальных проявлениях туберкулёза у взрослых (очаг Абрикосова).
В 1907 году австрийский педиатр Клеменс Пирке предложил накожную пробу с туберкулином для выявления людей, инфицированных микобактерией туберкулёза, и ввёл понятие аллергии.
В 1910 году Шарль Манту (Франция) и Феликс Мендель (Германия) предложили внутрикожный метод введения туберкулина, который в диагностическом плане оказался чувствительнее накожного.
В 1912 году исследователь Антон Гон (Австро-Венгрия) описал обызвествлённый первичный туберкулёзный очаг (очаг Гона).
В 1919 году микробиолог Альбер Кальметт и ветеринарный врач Камиль Герен (оба — Франция) создали вакцинный штамм микобактерии туберкулёза для противотуберкулёзной вакцинации людей. Штамм был назван «бациллы Кальметта — Герена» (Bacilles Calmette-Guerin, BCG). Впервые вакцина БЦЖ была введена новорождённому ребёнку в 1921 году.
В 1925 году Кальметт передал профессору Л. А. Тарасевичу штамм вакцины БЦЖ, которая была названа БЦЖ-1. Через три года экспериментального и клинического изучения было установлено, что вакцина относительно безвредна. Смертность от туберкулёза среди вакцинированных детей в окружении бактерионосителей была меньше, чем среди невакцинированных. В 1928 году было рекомендовано вакцинировать БЦЖ новорождённых из очагов туберкулёзной инфекции. С 1935 года вакцинацию стали проводить в широких масштабах не только в городах, но и в сельской местности. В середине 1950-х вакцинация новорождённых стала обязательной. До 1962 года проводили в основном пероральную вакцинацию новорождённых, с 1962 года для вакцинации и ревакцинации стали применять более эффективный внутрикожный метод введения вакцины. В 1985 году для вакцинации новорождённых с отягощённым постнатальным периодом была предложена вакцина БЦЖ-М, которая позволяет уменьшить антигенную нагрузку вакцинируемых.
С середины 1930-х годов применяется эктомия поражённой туберкулёзом части лёгкого.
В 1943 году Зельман Ваксман совместно с Альбертом Шацем получил стрептомицин — первый противомикробный препарат, который оказывал бактериостатическое действие на микобактерии туберкулёза. Интересно отметить, что в первые несколько лет применения стрептомицин обладал крайне высокой противотуберкулёзной активностью: даже смыв с флакона, где до этого находился лиофизат препарата, давал клинический эффект. Но всего через 10 лет эффективность препарата существенно снизилась, а в настоящее время его клинический эффект минимален. К концу XX века спектр антибактериальных препаратов, применяемых во фтизиатрии, значительно расширился.
Эпидемиология[править | править вики-текст]

В соответствии с информацией ВОЗ, около 2 миллиардов людей, треть общего населения Земли, инфицировано.[13] В настоящее время туберкулёзом ежегодно заболевает 9 миллионов человек во всём мире, из них 3 миллиона умирают от его осложнений. (По другим данным, ежегодно 8 миллионов заболевают туберкулёзом, а 2 миллиона умирает.[14])
На Украине в 1995 году ВОЗ объявила эпидемию туберкулёза.
Отмечено, что заболеваемость туберкулёзом зависит от неблагоприятных условий (стрессовой нагрузки), а также от индивидуальных характеристик организма человека (например, от группы крови и возраста заболевшего). Из числа заболевших в целом доминирует возрастная группа 18 — 26 лет.[15]
Однако, несмотря на этот факт, в странах, где заболеваемость туберкулёзом значительно снизилась — таких, как Америка — доминировать среди заболевших стала статистическая группа пожилых людей.[16]
Существует несколько факторов, вызывающих повышенную восприимчивость человека к туберкулёзу:
- Наиболее значимым в мире стал ВИЧ;
- Курение (особенно более 20 сигарет в день) — увеличивает вероятность туберкулёза в 2—4 раза[17];
- Диабет.[18]
Туберкулёз в России[править | править вики-текст]
В 2007 году в России отмечено 117 738 больных впервые выявленным туберкулёзом в активной форме (82,6 на 100 тыс. населения), что на 0,2 % выше, чем в 2006 г.
В 2009 году в России отмечено 105 530 случаев впервые выявленного активного туберкулёза (в 2008 г. — 107 988 случаев). Показатель заболеваемости туберкулёзом составил 74,26 на 100 тыс. населения (в 2008 г. — 75,79 на 100 тысяч).[19]
Наиболее высокие показатели заболеваемости в 2009 году, как и в предыдущие годы, отмечались в Дальневосточном (124,1), Сибирском (100,8), Уральском (73,6) федеральных округах. В пятнадцати субъектах Российской Федерации показатель заболеваемости в 1,5 и более раза превышает средний по стране: Еврейской автономной области (159,5), Амурской (114,4), Омской (112,0), Кемеровской (110,9), Иркутской (101,2), Новосибирской (98,10), Курганской (94,94), Сахалинской (94,06) областях, республиках Тыва (164,2), Бурятия (129,8), Хакасия (103,6), Алтай (97,45), Приморском (188,3) Хабаровском (110,0), Алтайском краях (102,1).
Среди всех впервые выявленных больных туберкулёзом бациллярные больные (бактериовыделители) в 2007 году составили 40 % (47 239 человек, показатель — 33,15 на 100 тыс. населения).
В России смертность от туберкулёза за 2007 год составила 18 человек на 100 тысяч жителей (на 7 % ниже, чем в 2006 г.), таким образом, в год умирает от туберкулёза около 25 000 человек (в среднем по Европе смертность от туберкулёза приблизительно в 3 раза меньше). В структуре смертности от инфекционных и паразитарных заболеваний в России доля умерших от туберкулёза составляет 70 %.[20]
Согласно официальной статистике, показатель смертности от туберкулеза в январе — сентябре 2011 года снизился на 7,2 % в сравнении с аналогичным периодом 2010 года[21].
Туберкулёз в Белоруссии[править | править вики-текст]
В Белоруссии ежегодно туберкулёз поражает около 5 тысяч человек.[22] Противотуберкулёзная вакцина в своё время серьёзно снизила детскую заболеваемость, которая продолжает оставаться одной из самых низких на постсоветском пространстве.
Туберкулёз на Украине[править | править вики-текст]
На Украине эпидемия туберкулёза перешла в категорию национальной проблемы, поскольку стала трудноуправляемой. Сегодня этой болезнью охвачено около 700 тыс. человек, из которых 600 тыс. находятся на диспансерном учёте, в том числе 142 тыс. с открытой формой туберкулёза. Официально число туберкулёзных больных превысило 1 % населения, однако эксперты не без основания полагают, что реальное количество больных значительно отличается от данных официальной статистики. Ежегодно число больных увеличивается на 40 тыс., умирает 10 тыс. ежегодно.[23]
Карты[править | править вики-текст]
- Эпидемиологические карты
-

В 2007 году показатель распространенности туберкулёза на 100 000 человек был самым высоким в странах Африки южнее Сахары, а также относительно высокой в Азии.[6]
-

Плотность ежегодных выявлений новых случаев туберкулёза, 22 страны, что согласно ВОЗ составляет 80 % всех новых случаев заболевания туберкулёзом. 2007 год.
-
Заболеваемость туберкулезом в мире. Случаев на 100 тысяч жителей: > 300; 200—300; 100—200; 50—100; < 50; нет данных. Данные ВОЗ, 2006 год.[24]
-
Тяжесть заболевания туберкулезом в мире. В 2010 году почти треть населения была заражена микобактерией туберкулеза.




Этиология[править | править вики-текст]

Флуоресцентная окраска МБТ
Возбудителями туберкулёза являются микобактерии — кислотоустойчивые бактерии рода Mycobacterium. Всего известно 74 вида микобактерий. Они широко распространены в почве, воде, среди людей и животных. Однако туберкулёз у человека вызывает условно выделенный комплекс, включающий в себя Mycobacterium tuberculosis (человеческий вид), Mycobacterium bovis (бычий вид), Mycobacterium africanum, Mycobacterium bovis BCG (БЦЖ-штамм бычьего вида), Mycobacterium microti, Mycobacterium canettii. В последнее время к нему отнесены Mycobacterium pinnipedii, Mycobacterium caprae, филогенетически имеющие отношение к Mycobacterium microti и Mycobacterium bovis.
Туберкулёз, вызванный различными видами микобактерий, достаточно сильно различается между собой. Основной видовой признак микобактерии туберкулёза (МБТ) — патогенность, которая проявляется в вирулентности. Вирулентность может существенно изменяться в зависимости от факторов внешней среды и по-разному проявляться в зависимости от состояния макроорганизма, который подвергается бактериальной агрессии.
