Как правильно пишется слово «вазэктомия»
Нет информации о правописании.
Делаем Карту слов лучше вместе

Привет! Меня зовут Лампобот, я компьютерная программа, которая помогает делать
Карту слов. Я отлично
умею считать, но пока плохо понимаю, как устроен ваш мир. Помоги мне разобраться!
Спасибо! Я стал чуточку лучше понимать мир эмоций.
Вопрос: приспеть — это что-то нейтральное, положительное или отрицательное?
Синонимы к слову «вазэктомия»
Предложения со словом «вазэктомия»
- Этих людей отвезли в мусоровозах в местную клинику, где во время вазэктомии их держали крепкие санитары.
- После того как у него родились близнецы, он сделал вазэктомию: у него не будет больше детей.
- Она знала: устранение результатов вазэктомии – это не просто физиологическая процедура.
- (все предложения)
Отправить комментарий
Дополнительно
Смотрите также
-
Этих людей отвезли в мусоровозах в местную клинику, где во время вазэктомии их держали крепкие санитары.
-
После того как у него родились близнецы, он сделал вазэктомию: у него не будет больше детей.
-
Она знала: устранение результатов вазэктомии – это не просто физиологическая процедура.
- (все предложения)
- миорелаксант
- иммунотерапия
- трансфузия
- рентгенотерапия
- суппозиторий
- (ещё синонимы…)
- сделать вазэктомию
- (полная таблица сочетаемости…)
| В Википедии есть статья «вазэктомия». |
Содержание
- 1 Русский
- 1.1 Морфологические и синтаксические свойства
- 1.2 Произношение
- 1.3 Семантические свойства
- 1.3.1 Значение
- 1.3.2 Синонимы
- 1.3.3 Антонимы
- 1.3.4 Гиперонимы
- 1.3.5 Гипонимы
- 1.4 Родственные слова
- 1.5 Этимология
- 1.6 Фразеологизмы и устойчивые сочетания
- 1.7 Перевод
- 1.8 Библиография
Русский[править]
| В Викиданных есть лексема вазэктомия (L94420). |
Морфологические и синтаксические свойства[править]
| падеж | ед. ч. | мн. ч. |
|---|---|---|
| Им. | вазэктоми́я | вазэктоми́и |
| Р. | вазэктоми́и | вазэктоми́й |
| Д. | вазэктоми́и | вазэктоми́ям |
| В. | вазэктоми́ю | вазэктоми́и |
| Тв. | вазэктоми́ей вазэктоми́ею |
вазэктоми́ями |
| Пр. | вазэктоми́и | вазэктоми́ях |
ва—зэк—то—ми́·я
Существительное, неодушевлённое, женский род, 1-е склонение (тип склонения 7a по классификации А. А. Зализняка).
Корень: —.
Произношение[править]
- МФА: [vəzɛktɐˈmʲiɪ̯ə]
Семантические свойства[править]
Значение[править]
- мед. хирургическая операция, при которой производится перевязка или удаление фрагмента семявыносящих протоков у мужчин (самцов) ◆ Отсутствует пример употребления (см. рекомендации).
Синонимы[править]
- мужская стерилизация
Антонимы[править]
Гиперонимы[править]
- хирургическая операция, стерилизация
Гипонимы[править]
Родственные слова[править]
| Ближайшее родство | |
Этимология[править]
Происходит от ??
Фразеологизмы и устойчивые сочетания[править]
Перевод[править]
| Список переводов | |
|
Библиография[править]
|
|
Для улучшения этой статьи желательно:
|
| Vasectomy | |
|---|---|
 |
|
| Background | |
| Type | Sterilization |
| First use | 1899 (experiments from 1785)[1] |
| Failure rates (first year) | |
| Perfect use | 0.10%[2] |
| Typical use | 0.15%[2] «Vas-Clip» nearly 1% |
| Usage | |
| Duration effect | Permanent |
| Reversibility | Possible |
| User reminders | Two consecutive negative semen specimens required to verify no sperm. |
| Clinic review | All |
| Advantages and disadvantages | |
| STI protection | No |
| Benefits | No need for general anesthesia. Lower cost and less invasive than tubal ligation for females. |
| Risks | Temporary local inflammation of the testes, long-term genital pain. |
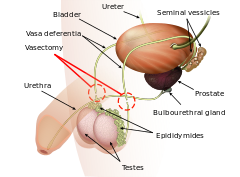
Vasectomy, or vasoligation, is an elective surgical procedure for male sterilization or permanent contraception. During the procedure, the male vasa deferentia are cut and tied or sealed so as to prevent sperm from entering into the urethra and thereby prevent fertilization of a female through sexual intercourse. Vasectomies are usually performed in a physician’s office, medical clinic, or, when performed on an animal, in a veterinary clinic. Hospitalization is not normally required as the procedure is not complicated, the incisions are small, and the necessary equipment routine. The leading potential complication is post-vasectomy pain syndrome.
There are several methods by which a surgeon might complete a vasectomy procedure, all of which occlude (i.e., «seal») at least one side of each vas deferens. To help reduce anxiety and increase patient comfort, those who have an aversion to needles may consider a «no-needle» application of anesthesia while the ‘no-scalpel’ or ‘open-ended’ techniques help to accelerate recovery times and increase the chance of healthy recovery.[3]
Due to the simplicity of the surgery, a vasectomy usually takes less than 30 minutes to complete. After a short recovery at the doctor’s office (usually less than an hour), the patient is sent home to rest. Because the procedure is minimally invasive, many vasectomy patients find that they can resume their typical sexual behavior within a week, and do so with little or no discomfort.
Because the procedure is considered a permanent method of contraception and is not easily reversed, patients are usually counseled and advised to consider how the long-term outcome of a vasectomy might affect them both emotionally and physically. The procedure is not often encouraged for young single childless people as their chances for biological parenthood are thereby permanently reduced, sometimes completely.