Патогенез и патологическая анатомия[править | править вики-текст]
В пораженных туберкулёзом органах (лёгкие, мочеполовая система, лимфатические узлы, кожа, кости, кишечник и др.) развивается специфическое «холодное» туберкулёзное воспаление, носящее преимущественно гранулематозный характер и приводящее к образованию множественных бугорков со склонностью к распаду.
Первичное инфицирование микобактериями туберкулёза и скрытое течение туберкулёзной инфекции[править | править вики-текст]
Большое значение имеет первичная локализация инфекционного очага. Различают следующие пути передачи туберкулёза:
- Воздушно-капельный. Туберкулёзные микобактерии попадают в воздух с капельками при кашле, разговоре и чихании больного активным туберкулёзом. При вдыхании эти капельки с микобактериями попадают в лёгкие здорового человека. Это самый распространённый путь заражения.
- Алиментарный. Проникновение происходит через пищеварительный тракт. Специальные эксперименты на животных показывают, что при алиментарном способе требуется значительно большее количество микобактерий, чем при аэрогенном заражении.[источник не указан 1280 дней] Если при вдыхании достаточно одной или двух микобактерий, то для заражения через пищу требуются сотни микробов.[источник не указан 1280 дней]
- Контактный. Описаны случаи заражения через конъюнктиву глаза маленьких детей и взрослых. При этом иногда обнаруживается острый конъюнктивит и воспаление слёзного мешочка. Заражение туберкулёзом через кожу встречается редко.
- Внутриутробное заражение туберкулёзом. Возможность заражения туберкулёзом плода в период внутриутробной жизни установлена у группы детей, умерших в первые дни после рождения.[источник не указан 1280 дней] Заражение происходит или при поражении туберкулёзом плаценты, или при инфицировании повреждённой плаценты во время родов больной туберкулёзом матерью. Такой путь заражения туберкулёзом встречается крайне редко.
Система дыхания защищена от проникновения микобактерий мукоцилиарным клиренсом (выделение бокаловидными клетками дыхательных путей слизи, которая склеивает поступившие микобактерии, и дальнейшая элиминация микобактерий с помощью волнообразных колебаний мерцательного эпителия). Нарушение мукоцилиарного клиренса при остром и хроническом воспалении верхних дыхательных путей, трахеи и крупных бронхов, а также под воздействием токсических веществ делает возможным проникновение микобактерий в бронхиолы и альвеолы, после чего вероятность инфицирования и заболевания туберкулёзом значительно увеличивается.
Возможность заражения алиментарным путём обусловлена состоянием стенки кишечника и его всасывающей функции.
Возбудители туберкулёза не выделяют какой-либо экзотоксин, который мог бы стимулировать фагоцитоз. Возможности фагоцитоза микобактерий на этом этапе ограничены, поэтому присутствие в тканях небольшого количества возбудителя проявляется не сразу. Микобактерии находятся вне клеток и размножаются медленно, и ткани некоторое время сохраняют нормальную структуру. Это состояние называется «латентный микробизм». Независимо от начальной локализации они с током лимфы попадают в регионарные лимфатические узлы, после чего лимфогенно распространяются по организму — происходит первичная (облигатная) микобактериемия. Микобактерии задерживаются в органах с наиболее развитым микроциркуляторным руслом (лёгкие, лимфатические узлы, корковый слой почек, эпифизы и метафизы трубчатых костей, ампуллярно-фимбриональные отделы маточных труб, увеальный тракт глаза). Поскольку возбудитель продолжает размножаться, а иммунитет ещё не сформировался, популяция возбудителя значительно увеличивается.[25]
Тем не менее, в месте скопления большого числа микобактерий начинается фагоцитоз. Сначала возбудителей начинают фагоцитировать и разрушать полинуклеарные лейкоциты, однако безуспешно — все они гибнут, вступив в контакт с МБТ, из-за слабого бактерицидного потенциала.
Затем к фагоцитозу МБТ подключаются макрофаги. Однако МБТ синтезируют АТФ-положительные протоны, сульфаты и факторы вирулентности (корд-факторы), в результате чего нарушается функция лизосом макрофагов. Образование фаголизосомы становится невозможным, поэтому лизосомальные ферменты макрофагов не могут воздействовать на поглощённые микобактерии. МБТ располагаются внутриклеточно, продолжают расти, размножаться и всё больше повреждают клетку-хозяина. Макрофаг постепенно погибает, а микобактерии вновь попадают в межклеточное пространство. Этот процесс называется «незавершённым фагоцитозом».
Приобретённый клеточный иммунитет[править | править вики-текст]
В основе приобретённого клеточного иммунитета лежит эффективное взаимодействие макрофагов и лимфоцитов. Особое значение имеет контакт макрофагов с Т-хелперами (CD4+) и Т-супрессорами (CD8+). Макрофаги, поглотившие МБТ, экспрессируют на своей поверхности антигены микобактерий (в виде пептидов) и выделяют в межклеточное пространство интерлейкин-1 (ИЛ-1), который активирует Т-лимфоциты (CD4+). В свою очередь Т-хелперы (CD4+) взаимодействуют с макрофагами и воспринимают информацию о генетической структуре возбудителя. Сенсибилизированные Т-лимфоциты (CD4+ и CD8+) выделяют хемотоксины, гамма-интерферон и интерлейкин-2 (ИЛ-2), которые активируют миграцию макрофагов в сторону расположения МБТ, повышают ферментативную и общую бактерицидную активность макрофагов. Активированные макрофаги интенсивно вырабатывают активные формы кислорода и пероксид водорода. Это так называемый кислородный взрыв; он воздействует на фагоцитируемый возбудитель туберкулёза. При одновременном воздействии L-аргинина и фактора некроза опухолей-альфа образуется оксид азота NO, который также обладает антимикробным эффектом. В результате всех этих процессов разрушительное действие МБТ на фаголизосомы ослабевает, и бактерии разрушаются лизосомальными ферментами. При адекватном иммунном ответе каждое последующее поколение макрофагов становится всё более иммунокомпетентным. Выделяемые макрофагами медиаторы активируют также B-лимфоциты, ответственные за синтез иммуноглобулинов, однако их накопление в крови на устойчивость организма к МБТ не влияет. Но выработка B-лимфоцитами опсонирующих антител, которые обволакивают микобактерии и способствуют их склеиванию, является полезной для дальнейшего фагоцитоза.
Повышение ферментативной активности макрофагов и выделение ими различных медиаторов может вести к появлению клеток гиперчувствительности замедленного типа (ГЗТ) к антигенам МБТ. Макрофаги трансформируются в эпителиоидные гигантские клетки Лангханса, которые участвуют в ограничении зоны воспаления. Образуется экссудативно-продуктивная и продуктивная туберкулёзная гранулёма, образование которой свидетельствует о хорошем иммунном ответе на инфекцию и о способности организма локализовать микобактериальную агрессию. На высоте гранулематозной реакции в гранулёме находятся Т-лимфоциты (преобладают), B-лимфоциты, макрофаги (осуществляют фагоцитоз, выполняют аффекторную и эффекторную функции); макрофаги постепенно трансформируются в эпителиоидные клетки (осуществляют пиноцитоз, синтезируют гидролитические ферменты). В центре гранулёмы может появиться небольшой участок казеозного некроза, который формируется из тел макрофагов, погибших при контакте с МБТ.
Реакция ГЗТ появляется через 2—3 недели после инфицирования, а достаточно выраженный клеточный иммунитет формируется через 8 недель. После этого размножение микобактерий замедляется, общее их число уменьшается, специфическая воспалительная реакция затихает. Но полной ликвидации возбудителя из очага воспаления не происходит. Сохранившиеся МБТ локализуются внутриклеточно (L-формы) и предотвращают формирование фаголизосомы, поэтому недоступны для лизосомальных ферментов. Такой противотуберкулёзный иммунитет называется нестерильным. Оставшиеся в организме МБТ поддерживают популяцию сенсибилизированных Т-лимфоцитов и обеспечивают достаточный уровень иммунологической активности. Таким образом, человек может сохранять МБТ в своем организме длительное время и даже всю жизнь. При ослаблении иммунитета возникает угроза активизации сохранившейся популяции МБТ и заболевания туберкулёзом.
Приобретенный иммунитет к МБТ снижается при СПИДе, сахарном диабете, язвенной болезни, злоупотреблении алкоголем и длительном применении наркотиков, а также при голодании, стрессовых ситуациях, беременности, лечении гормонами или иммунодепрессантами.
В целом риск развития туберкулёза у впервые инфицированного человека составляет около 8 % в первые 2 года после заражения, постепенно снижаясь в последующие годы.