Medical uses[edit]
A vasectomy is done to prevent fertility in males. It ensures that in most cases the person will be sterile after confirmation of success following surgery. The procedure is regarded as permanent because vasectomy reversal is costly and often does not restore the male’s sperm count or sperm motility to prevasectomy levels. Those with vasectomies have a very small (nearly zero) chance of successfully impregnating someone, but a vasectomy has no effect on rates of sexually transmitted infections.[citation needed]
After vasectomy, the testes remain in the scrotum where Leydig cells continue to produce testosterone and other male hormones that continue to be secreted into the bloodstream.
When the vasectomy is complete, sperm cannot exit the body through the penis. Sperm is still produced by the testicles but is broken down and absorbed by the body. Much fluid content is absorbed by membranes in the epididymis, and much solid content is broken down by the responding macrophages and reabsorbed via the bloodstream. Sperm is matured in the epididymis for about a month before leaving the testicles. After vasectomy, the membranes must increase in size to absorb and store more fluid; this triggering of the immune system causes more macrophages to be recruited to break down and reabsorb more solid content. Within one year after vasectomy, sixty to seventy percent of those vasectomized develop antisperm antibodies.[4] In some cases, vasitis nodosa, a benign proliferation of the ductular epithelium, can also result.[5][6] The accumulation of sperm increases pressure in the vas deferens and epididymis. The entry of the sperm into the scrotum can cause sperm granulomas to be formed by the body to contain and absorb the sperm which the body will treat as a foreign biological substance (much like a virus or bacterium).[7]
Efficacy[edit]
| Frequency | Risk | Source |
|---|---|---|
| 1 in 1400 | Unwanted pregnancy (failure of vasectomy) | [8] |
| 1 in 11 | For comparison: unwanted pregnancy w/ typical use of pill | [2] |
| 1 in 6 | For comparison: unwanted pregnancy w/ typical use of condom | [2] |
| 1 in 40 | Infection after surgery | [9] |
| 1 in 7 | Pain at 7 months after vasectomy | [10] |
| 1 in 110 | Pain at 7 months affecting quality of life | [10] |
Vasectomy is the most effective permanent form of contraception available to males. (Removing the entire vas deferens would very likely be more effective, but it is not something that is regularly done.[11]) In nearly every way that vasectomy can be compared to tubal ligation it has a more positive outlook. Vasectomy is more cost effective, less invasive, has techniques that are emerging that may facilitate easier reversal, and has a much lower risk of postoperative complications.
Early failure rates, i.e. pregnancy within a few months after vasectomy, typically result from unprotected sexual intercourse too soon after the procedure while some sperm continue to pass through the vasa deferentia. Most physicians and surgeons who perform vasectomies recommend one (sometimes two) postprocedural semen specimens to verify a successful vasectomy; however, many people fail to return for verification tests citing inconvenience, embarrassment, forgetfulness, or certainty of sterility.[12] In January 2008, the FDA cleared a home test called SpermCheck Vasectomy that allows patients to perform postvasectomy confirmation tests themselves;[13] however, compliance for postvasectomy semen analysis in general remains low.
Late failure, i.e. pregnancy following spontaneous recanalization of the vasa deferentia, has also been documented.[14] This occurs because the epithelium of the vas deferens (similar to the epithelium of some other human body parts) is capable of regenerating and creating a new tube if the vas deferens is damaged and/or severed.[15] Even when as much as five centimeters (or two inches) of the vas deferens is removed, the vas deferens can still grow back together and become reattached—thus allowing sperm to once again pass and flow through the vas deferens, restoring one’s fertility.[15]
The Royal College of Obstetricians and Gynaecologists states there is a generally agreed-upon rate of late failure of about one in 2000 vasectomies— better than tubal ligations for which the failure rate is one in every 200 to 300 cases.[16] A 2005 review including both early and late failures described a total of 183 recanalizations from 43,642 vasectomies (0.4%), and sixty pregnancies after 92,184 vasectomies (0.07%).[8]
Complications[edit]
Short-term possible complications include infection, bruising and bleeding into the scrotum resulting in a collection of blood known as a hematoma.[17] A study in 2012 demonstrated an infection rate of 2.5% postvasectomy.[9] The stitches on the small incisions required are prone to irritation, though this can be minimized by covering them with gauze or small adhesive bandages. The primary long-term complications are chronic pain conditions or syndromes that can affect any of the scrotal, pelvic or lower-abdominal regions, collectively known as post-vasectomy pain syndrome. Though vasectomy results in increases in circulating immune complexes, these increases are transient. Data based on animal and human studies indicate these changes do not result in increased incidence of atherosclerosis. The risk of testicular cancer is not affected by vasectomy.[18]
In 2014 the AUA reaffirmed that vasectomy is not a risk factor for prostate cancer and that it is not necessary for physicians to routinely discuss prostate cancer in their preoperative counseling of vasectomy patients.[19] There remains ongoing debate regarding whether vasectomy is associated with prostate cancer. A 2017 meta-analysis found no statistically significant increase in risk.[20] A 2019 study of 2.1 million Danish males found that vasectomy increased their incidence of prostate cancer by 15%.[21] A 2020 meta-analysis found that vasectomy increased the incidence by 9%.[22] Other recent studies agree on the 15% increase in risk of developing prostate cancer, but found that people who get a vasectomy are not more likely to die from prostate cancer than those without a vasectomy.[23][24]
Postvasectomy pain[edit]
Post-vasectomy pain syndrome is a chronic and sometimes debilitating condition that may develop immediately or several years after vasectomy.[25] The most robust study of post-vasectomy pain, according to the American Urology Association’s Vasectomy Guidelines 2012 (amended 2015)[26] surveyed people just before their vasectomy and again 7 months later. Of those that responded and who said they did not have any scrotal pain prior to vasectomy, 7% had scrotal pain seven months later which they described as «Mild, a bit of a nuisance», 1.6% had pain that was «Moderate, require painkillers» and 0.9% had pain that was «quite severe and noticeably affecting their quality of life».[10] Post-vasectomy pain can be constant orchialgia or epididymal pain (epididymitis), or it can be pain that occurs only at particular times such as with sexual intercourse, ejaculation, or physical exertion.[7]
Psychological effects[edit]
Approximately 90% are generally reported in reviews as being satisfied with having had a vasectomy,[27] while 7–10% of people regret their decision.[28] For those in relationships, regret was less common when both people in the relationship agreed on the procedure.[29]
Younger people who receive a vasectomy are significantly more likely to regret and seek a reversal of their vasectomy, with one study showing people in their twenties being 12.5 times more likely to undergo a vasectomy reversal later in life (and including some who chose sterilization at a young age). Pre-vasectomy counseling is often emphasised for younger patients.[30][31]
Vasectomy can cause:
- depression,[32][unreliable medical source?][33][unreliable medical source?]
- mental pain,[32][unreliable medical source?][33][unreliable medical source?][34][unreliable medical source?]
- misunderstandings with partners or new partners,[35][unreliable medical source?][34][unreliable medical source?]
- increased thoughts about masculinity,[35][unreliable medical source?]
- thinking about a revasectomy.[34][unreliable medical source?]
Dementia[edit]
An association between vasectomy and primary progressive aphasia, a rare variety of frontotemporal dementia, was reported.[29] However, it is doubtful that there is a causal relationship.[36] The putative mechanism is a cross-reactivity between brain and sperm, including the shared presence of neural surface antigens.[37] In addition, the cytoskeletal tau protein has been found only to exist outside of the CNS in the manchette of sperm.[37]
Procedure[edit]
The traditional incision approach of vasectomy involves numbing of the scrotum with local anesthetic (although some people’s physiology may make access to the vas deferens more difficult in which case general anesthesia may be recommended) after which a scalpel is used to make two small incisions, one on each side of the scrotum at a location that allows the surgeon to bring each vas deferens to the surface for excision. The vasa deferentia are cut (sometimes a section may be removed altogether), separated, and then at least one side is sealed by ligating (suturing), cauterizing (electrocauterization), or clamping.[38] There are several variations to this method that may improve healing, effectiveness, and which help mitigate long-term pain such as post-vasectomy pain syndrome or epididymitis, however the data supporting one over another are limited.[39]
- Fascial interposition: Recanalization of the vas deferens is a known cause of vasectomy failure(s).[40] Fascial interposition («FI»), in which a tissue barrier is placed between the cut ends of the vas by suturing, may help to prevent this type of failure, increasing the overall success rate of vasectomy while leaving the testicular end within the confines of the fascia.[41] The fascia is a fibrous protective sheath that surrounds the vas deferens as well as all other body muscle tissue. This method, when combined with intraluminal cautery (where one or both sides of the vas deferens are electrically «burned» closed to prevent recanalization), has been shown to increase the success rate of vasectomy procedures.
- No-needle anesthesia: Fear of needles for injection of local anesthesia is well known.[42] In 2005, a method of local anesthesia was introduced for vasectomy which allows the surgeon to apply it painlessly with a special jet-injection tool, as opposed to traditional needle application. The numbing agent is forced/pushed onto and deep enough into the scrotal tissue to allow for a virtually pain-free surgery. Lidocaine applied in this manner achieves anesthesia in less than one minute.[citation needed] Initial surveys show a very high satisfaction rate amongst vasectomy patients.[42] Once the effects of no-needle anesthesia set in, the vasectomy procedure is performed in the routine manner. However, unlike in conventional local anesthesia where needles and syringes are used on one patient only, the applicator is not single use and cannot be properly cleaned leading to concerns regarding infection control.
- No-scalpel vasectomy (NSV): Also known as a «key-hole» vasectomy,[38] is a vasectomy in which a sharp hemostat (as opposed to a scalpel) is used to puncture the scrotum. This method has come into widespread use as the resulting smaller «incision» or puncture wound typically limits bleeding and hematomas. Also the smaller wound has less chance of infection, resulting in faster healing times compared to the larger/longer incisions made with a scalpel. The surgical wound created by the no-scalpel method usually does not require stitches. NSV is the most commonly performed type of minimally invasive vasectomy, and both describe the method of vasectomy that leads to access of the vas deferens.[43]

- Open-ended vasectomy: In this procedure the testicular end of the vas deferens is not sealed, which allows continued streaming of sperm into the scrotum. This method may avoid testicular pain resulting from increased back-pressure in the epididymis.[7] Studies suggest that this method may reduce long-term complications such as post-vasectomy pain syndrome.[44][45]
- Vas irrigation: Injections of sterile water or euflavine (which kills sperm) are put into the distal portion of the vas at the time of surgery which then brings about a near-immediate sterile («azoospermatic») condition. The use of euflavine does however, tend to decrease time (or, number of ejaculations) to azoospermia vs. the water irrigation by itself. This additional step in the vasectomy procedure, (and similarly, fascial interposition), has shown positive results but is not as prominently in use, and few surgeons offer it as part of their vasectomy procedure.[39]
Other techniques[edit]
The following vasectomy methods have purportedly had a better chance of later reversal but have seen less use by virtue of known higher failure rates (i.e., recanalization). An earlier clip device, the VasClip, is no longer on the market, due to unacceptably high failure rates.[46][47][48][unreliable medical source?]