Возникновение клинически выраженного туберкулёза[править | править вики-текст]
В случае недостаточной активации макрофагов фагоцитоз неэффективен, размножение МБТ макрофагами не контролируется и потому происходит в геометрической прогрессии. Фагоцитирующие клетки не справляются с объёмом работы и массово гибнут. При этом в межклеточное пространство поступает большое количество медиаторов и протеолитических ферментов, которые повреждают прилежащие ткани. Происходит своеобразное «разжижение» тканей, формируется особая питательная среда, способствующая росту и размножению внеклеточно расположенных МБТ.
Большая популяция МБТ нарушает баланс в иммунной защите: количество Т-супресоров (CD8+) растёт, иммунологическая активность Т-хелперов (CD4+) падает. Сначала резко усиливается, а затем ослабевает ГЗТ к антигенам МБТ. Воспалительная реакция приобретает распространённый характер. Повышается проницаемость сосудистой стенки, в ткани поступают белки плазмы, лейкоциты и моноциты. Формируются туберкулёзные гранулёмы, в которых преобладает казеозный некроз. Усиливается инфильтрация наружного слоя полинуклеарными лейкоцитами, макрофагами и лимфоидными клетками. Отдельные гранулёмы сливаются, общий объём туберкулёзного поражения увеличивается. Первичное инфицирование трансформируется в клинически выраженный туберкулёз.
Клинические формы туберкулёза[править | править вики-текст]
Чаще всего туберкулёз поражает органы дыхательной (главным образом лёгкие и бронхи) и мочеполовой систем. При костно-суставных формах туберкулёза наиболее часто встречаются поражения позвоночника и костей таза. Ввиду этого различают два основных вида туберкулёза: туберкулёз лёгких и внелёгочный туберкулёз.
Туберкулёз лёгких[править | править вики-текст]
Туберкулёз лёгких может принимать различные формы:
- первичный туберкулёзный комплекс (очаг туберкулёзной пневмонии + лимфангит, лимфаденит средостения)
- туберкулёзный бронхоаденит, изолированный лимфаденит внутригрудных лимфатических узлов.
Исходя из степени распространённости туберкулёза лёгких, различают:
- латентный туберкулёз
- диссеминированный туберкулёз;
- милиарный туберкулёз;
- очаговый (ограниченный) туберкулёз;
- инфильтративный туберкулёз;
- казеозная пневмония;
- туберкулёма;
- кавернозный туберкулёз;
- фиброзно-кавернозный туберкулёз;
- цирротический туберкулёз.
Гораздо реже встречаются туберкулёз плевры, туберкулёз гортани, трахеи.
Внелёгочный туберкулёз[править | править вики-текст]
Внелёгочный туберкулёз может локализоваться в любом органе человека. Различают следующие формы внелёгочного туберкулёза:
- Туберкулёз органов пищеварительной системы — чаще всего поражаются дистальный отдел тонкой кишки и слепая кишка;
- Туберкулёз органов мочеполовой системы — поражение почек, мочевыводящих путей, половых органов;
- Туберкулёз центральной нервной системы и мозговых оболочек — поражение спинного и головного мозга, твёрдой оболочки головного мозга (туберкулёзный менингит);
- Туберкулёз костей и суставов — чаще всего поражаются кости позвоночника;
- Туберкулёз кожи;
- Туберкулёз глаз.
Основные клинические проявления[править | править вики-текст]

«Рождение Венеры», деталь, XV век. Флорентийка Симонетта Веспуччи, с которой написана Венера, умерла в возрасте 22 лет от туберкулёза.[26] Видимое на картине резко опущенное левое плечо даёт основания предполагать, что у натурщицы имело место туберкулёзное поражение плечевого пояса.[27]
Туберкулёз лёгких может длительное время протекать бессимптомно или малосимптомно и обнаружиться случайно при проведении флюорографии или на рентгеновском снимке грудной клетки. Факт обсеменения организма туберкулёзными микобактериями и формирования специфической иммунологической гиперреактивности может быть также обнаружен при постановке туберкулиновых проб.
В случаях, когда туберкулёз проявляется клинически, обычно самыми первыми симптомами выступают неспецифические проявления интоксикации: слабость, бледность, повышенная утомляемость, вялость, апатия, субфебрильная температура (около 37 °C, редко выше 38°), потливость, особенно беспокоящая больного по ночам, похудение. Часто выявляется генерализованная или ограниченная какой-либо группой лимфатических узлов лимфаденопатия — увеличение размеров лимфатических узлов. Иногда при этом удаётся выявить специфическое поражение лимфатических узлов — «холодное» воспаление.
В крови больных туберкулёзом или обсеменённых туберкулёзной микобактерией при лабораторном исследовании часто обнаруживается анемия (снижение числа эритроцитов и содержания гемоглобина), умеренная лейкопения (снижение числа лейкоцитов). Некоторыми специалистами предполагается, что анемия и лейкопения при туберкулёзной инфекции — последствие воздействия токсинов микобактерий на костный мозг. Согласно другой точке зрения, всё обстоит строго наоборот — туберкулёзная микобактерия преимущественно «нападает» в основном на ослабленных лиц — не обязательно страдающих клинически выраженными иммунодефицитными состояниями, но, как правило, имеющих слегка пониженный иммунитет; не обязательно страдающих клинически выраженной анемией или лейкопенией, но имеющих эти параметры около нижней границы нормы и т. д. В такой трактовке анемия или лейкопения — не прямое следствие туберкулёзной инфекции, а, наоборот, предусловие её возникновения и предсуществовавший до болезни (преморбидный) фактор.
Далее по ходу развития заболевания присоединяются более или менее явные симптомы со стороны пораженного органа. При туберкулёзе лёгких это кашель, отхождение мокроты, хрипы в лёгких, насморк, иногда затруднение дыхания или боли в грудной клетке (указывающие обычно на присоединение туберкулёзного плеврита), кровохарканье. При туберкулёзе кишечника — те или иные нарушения функции кишечника, запоры, поносы, кровь в кале и т. д. Как правило (но не всегда), поражение лёгких бывает первичным, а другие органы поражаются вторично путём гематогенного обсеменения. Но встречаются случаи развития туберкулёза внутренних органов или туберкулёзного менингита без каких-либо текущих клинических или рентгенологических признаков поражения лёгких и без такового поражения в анамнезе.
Профилактика[править | править вики-текст]

Основной профилактикой туберкулёза на сегодняшний день является вакцина БЦЖ (BCG). Она надёжно защищает от самой опасной формы туберкулёза — туберкулёзного менингита[28], но при наличии противопоказаний в некоторых случаях сама может способствовать развитию костно-суставного туберкулёза[29], а у ВИЧ-инфицированных и больных СПИД — и других видов туберкулёза[30]. В соответствии с «Национальным календарём профилактических прививок» прививку делают в роддоме при отсутствии противопоказаний в первые 3—7 дней жизни ребенка. В 7 и 14 лет при отрицательной реакции Манту и отсутствии противопоказаний проводят ревакцинацию.
С целью выявления туберкулёза на ранних стадиях, всем взрослым необходимо проходить флюорографическое обследование в поликлинике не реже 1 раза в год (в зависимости от профессии, состояния здоровья и принадлежности к различным «группам риска»). Также при резком изменении реакции Манту по сравнению с предыдущей (т. н. «вираже»), фтизиатром может быть предложено провести профилактическую химиотерапию несколькими препаратами, как правило, в комплексе с гепатопротекторами и витаминами группы B.[31] У некоторых взрослых и примерно у 10 % детей, не прошедших курс профилактического лечения в период виража, развивается состояние, именуемое туберкулёзной интоксикацией.
Лечение туберкулёза[править | править вики-текст]
Лечение туберкулёза, особенно внелёгочных его форм, является сложным делом, требующим много времени и терпения, а также комплексного подхода.
Фактически с самого начала применения антибиотикотерапии возник феномен лекарственной устойчивости. Феномен обусловлен тем, что микобактерия не имеет плазмид, а популяционная устойчивость микроорганизмов к антибактериальным препаратам традиционно описывалась в микробной клетке наличием R-плазмид (от англ. resistance — устойчивость). Однако, несмотря на этот факт, отмечалось появление или исчезновение лекарственной устойчивости у одного штамма МБТ. В итоге выяснилось, что за активацию или дезактивацию генов, отвечающих за резистентность, ответственны IS-последовательности.
Виды лекарственной устойчивости у возбудителя туберкулёза[править | править вики-текст]
Различают лекарственную устойчивость:
- первичную;
- приобретённую.
К микроорганизмам с первичной устойчивостью относят штаммы, выделенные от пациентов, не получавших ранее специфическую терапию или получавших препараты в течение месяца или меньше. При невозможности уточнения факта применения противотуберкулёзных препаратов используют термин «начальная устойчивость». Если устойчивый штамм выделен у пациента на фоне противотуберкулёзной терапии, проводимой в течение месяца и более, устойчивость расценивают как «приобретённую». Частота первичной лекарственной устойчивости характеризует эпидемиологическое состояние популяции возбудителя туберкулёза. Приобретённая лекарственная устойчивость среди впервые выявленных больных считается результатом неудачного лечения — то есть действовали факторы, приводящие к снижению системной концентрации химиопрепаратов в крови и их эффективности, одновременно «запуская» в клетках микобактерий защитные механизмы.
В структуре лекарственной устойчивости микобактерий туберкулёза различают:
- Монорезистентность — устойчивость к одному из противотуберкулёзных препаратов, чувствительность к другим препаратам сохранена. При применении комплексной терапии монорезистентность выявляют довольно редко и, как правило, к стрептомицину (в 10—15 % случаев среди впервые выявленных больных).
- Полирезистентность — устойчивость к двум и более препаратам.
- Множественная лекарственная устойчивость (МЛУ) — устойчивость к изониазиду и рифампицину одновременно (независимо от наличия устойчивости к другим препаратам). Она сопровождается, как правило, устойчивостью к стрептомицину и др. В настоящее время МЛУ возбудителей туберкулёза стала эпидемиологически опасным явлением. Расчёты показывают, что выявление возбудителей с МЛУ более чем в 6,6 % случаев (среди впервые выявленных больных) требует изменения стратегии Национальной противотуберкулёзной программы. В России, по данным мониторинга лекарственной устойчивости, частота МЛУ среди впервые выявленных больных составляет от 4 до 15 %, среди рецидивов — 45—55 %, а среди случаев неудачного лечения — до 80 %.
- Суперустойчивость — множественная лекарственная устойчивость в сочетании с устойчивостью к фторхинолонам и к одному из инъекционных препаратов (канамицин, амикацин, капреомицин). Туберкулёз, вызванный штаммами с суперустойчивостью, представляет прямую угрозу для жизни пациентов, так как остальные противотуберкулёзные препараты второго ряда не имеют выраженного эффекта. С 2006 года в некоторых странах организовано наблюдение за распространением штаммов микобактерий с суперустойчивостью. За рубежом принято обозначать этот вариант МЛУ как XDR (Extreme drug resistance).
- Перекрёстная устойчивость — когда возникновение устойчивости к одному препарату влечет за собой устойчивость к другим препаратам. У M. tuberculosis, как правило, ассоциированные с устойчивостью мутации не взаимосвязаны. Особенно часто перекрёстную устойчивость выявляют внутри одной группы препаратов, например аминогликозидов, что обусловлено одинаковой «мишенью» данной группы препаратов. В ежегодном отчете ВОЗ отмечен резкий всплеск множественной полирезистентности среди «Пекинского» («Beijing») штамма. Общемировой тенденцией является снижение эффективности антибактериальных препаратов.
На сегодняшний день основой лечения туберкулёза является поликомпонентная противотуберкулёзная химиотерапия (J04 Противотуберкулёзные препараты).
Трёхкомпонентная схема лечения[править | править вики-текст]
На заре противотуберкулёзной химиотерапии была выработана и предложена трёхкомпонентная схема терапии первой линии:
- стрептомицин
- изониазид
- пара-аминосалициловая кислота (ПАСК).
Эта схема стала классической. Она царствовала во фтизиатрии долгие десятилетия и позволила спасти жизни огромному числу больных туберкулёзом, однако на сегодняшний день исчерпала себя в виду высокой токсичности ПАСК и невозможности длительного применения стрептомицина.
Четырёхкомпонентная схема лечения[править | править вики-текст]
Одновременно в связи с повышением устойчивости выделяемых от больных штаммов микобактерий возникла необходимость усиления режимов противотуберкулёзной химиотерапии. В результате была выработана четырёхкомпонентная схема химиотерапии первой линии (DOTS — стратегия, используется при инфицировании достаточно чувствительными штаммами):
- рифампицин или рифабутин
- изониазид
- пиразинамид
- этамбутол
вместо этамбутола в схеме противотуберкулезной терапии первого ряда иногда применяется стрептомицин, а практикующееся в странах бывшего СССР применение канамицина в схеме первого ряда является недопустимым с точки зрения ВОЗ, так как его применение в таких случаях может привести к развитию устойчивых к аминогликозидам штаммов микобактерий.
Эта схема была разработана Карелом Стибло (Нидерланды) в 1980-х гг. На сегодняшний день система лечения т. н. препаратами первого ряда (включая изониазид, рифампицин, пиразинамид и этамбутол) является общепринятой в 120 странах мира, включая развитые страны.
В некоторых постсоветских странах (Россия, Украина) ряд специалистов считает стратегию DOTS недостаточно эффективной и существенно уступающей по уровню разработанной и внедрённой в СССР комплексной противотуберкулёзной стратегии, опирающейся на развитую сеть противотуберкулёзных диспансеров.[источник не указан 1599 дней]
Тем не менее, именно в странах бывшего СССР получил распространение туберкулез с множественной лекарственной устойчивостью — МЛУ, возникновение которого является результатом многолетней практики применения нестандартных схем лечения туберкулеза, а также, возможно, практикой необоснованной длительной госпитализации пациентов в противотуберкулезных стационарах, что приводит к внутрибольничному перекрестному инфицированию пациентов устойчивыми штаммами микобактерий.
Пятикомпонентная схема лечения[править | править вики-текст]
Во многих центрах, специализирующихся на лечении туберкулёза, сегодня предпочитают применять ещё более мощную пятикомпонентную схему, добавляя к упомянутой выше четырёхкомпонентной схеме производное фторхинолона, например, ципрофлоксацин. Включение препаратов второго, третьего и следующих поколений является основным при лечении лекарственноустойчивых форм туберкулёза. Режим лечения препаратами второго и следующих поколений подразумевает как минимум 20 месяцев ежедневного приёма препаратов. Данный режим гораздо дороже, чем лечение препаратами первого ряда, и составляет эквивалент примерно в 25 000 долларов США на весь курс. Существенно ограничивающим моментом также является наличие огромного количества различного рода побочных эффектов от применения препаратов второго и следующих поколений.
Если, несмотря на 4—5-компонентный режим химиотерапии, микобактерии всё же развивают устойчивость к одному или нескольким применяемым химиопрепаратам, то применяют химиопрепараты второй линии: циклосерин, капреомицин и другие, относящиеся ко второму (резервному) ряду вследствие своей токсичности для человеческого организма.
Кроме химиотерапии, большое внимание должно уделяться интенсивному, качественному и разнообразному питанию больных туберкулёзом, набору массы тела при пониженной массе, коррекции гиповитаминозов, анемии, лейкопении (стимуляции эритро- и лейкопоэза). Больные туберкулёзом, страдающие алкоголизмом или наркотической зависимостью, должны пройти детоксикацию до начала противотуберкулёзной химиотерапии.
Больным туберкулёзом, получающим иммуносупрессивные препараты по каким-либо показаниям, стремятся снизить их дозы или совсем отменить их, уменьшив степень иммуносупрессии, если это позволяет клиническая ситуация по заболеванию, потребовавшему иммуносупрессивной терапии. Больным ВИЧ-инфекцией и туберкулёзом показана специфическая анти-ВИЧ терапия параллельно с противотуберкулёзной, а также противопоказано применение рифампицина.[32]
Глюкокортикоиды в лечении туберкулёза применяют очень ограниченно в связи с их сильным иммуносупрессивным действием. Основными показаниями к назначению глюкокортикоидов являются сильное, острое воспаление, выраженная интоксикация и др. При этом глюкокортикоиды назначают на достаточно короткий срок, в минимальных дозах и только на фоне мощной (5-компонентной) химиотерапии.
Очень важную роль в лечении туберкулёза играет также санаторно-курортное лечение. Давно известно, что микобактерии туберкулёза не любят хорошей оксигенации и предпочитают селиться в сравнительно плохо оксигенируемых верхушечных сегментах долей лёгких. Улучшение оксигенации лёгких, наблюдаемое при интенсификации дыхания в разрежённом воздухе горных курортов, способствует торможению роста и размножения микобактерий. С той же целью (создания состояния гипероксигенации в местах скопления микобактерий) иногда применяют гипербарическую оксигенацию и др.
Сохраняют своё значение и хирургические методы лечения туберкулёза: в запущенных случаях может оказаться полезным наложение искусственного пневмоторакса и пневмоперитонеума, удаление поражённого лёгкого или его доли, дренирование каверны, эмпиемы плевры и др. Однако безусловным и важнейшим действенным средством является химиотерапия — терапия противотуберкулёзными препаратами, гарантирующими бактериостатический, бактериолитический эффекты, без которых невозможно достижение излечения от туберкулёза.