The VasClip method, though considered reversible, has had a higher cost and resulted in lower success rates. Also, because the vasa deferentia are not cut or tied with this method, it could technically be classified as other than a vasectomy. Vasectomy reversal (and the success thereof) was conjectured to be higher as it only required removing the Vas-Clip device. This method achieved limited use, and scant reversal data are available.[48]
Vas occlusion techniques[edit]
- Injected plugs: There are two types of injected plugs which can be used to block the vasa deferentia. Medical-grade polyurethane (MPU) or medical-grade silicone rubber (MSR) starts as a liquid polymer that is injected into the vas deferens after which the liquid is clamped in place until is solidifies (usually in a few minutes).[49]
- Intra-vas device: The vasa deferentia can also be occluded by an intra-vas device (IVD). A small cut is made in the lower abdomen after which a soft silicone or urethane plug is inserted into each vas tube thereby blocking (occluding) sperm. This method allows for the vas to remain intact. IVD technique is done in an out-patient setting with local anesthetic, similar to a traditional vasectomy. IVD reversal can be performed under the same conditions making it much less costly than vasovasostomy which can require general anesthesia and longer surgery time.[50]
Both vas occlusion techniques require the same basic patient setup: local anesthesia, puncturing of the scrotal sac for access of the vas, and then plug or injected plug occlusion. The success of the aforementioned vas occlusion techniques is not clear and data are still limited. Studies have shown, however, that the time to achieve sterility is longer than the more prominent techniques mentioned in the beginning of this article. The satisfaction rate of patients undergoing IVD techniques has a high rate of satisfaction with regard to the surgery experience itself.[51]
Recovery[edit]


14 days after vasectomy surgery
Sexual intercourse can usually be resumed in about a week (depending on recovery); however, pregnancy is still possible as long as the sperm count is above zero. Another method of contraception must be relied upon until a sperm count is performed either two months after the vasectomy or after 10–20 ejaculations have occurred.[52]
After a vasectomy, contraceptive precautions must be continued until azoospermia is confirmed. Usually two semen analyses at three and four months are necessary to confirm azoospermia. The British Andrological Society has recommended that a single semen analysis confirming azoospermia after sixteen weeks is sufficient.[53]
Post-vasectomy, testicles will continue to produce sperm cells. As before vasectomy, unused sperm are reabsorbed by the body.[54]
Conceiving after vasectomy[edit]
In order to allow the possibility of reproduction via artificial insemination after vasectomy, some opt for cryopreservation of sperm before sterilization. Dr Allan Pacey, senior lecturer in andrology at Sheffield University and secretary of the British Fertility Society, notes that those he sees for a vasectomy reversal which has not worked express wishing they had known they could have stored sperm. Pacey notes, «The problem is you’re asking a man to foresee a future where he might not necessarily be with his current partner—and that may be quite hard to do when she’s sitting next to you.»[55]
The cost of cryo-preservation (sperm banking) may also be substantially less than alternative vaso-vasectomy procedures, compared to the costs of in-vitro fertilization (IVF) which usually run from $12,000 to $25,000.[56]
Sperm can be aspirated from the testicles or the epididymis, and while there is not enough for successful artificial insemination, there is enough to fertilize an ovum by intracytoplasmic sperm injection. This avoids the problem of antisperm antibodies and may result in a faster pregnancy. IVF may be less costly per cycle than reversal in some health-care systems, but a single IVF cycle is often insufficient for conception. Disadvantages include the need for procedures on the woman, and the standard potential side-effects of IVF for both the mother and the child.[57]
Vasectomy reversal[edit]
Although those considering vasectomies should not think of them as reversible, and most people and their partners are satisfied with the operation,[58][59] life circumstances and outlooks can change, and there is a surgical procedure to reverse vasectomies using vasovasostomy (a form of microsurgery first performed by Earl Owen in 1971[60][61]). Vasovasostomy is effective at achieving pregnancy in a variable percentage of cases, and total out-of-pocket costs in the United States are often upwards of $10,000.[62] The typical success rate of pregnancy following a vasectomy reversal is around 55% if performed within 10 years, and drops to around 25% if performed after 10 years.[63] After reversal, sperm counts and motility are usually much lower than pre-vasectomy levels. There is evidence that those who had a vasectomy may produce more abnormal sperm, which would explain why even a mechanically successful reversal does not always restore fertility.[64][65] The higher rates of aneuploidy and diploidy in the sperm cells of those who have undergone vasectomy reversal may lead to a higher rate of birth defects.[64]
Approximately 2% of men who have undergone vasectomy will undergo a reversal within 10 years of the procedure.[31] Some reasons that people seek vasectomy reversals include wanting a family with a new partner following a relationship breakdown or divorce, their original partner dying and subsequently going on to repartner and to want children, the unexpected death of a child, or a long-standing couple changing their minds some time later, often prompted by situations such as improved finances or existing children approaching the age of school or leaving home.[55] Patients often comment that they never anticipated the possibility of a relationship breakdown or death, or how that might affect their situation at the time of having their vasectomy. A small number of vasectomy reversals are also performed in attempts to relieve post-vasectomy pain syndrome.[66]
Prevalence[edit]
Internationally, vasectomy rates are vastly different.[67] While female sterilisation is the most widely used method worldwide, with 223 million women relying on it, only 28 million women rely on their partner’s vasectomy.[68] In the world’s 69 least developed countries less than 0.1% of males use vasectomies on average. Of 54 African countries, only ten report measurable vasectomy use and only Swaziland, Botswana, and South Africa exceed 0.1% prevalence.[67]
| country | vasectomy usage[67] | notes |
|---|---|---|
| Canada | 22% | «of all women rely on vasectomy» |
| UK | 17% — 21% | only range given |
| New Zealand | 17% — 21% | only range given |
| South Korea | 17% — 21% | only range given |
| Australia | ~10% | |
| Belgium | ~10% | |
| Denmark | ~10% | |