Прогноз[править | править вики-текст]
Прогноз заболевания во многом зависит от стадии, локализации заболевания, лекарственной устойчивости возбудителя и своевременности начала лечения, однако в целом является условно неблагоприятным[33][данные по источнику 1967 года]. Заболевание без усиленного диетического питания, благоприятных социально-гигиенических условий, климатолечения плохо поддаётся химиотерапии, особенно это касается туберкулёза с множественной лекарственной устойчивостью и широкой лекарственной устойчивостью, а хирургическое лечение зачастую является симптоматическим или паллиативным. Трудоспособность во многих случаях стойко утрачивается, и даже при сохранённой после излечения трудоспособности существует запрет на трудовую деятельность подобных лиц по целому ряду декретированных профессий, таких как учителя младших классов, воспитатели детских садов, сотрудники пищевой промышленности или коммунальных служб и т. п. Своевременно начатое лечение позволяет добиться полного восстановления трудоспособности, однако не гарантирует невозможность рецидива заболевания. При несвоевременной диагностике или неаккуратном лечении происходит инвалидизация пациента, зачастую в итоге приводящая к его смерти.
В произведениях искусства[править | править вики-текст]
|
|
Список примеров в этой статье или её разделе не основывается на авторитетных источниках непосредственно о предмете статьи или её разделе.
Добавьте ссылки на источники, предметом рассмотрения которых является тема настоящей статьи (раздела) в целом, и содержащие данные элементы списка как примеры. В противном случае раздел может быть удалён. |
Тема туберкулёза активно поднималась в классической художественной литературе.
От туберкулёза, несмотря на смерть от этой болезни матери и первой жены писателя, излечивается герой рассказа О. Генри «Санаторий на ранчо». Благодаря повышающему иммунитет альтруизму, впрочем, характерному и для большинства умерших от туберкулёза благородных героев литературы XIX — начала XX века, излечивается Рашель — героиня рассказа Ги де Мопассана «Мадемуазель Фифи», одноимённой оперы Цезаря Кюи и оперы «Рашель» Р. М. Глиэра и М. А. Булгакова (либретто оперы, ставшей завещанием врача и писателя М. А. Булгакова, закончено Маргаритой Алигер).
Туберкулёзом страдают и от туберкулёза умирают герои романов М. Ю. Лермонтова («Герой нашего времени»), И. С. Тургенева («Накануне»), Бальзака («Шагреневая кожа»), Виктора Гюго («Отверженные»), А. Мюрже («Сцены из жизни богемы»), Чарльза Диккенса, Дюма-сына («Дама с камелиями»), Ремарка («Три товарища», «Жизнь взаймы», «Ночь в Лиссабоне»), трагедии Эдмона Ростана «Орлёнок», повести В. Г. Короленко «Дети подземелья», повести А. И. Куприна «Яма», его рассказа «Сентиментальный роман», оперы Джузеппе Верди «Травиата», опер Леонкавалло и Пуччини «Богема» и др.
Переживаниям больных туберкулёзом, в том числе последней стадии, много внимания под впечатлением личных переживаний или семейной трагедии уделяли реалисты Достоевский («Идиот», «Преступление и наказание»), Толстой («Анна Каренина», «Воскресение»), Чехов. Действие романов «Волшебная гора» Томаса Манна и «Санаторий» Сомерсета Моэма разворачиваются в стенах туберкулёзных санаториев.
В современной российской литературе тема туберкулёза продолжена в романе Тимофея Фрязинского «Венера туберкулёза»[34] (изд-во Ad Marginem), в котором описывается моральная составляющая жизни с этой болезнью и жёсткие будни той среды, где туберкулёз является нормой.
В мюзикле «Мулен Руж» главная героиня умирает от туберкулеза.
В аниме Хаяо Миядзаки «Ветер крепчает» в конце фильма главная героиня Наоко Сатоми умирает от туберкулёза.
Об ущербной пользе туберкулёза[править | править вики-текст]
|
|
Список примеров в этой статье или её разделе не основывается на авторитетных источниках непосредственно о предмете статьи или её разделе.
Добавьте ссылки на источники, предметом рассмотрения которых является тема настоящей статьи (раздела) в целом, и содержащие данные элементы списка как примеры. В противном случае раздел может быть удалён. |
Туберкулёзом болели многие выдающиеся таланты — Спиноза, Н. Х. Абель, Чокан Валиханов, В. И. Вернадский, Н. М. Амосов, Шиллер, Франц Кафка, Джон Китс, сёстры Бронте, Роберт Льюис Стивенсон, Джордж Оруэлл, Эдит Сёдергран, Альбер Камю, Йозеф Гайдн, Никколо Паганини, Фредерик Шопен, Карл Мария фон Вебер, Стравинский, С. Я. Лемешев, Рашель, Сара Бернар, Ж. П. Бельмондо, Рафаэль, П. З. Захаров, Ф. А. Васильев, Исаак Левитан, М. К. Башкирцева, Б. М. Кустодиев, Н. Б. Северова (Нордман), П. Я. Чаадаев, В. Г. Белинский, Н. А. Добролюбов, Алексей Кольцов, А. И. Полежаев, И. С. Никитин, Н. А. Некрасов, К. С. Аксаков, Ф. М. Достоевский, С. Надсон, Шолом Алейхем, А. П. Чехов, Максим Горький, Александр Куприн, Габдулла Тукай, Михаил Коцюбинский, Леся Украинка, Александр Грин, Илья Ильф, Анна Ахматова — и многие другие. Генрик Сенкевич создал специальный фонд для помощи больным туберкулёзом литераторам.
Биолог В. П. Эфроимсон, увлекавшийся поиском биологических и биохимических предпосылок гениальности человека, отметил (в том числе в своей книге «Генетика гениальности»), что некоторые заболевания, при всех своих известных минусах, способствуют либо повышенному возбуждению и беспрестанной деятельности головного мозга (например, подагра), либо снижению чувства усталости, при отсутствии которого человек продолжает в том числе умственную работу более длительное время. Последнее характерно как раз для ранних стадий туберкулёза. В названной работе приводится целый ряд примеров известных исторических деятелей и учёных в подтверждение данного предположения.
Примечания[править | править вики-текст]
- ↑ 1 2 Kumar, Vinay; Abbas, Abul K.; Fausto, Nelson; & Mitchell, Richard N. Robbins Basic Pathology. — 8th. — Saunders Elsevier, 2007. — P. 516–522. — ISBN 978-1-4160-2973-1.
- ↑ Konstantinos, A (2010). «Testing for tuberculosis». Australian Prescriber, 33:12-18. http://www.australianprescriber.com/magazine/33/1/12/18/
- ↑ al.] edited by Peter G. Gibson ; section editors, Michael Abramson … [et Evidence-based respiratory medicine. — 1. publ.. — Oxford: Blackwell, 2005. — P. 321. — ISBN 978-0-7279-1605-1.
- ↑ Jasmer RM, Nahid P, Hopewell PC (December 2002). «Clinical practice. Latent tuberculosis infection». N. Engl. J. Med. 347 (23): 1860–6. DOI:10.1056/NEJMcp021045. PMID 12466511.
- ↑ 1 2 Tuberculosis. World Health Organization (2007). Проверено 12 ноября 2009. Архивировано из первоисточника 24 августа 2011. Fact sheet No 104.
- ↑ 1 2 World Health Organization The Stop TB Strategy, case reports, treatment outcomes and estimates of TB burden // Global tuberculosis control: epidemiology, strategy, financing. — 2009. — P. 187–300. — ISBN 978 92 4 156380 2.
- ↑ http://medi.ru/doc/9590305.htm Большой Целевой Журнал о туберкулёзе «» № 3 1999 Основы. К проблеме вакцинации BCG
- ↑ Факторы риска развития заболевания туберкулезом у детей и подростков из социально-дезадаптированных групп населения
- ↑ ЕРБ ВОЗ | Европейские государства-члены демонстрируют новую решимость в борьбе с лекарственно-устойчивыми формами туберкулеза
- ↑ Вторичный туберкулез
- ↑ W. Devitt Indications for Pneumothorax. Chest. 1936;2;8—26
- ↑ WHO Disease and injury country estimates. World Health Organization (2004). Проверено 11 ноября 2009. Архивировано из первоисточника 20 августа 2011.
- ↑ National Institute of Allergy and Infectious Diseases (NIAID). Microbes in Sickness and in Health. 26 October 2005. Retrieved on 3 October 2006. „According to the World Health Organization (WHO), nearly 2 billion people, one-third of the world’s population, have TB.“
- ↑ Centers for Disease Control. Fact Sheet: Tuberculosis in the United States. (недоступная ссылка с 21-05-2013 (663 дня) — история, копия) 17 March 2005, Retrieved on 6 October 2006.