| Spain | ~10% | |
| Switzerland | ~10% | |
| Nepal | 7.8% | |
| Brazil | 5.1% | |
| Colombia | 3.4% | |
| Swaziland | 0.3% | |
| Botswana | 0.4% | |
| South Africa | 0.7% |
In North America and Europe vasectomy usage is on the order of 10% with some countries reaching 20%.[67] Despite its high efficacy, in the United States, vasectomy is utilized less than half the rate of the alternative female tubal ligation.[69] According to the research, vasectomy in the US is least utilized among black and Latino populations, the groups that have the highest rates of female sterilization.[69]
New Zealand, in contrast, has higher levels of vasectomy than tubal ligation. 18% of all males, and 25% of all married males, have had a vasectomy. The age cohort with the highest level of vasectomy was 40–49, where 57% of males had taken it up.[70] Canada, the UK, Bhutan and the Netherlands all have similar levels of uptake.[71]
History[edit]
The first human vasectomies were performed in the late 19th century. The procedure was initially used mainly as a treatment for prostate enlargement and as a eugenic method for sterilizing «degenerates».[72] Vasectomy as a method of voluntary birth control began during the Second World War.[73]
The first recorded vasectomy was performed on a dog in 1823.[73] The first human vasectomies were performed to treat benign prostatic hyperplasia, or enlargement of the prostate. Castration had sometimes been used as a treatment for this condition in the 1880s, but, given the serious side effects, doctors sought alternative treatments. The first to suggest vasectomy as an alternative to castration may have been James Ewing Mears (in 1890), or Jean Casimir Félix Guyon.[72]
The first human vasectomy is thought to have been performed by Reginald Harrison.[73][additional citation(s) needed] By 1900, Harrison reported that he had performed more than 100 vasectomies with no adverse outcomes.[72]
In the late 1890s, vasectomy also came to be proposed as a eugenic measure for the sterilization of men considered unfit to reproduce. The first case report of vasectomy in the United States was in 1897, by A. J. Ochsner, a surgeon in Chicago, in a paper titled, «Surgical treatment of habitual criminals». He believed vasectomy to be a simple, effective means for stemming the tide of racial degeneration widely believed to be occurring.[74][75] In 1902, Harry C. Sharp, the surgeon at the Indiana Reformatory, reported that he had sterilized 42 inmates in an effort to both reduce criminal behavior in those individuals and prevent the birth of future criminals.[76]
Eugen Steinach (1861–1944), an Austrian physician, believed that a unilateral vasectomy (severing only one of the two vasa deferentia) in older individuals could restore general vigor and sexual potency, shrink enlarged prostates, and cure various ailments by somehow boosting the hormonal output of the vasectomized testicle.[77] This surgery, which became very popular in the 1920s, was undertaken by many wealthy individuals, including Sigmund Freud and W. B. Yeats.[78] Since these operations lacked rigorous controlled trials, any rejuvenating effect was likely due to the placebo effect, and with the later development of synthetic injectable hormones, this operation fell out of vogue.[77][79]
Vasectomy began to be regarded as a method of consensual birth control during the Second World War.[73] The first vasectomy program on a national scale was launched in 1954 in India.[80]
The procedure is seldom performed on dogs, with castration remaining the preferred reproductive control option for canines. It is regularly performed on bulls.[81]
Society and culture[edit]
Availability and legality[edit]
Vasectomy costs are (or may be) covered in different countries, as a method of both contraception or population control, with some offering it as a part of a national health insurance. The procedure was generally considered illegal in France until 2001, due to provisions in the Napoleonic Code forbidding «self-mutilation». No French law specifically mentioned vasectomy until a 2001 law on contraception and infanticide permitted the procedure.[82]
The U.S. Affordable Care Act (signed into law in 2010) does not cover vasectomies,[83] although eight states require state-health insurance plans to cover the cost. These include: Illinois, Maryland, New Jersey, New Mexico, New York, Oregon, Vermont and Washington.[84]
In 2014, the Iranian parliament voted for a bill that would ban the procedure.[85]
Tourism[edit]
Medical tourism, where a patient travels to a less-developed location where a procedure is cheaper to save money and combine convalescence with a vacation, is infrequently used for vasectomy due to its low cost, but is more likely to be used for vasectomy reversal. Many hospitals list vasectomy as being available. Medical tourism has been scrutinized by some governments for quality of care and postoperative care issues.[86]
Shooting of Andrew Rynne[edit]
In 1990 Andrew Rynne, chairperson of the Irish Family Planning Association, and the Republic of Ireland’s first vasectomy specialist,[87] was shot by a former client, but he survived. The incident is the subject of a short film, The Vasectomy Doctor, by Paul Webster.[88]
See also[edit]
- Caroline Deys, a noted vasectomy specialist
- List of surgeries by type
- Male contraceptive
- Orchiectomy
- Testicular sperm extraction
- World Vasectomy Day
References[edit]
- ^ Popenoe P (1934). «The progress of eugenic sterilization». Journal of Heredity. 25 (1): 19.
- ^ a b c d Trussell, James (2011). «Contraceptive efficacy». In Hatcher, Robert A.; Trussell, James; Nelson, Anita L.; Cates, Willard Jr.; Kowal, Deborah; Policar, Michael S. (eds.). Contraceptive technology (20th revised ed.). New York: Ardent Media. pp. 779–863. ISBN 978-1-59708-004-0. ISSN 0091-9721. OCLC 781956734. Table 26–1 = Table 3–2 Percentage of women experiencing an unintended pregnancy during the first year of typical use and the first year of perfect use of contraception, and the percentage continuing use at the end of the first year. United States.
- ^ «What Happens When I Get a Vasectomy?». WebMD. Retrieved 7 October 2021.
- ^ Hattikudur, S.; Shanta, S. RAO; Shahani, S.K.; Shastri, P.R.; Thakker, P.V.; Bordekar, A.D. (2009). «Immunological and Clinical Consequences of Vasectomy*». Andrologia. 14 (1): 15–22. doi:10.1111/j.1439-0272.1982.tb03089.x. PMID 7039414. S2CID 10468133.
- ^ Deshpande RB, Deshpande J, Mali BN, Kinare SG (1985). «Vasitis nodosa (a report of 7 cases)». J Postgrad Med. 31 (2): 105–8. PMID 4057111.
- ^ Hirschowitz, L; Rode, J; Guillebaud, J; Bounds, W; Moss, E (1988). «Vasitis nodosa and associated clinical findings». Journal of Clinical Pathology. 41 (4): 419–423. doi:10.1136/jcp.41.4.419. PMC 1141468. PMID 3366928.
- ^ a b c Christiansen C, Sandlow J (2003). «Testicular Pain Following Vasectomy: A Review of Post vasectomy Pain Syndrome». Journal of Andrology. 24 (3): 293–8. doi:10.1002/j.1939-4640.2003.tb02675.x. PMID 12721203.