- ↑ World Health Organization (WHO). Global Tuberculosis Control Report, 2006 (недоступная ссылка с 21-05-2013 (663 дня) — история, копия) — Annex 1 Profiles of high-burden countries. (PDF) Retrieved on 13 October 2006.
- ↑ Centers for Disease Control and Prevention (CDC). 2005 Surveillance Slide Set. (September 12, 2006) Retrieved on 13 October 2006.
- ↑ Davies PDO, Yew WW, Ganguly D, et al. (2006). «Smoking and tuberculosis: the epidemiological association and pathogenesis». Trans R Soc Trop Med Hyg 100: 291–8. PMID 16325875.
- ↑ Restrepo BI (2007). «Convergence of the tuberculosis and diabetes epidemics: renewal of old acquaintances». Clin Infect Dis 45: 436–8.
- ↑ Туберкулёз в России. Справка. РИА Новости (24 марта 2010). Проверено 14 августа 2010. Архивировано из первоисточника 24 августа 2011.
- ↑ Бремя туберкулеза в России // Демоскоп Weekly 11 декабря 2011 «смертность от туберкулеза составляет около 70 % всех случаев, приходящихся на инфекционные и паразитарные болезни в России. «
- ↑ Минздрав РФ (недоступная ссылка с 21-05-2013 (663 дня) — история, копия)
- ↑ Туберкулёз. Лечение. Симптомы. Профилактика. Диагностика (фото+видео)» (недоступная ссылка с 21-05-2013 (663 дня) — история, копия)
- ↑ Туберкулёз. Оценка ситуации | Медицинская газета «Здоровье Украины», Медицинское издание, медицинские издательства на Украине
- ↑ Organització Mundial de la Salut (OMS). Global tuberculosis control — surveillance, planning, financing WHO Report 2006. Consultat el 13 d’octubre del 2006.
- ↑ Справочник по клинической хирургии / Под ред. проф. В. И. Стручкова. — М.: «Медицина», 1967. — 520 с.
- ↑ Список знаменитых людей, умерших от туберкулёза
- ↑ Ортопедическая диагностика. Плечевой пояс и плечевой сустав.
- ↑ Вакцина БЦЖ. Еженедельный эпидемиологический бюллетень ВОЗ (январь 2004). Проверено 7 ноября 2014.
- ↑ Н.Г. Камаева и др. Клинико-эпидемиологические особенности туберкулезных оститов у детей, вакцинированных БЦЖ 16-20. Проблемы туберкулеза и болезней легких (2009). Проверено 7 ноября 2014.
- ↑ Р.Я. Мешкова. Руководство по иммунопрофилактике для врачей. Проверено 7 ноября 2014.
- ↑ Витамин B6: фармакодинамика и фармакокинетика
- ↑ М. И. Перельман Консультант врача. Фтизиатрия. — М.: ГЭОТАР-Медиа, 2007. — С. 57-65. — ISBN 978-5-9704-1234-3.
- ↑ Проф. А. И. Арутюнов, кандидат медицинских наук Н. Я. Васин и В. Л. Анзимиров Справочник по клинической хирургии / Проф. В.И. Стручкова. — Москва: Медицина, 1967. — С. 234. — 520 с. — 100 000 экз.
- ↑ Тимофей Фрязинский «Венера туберкулёза». admarginem.ru. Проверено 10 ноября 2010. Архивировано из первоисточника 24 августа 2011.
Литература[править | править вики-текст]
- Перельман М. И., Корякин В. А., Богадельникова И. В. Фтизиатрия. ОАО Издательство «Медицина», 2004.
- Руководство по лечению лекарственно-устойчивых форм туберкулёза. Издание ВОЗ.
- Сайт ВОЗ. Руководство по программному ведению лекарственно-устойчивого туберкулёза
- Туберкулёз. Вопросы и ответы. Всемирная организация здравоохранения
- Факты о туберкулёзе. Сайт Всемирной организации здравоохранения
Ссылки[править | править вики-текст]
| Туберкулёз на Викискладе? |
- Туберкулёз/ВИЧ: Клиническое руководство на сайте ВОЗ
- Центральный НИИ Туберкулёза РАМН г. Москва
- Как защитить себя от туберкулёза
- Фильм о диагностике, лечении и профилактике туберкулёза
- Новая эффективная диагностика туберкулёза
- Новая вакцина H56 способна бороться с латентной туберкулезной инфекцией
- Туберкулёз в России
- Туберкулез: что это? Учебное видео — инфографика о туберкулезе
- Туберкулез среди подростков и молодежи в России. Доклад (2011 г.)
С появлением антибиотиков человеку удалось взять под контроль такое распространенное и опасное инфекционное заболевание, как туберкулез (старое название – чахотка). Тем не менее оно продолжает оставаться в списке глобальных угроз человечеству и в XXI веке.
В России каждый год регистрируется все меньше новых случаев болезни, и уровень смертности от нее продолжает снижаться. Однако ситуация все еще сложная. ВОЗ сообщает, что за 2018 год в РФ заболели туберкулезом 79 тысяч, а умерли – 10 тысяч человек. Мало того, инфекция бросает новый вызов человечеству: появились особые формы заболевания, стойкие к существующим лекарствам. В России число таких случаев достигает 9 %. По этому показателю она занимает третье место в мире после Индии и Китая. Необходимое лечение в стране получают 99 % всех больных туберкулезом, однако полностью излечиваются только 69 %. Сложная ситуация наблюдается также в Азербайджане, Беларуси, Казахстане, Кыргызстане, Молдове, Таджикистане, Узбекистане, Украине.
Что такое туберкулез, возбудитель болезни
- Туберкулезом называют хроническое инфекционное бактериальное заболевание, вызванное возбудителем Mycobacterium tuberculosis complex (в народе более известном как палочка Коха).
- Впервые этот микроорганизм выделил немецкий ученый Роберт Кох в 1882 году, но сам недуг известен очень давно. Следы микобактерий туберкулеза исследователи находили даже в останках древнеегипетских мумий.
- Эти микроорганизмы отличаются высокой жизнестойкостью в окружающей среде. Во влажном и темном месте при температуре 23 °C они могут сохраняться до 7 лет, в темном и сухом – до 10–12 месяцев, в сухом и светлом – около 2 месяцев.
- В воде палочка живет до 5 месяцев, в почве – до 6 месяцев, в сыром молоке – до 2 недель, в сыре и масле – около года, на страницах книг – около 3 месяцев. Однако эти бактерии погибают при воздействии веществ, содержащих хлор, третичных аминов, перекиси водорода, а также при облучении ультрафиолетом. Они могут принимать малоопасные L-формы, которые присутствуют в организме человека, но не вызывают острого процесса.
Стадии заболевания
Существует три стадии развития туберкулеза:
- первичная;
- латентная;
- активная.
Также различают открытую и закрытую формы. В первом случае болезнь явно выражена, бактерии легко обнаруживаются в мокроте, каловых массах, а сам больной представляет опасность для окружающих в плане инфицирования. Закрытая форма неопасна для окружающих. Чаще всего встречается туберкулез легких, но эта инфекция может также поражать кости, суставы, мочеполовую систему, кишечник, брюшину, мозговые оболочки, ЦНС, периферические лимфоузлы, кожу (золотуха).
Первичное инфицирование
Заражение происходит, когда бактериям удается пройти сквозь защитные барьеры и проникнуть глубоко в легкие. Если верхние дыхательные пути здоровые и работают правильно, им удается задержать и вывести со слизью большую часть палочек Коха и других опасных бактерий. В теории для инфицирования людей со слабым иммунитетом достаточно одной палочки, но для более стойких организмов все же требуется многоразовый контакт.
Далее бактерии поглощаются альвеолярными макрофагами. Необезвреженные возбудители начинают воспроизводиться, возникает локальное воспаление в области проникновения инфекции. Через ближайшие лимфоузлы зараженные макрофаги попадают в кровь, проникая в другие органы. Но если у человека сформирован хотя бы частичный иммунитет, распространение через кровоток маловероятно.
Латентная инфекция
Через три недели активного роста бактерий примерно в 95 % случаев, иммунная система подавляет их рост и размножение. Тогда очаги с микробами в пораженных органах превращаются в эпителиоидные гранулемы. В них туберкулезные палочки могут жить много лет, человек при этом чувствует себя вполне здоровым, клинических проявлений болезни также не наблюдается. Если иммунитет достаточно сильный, инфекция так и остается в неактивной форме. Считается, что у почти одной трети населения мира присутствует латентный туберкулез, но эти люди не представляют угрозу для окружающих, потому что не выделяют бактерии. Однако сбои в работе иммунной системы могут привести к обострению процесса. Бывает, что первичное поражение начинает прогрессировать сразу. В группе риска – маленькие дети и лица с очень слабым иммунитетом.