- ^ a b Griffin, T; Tooher, R; Nowakowski, K; Lloyd, M; Maddern, G (2005). «How Little is Enough? The Evidence for Post-Vasectomy Testing». The Journal of Urology. 174 (1): 29–36. doi:10.1097/01.ju.0000161595.82642.fc. PMID 15947571.
- ^ a b Nevill et al (2013) Surveillance of surgical site infection post vasectomy. Journal of Infection Prevention. January 2013. Vol 14(1) [1]
- ^ a b c Leslie TA; Illing RO; Cranston DW; et al. (2007). «The incidence of chronic scrotal pain after vasectomy: a prospective audit». BJU Int. 100 (6): 1330–3. doi:10.1111/j.1464-410X.2007.07128.x. PMID 17850378. S2CID 23328539.
- ^ «Is it possible to have my entire vas deferens removed? — Vasectomy Questions & Answers | Vasectomy.com». www.vasectomy.com.
- ^ Christensen, R. E.; Maples, D. C. (2005). «Postvasectomy Semen Analysis: Are Men Following Up?». The Journal of the American Board of Family Medicine. 18 (1): 44–47. doi:10.3122/jabfm.18.1.44. PMID 15709063.
- ^ Klotz, Kenneth L.; Coppola, Michael A.; Labrecque, Michel; Brugh Vm, Victor M.; Ramsey, Kim; Kim, Kyung-ah; Conaway, Mark R.; Howards, Stuart S.; Flickinger, Charles J.; Herr, John C. (2008). «Clinical and Consumer Trial Performance of a Sensitive Immunodiagnostic Home Test That Qualitatively Detects Low Concentrations of Sperm Following Vasectomy». The Journal of Urology. 180 (6): 2569–2576. doi:10.1016/j.juro.2008.08.045. PMC 2657845. PMID 18930494.
- ^ Philp, T; Guillebaud, J; Budd, D (1984). «Late failure of vasectomy after two documented analyses showing azoospermic semen». BMJ. 289 (6437): 77–79. doi:10.1136/bmj.289.6437.77. PMC 1441962. PMID 6428685.
- ^ a b Rolnick, H. C. (1924). «Regeneration of the Vas Deferens». Archives of Surgery. 9: 188. doi:10.1001/archsurg.1924.01120070191008.
- ^ Royal College of Obstetricians and Gynaecologists. «Sterilisation for women and men: what you need to know». Archived from the original on 4 January 2011. Retrieved 31 January 2011.
- ^ Yang, Fang; Li, Junjun; Dong, Liang; Tan, Kun; Huang, Xiaopeng; Zhang, Peihai; Liu, Xiaozhang; Chang, Degui; Yu, Xujun (2021). «Review of Vasectomy Complications and Safety Concerns». The World Journal of Men’s Health. 39 (3): 406–418. doi:10.5534/wjmh.200073. ISSN 2287-4208. PMC 8255399. PMID 32777870.
- ^ Schwingl, Pamela J; Guess, Harry A (2000). «Safety and effectiveness of vasectomy». Fertility and Sterility. 73 (5): 923–936. CiteSeerX 10.1.1.494.1247. doi:10.1016/S0015-0282(00)00482-9. PMID 10785217.
- ^ «AUA Responds to Study Linking Vasectomy with Prostate Cancer». American Urological Association. Archived from the original on 31 March 2016. Retrieved 19 March 2016.
- ^ Bhindi, Bimal; Wallis, Christopher J. D.; Nayan, Madhur; Farrell, Ann M.; Trost, Landon W.; Hamilton, Robert J.; Kulkarni, Girish S.; Finelli, Antonio; Fleshner, Neil E.; Boorjian, Stephen A.; Karnes, R. Jeffrey (17 July 2017). «The Association Between Vasectomy and Prostate Cancer: A Systematic Review and Meta-analysis». JAMA Internal Medicine. 177 (9): 1273–1286. doi:10.1001/jamainternmed.2017.2791. PMC 5710573. PMID 28715534.
- ^ Husby, Anders; Wohlfahrt, Jan; Melbye, Mads (1 January 2020). «Vasectomy and Prostate Cancer Risk: A 38-Year Nationwide Cohort Study». Journal of the National Cancer Institute. 112 (1): 71–77. doi:10.1093/jnci/djz099. ISSN 1460-2105. PMID 31119294.
- ^ Cheng, Sheng; Yang, Bo; Xu, Liwei; Zheng, Qiming; Ding, Guoqing; Li, Gonghui (9 August 2020). «Vasectomy and prostate cancer risk: a meta-analysis of prospective studies». Carcinogenesis. 42 (1): 31–37. doi:10.1093/carcin/bgaa086. ISSN 1460-2180. PMID 32772072.
- ^ Seikkula, Heikki; Kaipia, Antti; Hirvonen, Elli; Rantanen, Matti; Pitkäniemi, Janne; Malila, Nea; Boström, Peter J. (February 2020). «Vasectomy and the risk of prostate cancer in a Finnish nationwide population-based cohort». Cancer Epidemiology. 64: 101631. doi:10.1016/j.canep.2019.101631. ISSN 1877-783X. PMID 31760357. S2CID 208276171.
- ^ Xu, Yawei; Li, Lei; Yang, Wuping; Zhang, Kenan; Ma, Kaifang; Xie, Haibiao; Zhou, Jingcheng; Cai, Lin; Gong, Yanqing; Zhang, Zheng; Gong, Kan (29 April 2021). «Association between vasectomy and risk of prostate cancer: a meta-analysis». Prostate Cancer and Prostatic Diseases. 24 (4): 962–975. doi:10.1038/s41391-021-00368-7. ISSN 1476-5608. PMID 33927357. S2CID 233458537.
- ^ Nangia, Ajay K.; Myles, Jonathan L.; Thomas Aj, Anthony J. (2000). «Vasectomy Reversal for the Post-Vasectomy Pain Syndrome: : A Clinical and Histological Evaluation». The Journal of Urology. 164 (6): 1939–1942. doi:10.1016/S0022-5347(05)66923-6. PMID 11061886.