Активная стадия
Туберкулез у взрослых людей переходит в активную фазу в течение двух лет с момента заражения, но нередко он проявляется и через десятилетия. Этому способствует снижение клеточного иммунитета. Больше всего в этой связи уязвимы люди с ВИЧ инфекцией, не получающие антиретровирусной терапии. Также в группе риска находится еще ряд пациентов:
- с сахарным диабетом;
- с раком головы и шеи;
- с болезнями почек, которым назначен диализ;
- перенесшие операцию по резекции желудка;
- принимающие препараты, которые подавляют иммунную систему (после трансплантации органов).
Фактором риска также считается курение и недостаточное питание, поэтому эта инфекция нередко встречается у лиц, ведущих асоциальный образ жизни. При отсутствии лечения ткани поврежденного болезнью органа распадаются, образуются множественные каверны (изолированные полости в легких).
Формы туберкулеза:
- туберкулема;
- латентный;
- очаговый (ограниченный);
- милиарный;
- инфильтративный;
- диссеминированный;
- кавернозный;
- фиброзно-кавернозный;
- цирротический;
- казеозная пневмония.
Как передается туберкулез
Главным источником инфекции являются люди с болезнью в открытой форме. Пути передачи возбудителя:
- воздушно-капельный – при чихании и кашле бактерии оказываются в воздухе, который вдыхают здоровые люди. Кроме того, микроорганизмы оседают в пыли и долго там сохраняются;
- алиментарный – через употребление в пищу зараженных продуктов – молока, яиц и проч. Однако в этом случае требуется большее количество бактерий в сравнении с воздушно-капельным путем;
- контактный – при прямом соприкосновении поврежденной кожи со здоровой или через конъюнктиву глаза, но подобное отмечается редко;
- в период внутриутробного развития от матери – плод инфицируется через плаценту, но это также происходит нечасто.
Симптомы, клинические проявления
На ранних стадиях туберкулез протекает практически бессимптомно. По мере его развития состояние больного ухудшается, однако специфическая симптоматика не наблюдается. Клинические признаки – повышенная усталость, слабость, резкое снижение веса без видимых на то причин, температура 37-38 °С, не спадающая продолжительное время, ночная потливость. Лицо становится бледным, а на щеках появляется румянец. У детей туберкулез прогрессирует намного быстрее, чем у взрослых, в силу неразвитой иммунной системы.
Легочную форму туберкулеза сопровождает кашель. Вначале он несильный, но со временем его интенсивность возрастает. Если он продолжается больше трех недель, следует немедленно обратиться к врачу. Кашель вначале сухой, приступообразный, особенно ночью и утром. Позже начинает выделяться желто-зеленая мокрота, а на стадии каверн наблюдается кровохаркание.
При туберкулезе мозговых оболочек и головного мозга к симптомам общей интоксикации добавляются расстройства сна, головные боли, интенсивность которых постепенно усиливается. Затем проявляется ригидность затылочных мышц, симптомы Кернига и Брудзинского, неврологические расстройства.
Симптоматика туберкулеза органов пищеварения схожа с другими болезнями этого отдела: диспепсия, боль в животе, позже – кровь в кале. Поражение костей и суставов проявляет себя так же, как и артриты, почек – имеет симптомы нефрита: боль в спине, кровь в моче. При туберкулезе кожи наблюдаются плотные узелки под эпидермисом, которые увеличиваются и прорываются с выделением творожистой массы.
Диагностика туберкулеза
Из-за того, что болезнь на начальных стадиях не проявляет себя, особое внимание уделяют профилактическим обследованиям. Для этого взрослые каждый год проходят флюорографию грудной клетки, а детям делают пробу Манту (туберкулиновую) или диаскинтест, направленные на выявление степени инфицированности организма туберкулезной палочкой и реактивность тканей. Есть также альтернативные исследования крови: T-SPOT тест и квантиферон-тест. Рентгенография позволяет выявить инфекцию не только в легких, а и в других органах. В случае необходимости проводят КТ.
Но окончательный диагноз ставят по итогам исследования биологических сред. Делают посев мокроты, промывных вод бронхов и желудка, а также масс, отделяемых от кожи. В отдельных случаях выполняют бронхоскопию с биопсией, а также биопсию лимфоузлов.
Лечение туберкулеза, прогнозы
- Своевременно выявленный туберкулез поддается лечению антибиотиками. Обычно назначают 4-5 препаратов, которые следует принимать строго по назначенной врачом схеме.
- Есть медикаменты первого ряда, наиболее эффективные, и лекарства второго ряда, резервные. При подозрении на болезнь врачи могут назначить 1-2 препарата для профилактики.
- Обычно положительных результатов добиваются за полгода активного лечения. За этот период очаги инфекции заживают, исчезают симптомы, болезнь переходит в закрытую форму.
- Больных с открытой формой помещают в туберкулезный диспансер. Там до прекращения выделения бактерий ими занимаются врачи-фтизиатры. Но полное исцеление занимает около года, а порой на это требуется и больше времени.
- Помимо медикаментозного лечения больным рекомендуется делать дыхательную гимнастику, укреплять иммунитет, проходить физиотерапию.
- Важно полноценно питаться, включать в рацион мясо, фрукты, овощи, кисломолочные продукты, исключить алкоголь и табак.
- В период выздоровления рекомендуется продолжить лечение в специализированных санаториях.
- В отдельных случаях показано хирургическое вмешательство. Этот метод чаще всего применяется при кавернозной форме туберкулеза легких, когда врачам приходится удалять сильно пораженную часть органа.
При своевременной диагностике и правильной терапии болезнь излечима. Но на пораженных участках могут оставаться рубцы и инкапсулированные очаги, в которых бактерии пребывают в неактивном состоянии. При снижении иммунитета возможен рецидив, поэтому все пациенты должны находиться на диспансерном учете и регулярно обследоваться. При этом туберкулиновая проба будет давать положительный результат даже после полного излечения.
При отсутствии терапии смертность от туберкулеза составляет 50 %.
Туберкулез при беременности
Беременность может активировать дремавший в организме возбудитель туберкулеза, при этом чаще всего заболевание протекает более остро. Применяемые сегодня для лечения туберкулеза антибиотики в принципе не вызывают отклонений в развитии плода, однако принимать их на ранних сроках все равно не рекомендуется. Врачам, лечащим туберкулез, приходится подбирать щадящую терапию. Течение беременности осложняется туберкулезной интоксикацией, поэтому ребенок нередко рождается с малым весом и раньше срока. Если болезнь проявляется на ранних сроках беременности впервые, и мать ранее не получала лечения, младенец появляется на свет с врожденным туберкулезом. Кормление грудью разрешается, если у матери болезнь находится в неактивной стадии. Планирование беременности целесообразно не раньше, чем через 2-3 года после выздоровления.
Резистентный туберкулез
Для терапии туберкулеза применяют антибактериальные препараты. Но микобактерии обладают свойством быстро мутировать и образовывать множество генотипов с устойчивостью к некоторым медикаментам. Поэтому пациентам назначают одновременно несколько разных лекарственных средств.
Различают первично-резистентный и вторично-резистентный туберкулез. Первый возникает, когда устойчивый к антибиотикам штамм находят у больных, ранее вообще не принимавших специфические средства. Второй проявляется у пациентов, либо прервавших терапию самостоятельно, либо проходящих неправильно спланированный курс лечения.
Микобактерии могут быть нечувствительными к одному лекарственному средству, но случается и полирезистентный туберкулез, при котором штамм устойчив сразу к нескольким препаратам. ВОЗ сообщат, что 490 тыс. больных туберкулезом в мире имеют форму с множественной медикаментозной устойчивостью.
Для предотвращения развития резистентности больным назначают не меньше двух препаратов, а на первом этапе – даже четырех. Важно также полностью завершить назначенный курс лечения, ни в коем случае не пропускать прием лекарств.
Профилактика
Профилактика туберкулеза начинается еще в грудном возрасте. На 4-й день жизни ребенка ему делают прививку БЦЖ, представляющую собой ослабленный штамм микобактерий. Поскольку возбудители очень активны в отношении детей, очень важно выработать иммунитет как можно раньше. Для недоношенных младенцев разработан более слабый вариант вакцины – БЦЖ-М. В норме в месте укола появляется бугорок, а потом пузырек с желтоватой жидкостью, который позже лопается и покрывается коркой. Вакцина не защищает от туберкулеза полностью, однако позволяет избежать внелегочной инфекции у детей.