- ^ «Vasectomy Guideline — American Urological Association». www.auanet.org.
- ^ THONNEAU, P.; D’ISLE, BÉATRICE (1990). «Does vasectomy have long-term effects on somatic and psychological health status?». International Journal of Andrology. 13 (6): 419–432. doi:10.1111/j.1365-2605.1990.tb01050.x. PMID 2096110.
- ^ Labrecque, Michel; Paunescu, Cristina; Plesu, Ioana; Stacey, Dawn; Légaré, France (2010). «Evaluation of the effect of a patient decision aid about vasectomy on the decision-making process: a randomized trial». Contraception. 82 (6): 556–562. doi:10.1016/j.contraception.2010.05.003. PMID 21074020.
- ^ a b Köhler TS, Fazili AA, Brannigan RE (August 2009). «Putative health risks associated with vasectomy». Urol. Clin. North Am. 36 (3): 337–45. doi:10.1016/j.ucl.2009.05.004. PMID 19643236.
- ^ POTTS, J.M.; PASQUALOTTO, F.F.; NELSON, D.; THOMAS, A.J.; AGARWAL, A. (June 1999). «Patient Characteristics Associated with Vasectomy Reversal» (PDF). The Journal of Urology. 161 (6): 1835–1839. doi:10.1016/S0022-5347(05)68819-2. PMID 10332448.
- ^ a b Dohle, Gert R.; Diemer, Thorsten; Kopa, Zsolt; Krausz, Csilla; Giwercman, Aleksander; Jungwirth, Andreas; European Association of Urology Working Group on Male Infertility (January 2012). «European Association of Urology guidelines on vasectomy». European Urology. 61 (1): 159–163. doi:10.1016/j.eururo.2011.10.001. ISSN 1873-7560. PMID 22033172.
- ^ a b No-Reply (4 November 2014). «Psychological Effects of a Vasectomy». Dr. Elist. Retrieved 15 January 2023.
- ^ a b Vogel, Kaitlin. «There’s a Fascinating Connection That Might Exist Between Vasectomies and Depression—Here’s What to Know About It». Parade: Entertainment, Recipes, Health, Life, Holidays. Retrieved 15 January 2023.
- ^ a b c shucosmetic (29 June 2013). «Psychological Effects of Vasectomy | Minnesota». Medical Center Minneapolis | Varicose Veins St. Paul | Nail Fungus MN. Retrieved 15 January 2023.
- ^ a b «Emotional Reactions After a Vasectomy». His Choice. Retrieved 15 January 2023.
- ^ Köhler, TS.; Choy, JT.; Fazili, AA.; Koenig, JF.; Brannigan, RE. (November 2012). «A critical analysis of the reported association between vasectomy and frontotemporal dementia». Asian J Androl. 14 (6): 903–4. doi:10.1038/aja.2012.94. PMC 3720109. PMID 23064682.
- ^ a b Rogalski E, Weintraub S, Mesulam MM (2013). «Are there susceptibility factors for primary progressive aphasia?». Brain Lang. 127 (2): 135–8. doi:10.1016/j.bandl.2013.02.004. PMC 3740011. PMID 23489582.
- ^ a b Cook, LA; Pun, A; Gallo, MF; Lopez, LM; Van Vliet, HA (30 March 2014). «Scalpel versus no-scalpel incision for vasectomy». The Cochrane Database of Systematic Reviews. 2014 (3): CD004112. doi:10.1002/14651858.CD004112.pub4. PMC 6464377. PMID 24683021.
- ^ a b Cook, Lynley A.; Van Vliet, Huib AAM; Lopez, Laureen M; Pun, Asha; Gallo, Maria F (2014). Cook, Lynley A. (ed.). «Vasectomy occlusion techniques for male sterilization». Cochrane Database of Systematic Reviews. 2014 (2): CD003991. doi:10.1002/14651858.CD003991.pub4. PMC 7173716. PMID 24683020.
- ^ webmaster@vasectomy-information.com (14 September 2007). «Recanalization of the vas deferens». Vasectomy-information.com. Archived from the original on 4 January 2012. Retrieved 28 December 2011.
- ^ Sokal, David; Irsula, Belinda; Hays, Melissa; Chen-Mok, Mario; Barone, Mark A; Investigator Study, Group (2004). «Vasectomy by ligation and excision, with or without fascial interposition: a randomized controlled trial ISRCTN77781689». BMC Medicine. 2 (1): 6. doi:10.1186/1741-7015-2-6. PMC 406425. PMID 15056388.

- ^ a b Weiss, RS; Li, PS (2005). «No-needle jet anesthetic technique for no-scalpel vasectomy». The Journal of Urology. 173 (5): 1677–80. doi:10.1097/01.ju.0000154698.03817.d4. PMID 15821547. S2CID 13097425.
- ^ Sharlip ID, Belker AM, Honig S, Labrecque M, Marmar JL, Ross LS, Sandlow JI, Sokal DC (December 2012). «Vasectomy: AUA guideline». The Journal of Urology. 188 (6 Suppl): 2482–91. doi:10.1016/j.juro.2012.09.080. PMID 23098786.
- ^ Moss, WM (December 1992). «A comparison of open-end versus closed-end vasectomies: a report on 6220 cases». Contraception. 46 (6): 521–5. doi:10.1016/0010-7824(92)90116-B. PMID 1493712.
- ^ Shapiro, EI; Silber, SJ (November 1979). «Open-ended vasectomy, sperm granuloma, and postvasectomy orchialgia». Fertility and Sterility. 32 (5): 546–50. doi:10.1016/S0015-0282(16)44357-8. PMID 499585.
- ^ Levine, LA; Abern, MR; Lux, MM (2006). «Persistent motile sperm after ligation band vasectomy». The Journal of Urology. 176 (5): 2146–8. doi:10.1016/j.juro.2006.07.028. PMID 17070280.