Важно также вести здоровый образ жизни, хорошо питаться, не курить, регулярно проходить обследования. Туберкулезом может заболеть любой человек, даже из вполне благополучных слоев общества. Запускают механизм развития болезни сбои в работе иммунной системы.
Туберкулез (устаревшее название — чахотка) — тяжелое, но излечимое инфекционное заболевание. Его трудно выявить, оно наносит серьезные повреждения организму, а потому смертельно опасно. Заражение происходит достаточно легко, однако своевременное обращение за медицинской помощью делают полное выздоровление абсолютно реальным.

Общая информация
Всемирная организация здравоохранения сообщает, что туберкулезом инфицирован каждый третий житель планеты. Однако быть инфицированным — не значит болеть чахоткой. Примерно у 8-9 млн людей в год заболевание переходит в активную форму, а смертность от туберкулеза составляет 3 млн человек в год.
Что же вызывает болезнь: вирус или бактерия? Туберкулез — невирусное заболевание. Его возбудитель — палочка Коха — микробактерия.
Палочки Коха имеют ряд особенностей, именно они делают болезнь чрезвычайно заразной:
- Микробы устойчивы к спирту, щелочи, кислотам.
- Не погибают под воздействием низких температур.
- Усиленно размножаются во влажной среде, в темных, невентилируемых помещениях.
- Быстро распространяются по воздуху: во время разговора — на 70 см и дальше, при кашле — на 3 м.
- Вне организма живут четыре месяца, в воде — почти полгода.
- Устойчивы ко многим лекарственным препаратам.
Бактерии погибают в тепле, не переносят солнечные лучи, хлорсодержащие вещества.

Развитие
С момента попадания палочки Коха в организм и до появления первых признаков заболевания могут пройти даже годы. Все зависит от состояния иммунной системы человека. Сильная — убивает бактерию, поэтому болезнь не развивается. Слабая сдается почти сразу, инкубационный период в этом случае очень короткий. Если иммунитет не в состоянии уничтожить возбудителя, но и не дает ему распространиться, болезнь становится скрытой (латентной). Любой сбой в работе иммунитета даст толчок к развитию активной формы.
Лучшая защита от туберкулеза — своевременная вакцинация. В Российской Федерации БЦЖ делают в роддоме всем здоровым новорожденным. Если необходимо, проводят ревакцинацию, когда ребенку исполняется 7 и 14 лет. Взрослый может защитить себя, не пропуская профилактические медосмотры и флюорографические исследования, которые позволяют выявить заболевание на ранней стадии.
Виды и формы туберкулеза
Самым распространенным считается туберкулез легких. Однако болезнь может поразить любой орган или систему органов.
Выявляют туберкулез:
- лимфоузлов;
- пищеварительной системы;
- нервной системы;
- мочеполовой;
- костей и суставов.
Заболевание бывает первичным (развивается сразу после проникновения в клетку палочки Коха) и вторичным (после заражения другим типом микобактерии или смены ремиссии обострением). Вторичный тип чаще встречается у взрослых пациентов.
По отношению к выделению бактерий различают открытую форму (больные выделяют возбудителя в окружающую среду) и закрытую (выделения не происходит).
Есть особая форма туберкулеза — туберкулома. В легких образуются некротические очаги, окруженные фиброзной капсулой. Болезнь не дает симптомов, ее может выявить только рентгенография или специальные анализы. Часто развивается у людей с сахарным диабетом и нарушениями обмена веществ.

Причины развития туберкулеза
Основной путь передачи инфекции — воздушно-капельный. Она распространяется с частицами слюны носителя при разговоре, кашле, чихании, пении. Больной с открытой формой туберкулеза за год в среднем заражает более 10 человек. Реже бактерии передаются воздушно-пылевым путем, через предметы обихода. Заражение также происходит через продукты питания: мясо, молоко животных, болеющих туберкулезом.
Риск заболеть высок у тех, кто:
- находится в плотном контакте с больным человеком;
- проживает в регионе с высоким уровнем заболеваемости;
- страдает ВИЧ, сахарным диабетом, другими заболеваниями, снижающими иммунитет;
- длительно принимал лекарственные препараты, ослабляющие иммунную систему (кортикостероиды, цитостатики и др.);
- плохо питается;
- употребляет алкоголь, наркотические вещества;
- проживает в неблагоприятных условиях (тюрьма, ночлежка).
Фактором риска считается также детский или пожилой возраст, так как иммунитет у детей и пожилых обычно слабее, чем у взрослых.

Симптомы туберкулеза легких
Первые признаки заболевания — слабость и кашель, которые не исчезают в течение трех недель. Немного позднее в мокроте появляется кровь, возникает боль при дыхании, так как ткани легких начинают разрушаться. Наличие этих признаков требует безотлагательного обращения к врачу.
К симптомам туберкулеза также относят:
- субфебрилитет;
- внезапная потеря веса, аппетита;
- перепады настроения;
- усиление потоотделения, особенно в ночное время;
- одышка;
- тахикардия;
- увеличение лимфатических узлов.
Больной выглядит уставшим, его черты лица заостряются, на щеках появляется нездоровый румянец. На первой стадии болезни общий анализ крови не покажет разительных изменений, кроме снижения количества лейкоцитов и уровня гемоглобина.

Диагностика
Своевременная диагностика туберкулезной инфекции очень важна. Чем раньше человек узнает о ней, тем быстрее сможет вылечиться и меньшее количество людей заразит. Поэтому обязательный скрининг на туберкулез легких прописан на законодательном уровне.
Для детей это ежегодная проба Манту — введение под кожу микроскопической дозы туберкулина PPD (очищенного экстракта белков палочки Коха). После введения экстракта на коже проявляется реакция — «пуговка» — уплотнение с покраснением. По ее размеру судят о том, как часто организм сталкивается с искомой бактериальной инфекцией, как на нее реагирует иммунитет. При подозрении на туберкулез пробу Манту делают и взрослым.
С 15-летнего возраста раз в два года проходят флюорографическое обследование. Врачам, работникам пищевой промышленности, учителям, военным и некоторым другим группам населения такое исследование нужно проводить 1 раз в год. Рентгеновский снимок покажет, есть ли изменения в легких. Также регулярно на профосмотрах сдается общий анализ крови.
При подозрении на туберкулез человека направляют к фтизиатру. К доктору необходимо обратиться самостоятельно, если вы были в тесном контакте с инфицированным.
Наиболее информативный анализ, позволяющий быстро разобраться, есть ли у пациента туберкулез (даже в латентной форме) — анализ крови на секрецию гамма-интерферона. Исследование показано, когда рентген делать нельзя (беременность, патологии щитовидной железы, почек, печени и т.д.), а проба Манту малоинформативна.
Врач обязательно назначит анализ мокроты. Он покажет, присутствуют ли в ней микобактерии. Если да — это признак открытой формы туберкулеза легких.

Лечение
Если не лечить туберкулез, это может привести к смерти. При отсутствии терапии или несоблюдении врачебных рекомендаций смертность составляет 50%. Однако правильно пройденный курс лечения практически полностью исключает смертельные исходы.
Терапия не требует госпитализации, проводится в домашних условиях. В зависимости от состояния, больному назначается режим:
- постельный, если состояние тяжелое, есть осложнения;
- ограниченный (покой, отсутствие физических нагрузок) при самочувствии средней тяжести;
- общий, когда состояние улучшается.
Прием лекарств
Нужно принимать курс антибиотиков (несколько видов) в течение полугода (иногда дольше). Продолжительность приема зависит от формы, стадии заболевания, наличия сопутствующих патологий. Так, внелегочная форма лечится примерно теми же лекарствами, только гораздо дольше.
Уже через две недели после начала лечения больные начинают чувствовать себя лучше. Однако курс необходимо закончить. Если прекратить прием антибиотиков раньше, микобактерии разовьют к ним устойчивость. Тогда длительность и сложность лечения увеличатся в разы.
Примерно пятая часть всех случаев заболевания требует хирургического лечения. Внутрилегочное кровотечение может полностью заблокировать дыхательную систему.

Латентная форма
Лечить латентную форму рекомендуется в тех случаях, когда есть риск ее перехода в активную, а также позволяет возраст. После 35 лет усиливается уязвимость печени — побочные эффекты лечения могут перевесить его преимущества.
После выздоровления больные находятся под наблюдением фтизиатра еще три года. Они проходят регулярные обследования, узнают, на что необходимо обращать внимание, чтобы не допустить рецидива болезни.
Помните, что подавляющее большинство случаев чахотки у взрослых и детей может быть излечено. Главные условия для этого — наличие медикаментов и их добросовестный прием.