- ^ «Male Contraception Update for the public — August 2008, 3(8)». Imccoalition.org. Archived from the original on 27 March 2012. Retrieved 28 December 2011.
- ^ a b «VasClip». www.vasweb.com. Archived from the original on 19 October 2011.
- ^ «Injected plugs». MaleContraceptives.org. 27 July 2011. Retrieved 28 December 2011.
- ^ «Intra Vas Device (IVD)». MaleContraceptives.org. Retrieved 28 December 2011.
- ^ Cook, LA; Van Vliet, HA; Lopez, LM; Pun, A; Gallo, MF (30 March 2014). «Vasectomy occlusion techniques for male sterilization». The Cochrane Database of Systematic Reviews. 2014 (3): CD003991. doi:10.1002/14651858.CD003991.pub4. PMC 7173716. PMID 24683020.
- ^ Healthwise Staff (13 May 2010). «Vasectomy Procedure, Effects, Risks, Effectiveness, and More». webmd.com. Retrieved 29 March 2012.
- ^ «Post Vasectomy Semen Analysis». Cambridge IVF. Cambridge IVF. Archived from the original on 26 February 2021. Retrieved 23 October 2015.
- ^ «Vasectomy». University of Miami Health System, Miller School of Medicine. University of Miami Health System, Miller School of Medicine. Retrieved 28 December 2019.
- ^ a b Murphy, Clare. «Divorce fuels vasectomy reversals», BBC News, 18 March 2009. Retrieved 19 September 2012.
- ^ Klein, Amy (20 June 2019). «I.V.F. is Expensive. Here’s How to Bring Down the Cost». The New York Times. Retrieved 8 July 2021.
- ^ Shridharani, Anand; Sandlow, Jay I (2010). «Vasectomy reversal versus IVF with sperm retrieval: which is better?». Current Opinion in Urology. 20 (6): 503–509. doi:10.1097/MOU.0b013e32833f1b35. PMID 20852426. S2CID 42105503.
- ^ Landry E, Ward V (1997). «Perspectives from Couples on the Vasectomy Decision: A Six-Country Study» (PDF). Reproductive Health Matters. (special issue): 58–67. Archived from the original (PDF) on 4 March 2016. Retrieved 17 June 2006.
- ^ Jamieson, D (2002). «A comparison of women’s regret after vasectomy versus tubal sterilization». Obstetrics & Gynecology. 99 (6): 1073–1079. doi:10.1016/S0029-7844(02)01981-6. PMID 12052602. S2CID 6586905.
- ^ «About Vasectomy Reversal». Professor Earl Owen’s homepage. Archived from the original on 6 December 2007. Retrieved 29 November 2007.
- ^ Owen ER (1977). «Microsurgical vasovasostomy: a reliable vasectomy reversal». Urology. 167 (2 Pt 2): 1205. doi:10.1016/S0022-5347(02)80388-3. PMID 11905902.
- ^ Vasectomy Reversal http://www.epigee.org/guide/vasectomy_reversal.html
- ^ Cited in Laurance, Jeremy (2009) «Vasectomy Reversal: First Cut Isn’t Final» in The Independent 30 March 2009 https://www.independent.co.uk/life-style/health-and-families/health-news/vasectomy-reversal-first-cut-isnt-final-1657039.html
- ^ a b Sukcharoen, Nares; Ngeamvijawat, J; Sithipravej, T; Promviengchai, S (2003). «High sex chromosome aneuploidy and diploidy rate of epididymal spermatozoa in obstructive azoospermic men». Journal of Assisted Reproduction and Genetics. 20 (5): 196–203. doi:10.1023/A:1023674110940. PMC 3455301. PMID 12812463.
- ^ Abdelmassih, V.; Balmaceda, JP; Tesarik, J; Abdelmassih, R; Nagy, ZP (2002). «Relationship between time period after vasectomy and the reproductive capacity of sperm obtained by epididymal aspiration». Human Reproduction. 17 (3): 736–740. doi:10.1093/humrep/17.3.736. PMID 11870128.
- ^ Horovitz, D. (February 2012). «Vasectomy reversal provides long-term pain relief for men with the post-vasectomy pain syndrome». Journal of Urology. 187 (2): 613–7. doi:10.1016/j.juro.2011.10.023. PMID 22177173.
- ^ a b c d Jacobstein, Roy (December 2015). «The kindest cut: global need to increase vasectomy availability». The Lancet. Global Health. 3 (12): e733–734. doi:10.1016/S2214-109X(15)00168-0. ISSN 2214-109X. PMID 26545447.
- ^ «Contraceptive Use 2011». UN Department of Economic and Social Affairs, Population Division, 2012. Archived from the original on 28 September 2014. Retrieved 8 October 2017.
- ^ a b Shih G, Turok DK, Parker WJ (April 2011). «Vasectomy: the other (better) form of sterilization». Contraception. 83 (4): 310–5. doi:10.1016/j.contraception.2010.08.019. PMID 21397087.[permanent dead link]
- ^ Sneyd, Mary Jane; Cox, Brian; Paul, Charlotte; Skegg, David C.G. (2001). «High prevalence of vasectomy in New Zealand». Contraception. 64 (3): 155–159. doi:10.1016/S0010-7824(01)00242-6. PMID 11704094.
- ^ Pile, John M.; Barone, Mark A. (2009). «Demographics of Vasectomy—USA and International». Urologic Clinics of North America. 36 (3): 295–305. doi:10.1016/j.ucl.2009.05.006. PMID 19643232.
- ^ a b c Drake, M.J.; Mills, I.W.; Cranston, D. (1999). «On the chequered history of vasectomy». BJU International. 84 (4): 475–481. doi:10.1046/j.1464-410x.1999.00206.x. PMID 10468765. S2CID 20563820.
- ^ a b c d Leavesley, JH (1980). «Brief history of vasectomy». Family Planning Information Service. 1 (5): 2–3. PMID 12336890.
- ^ A.J., Ochsner (1969). «Surgical Treatment of Habitual Criminals». Buck V Bell Documents.
- ^ Carlson, Elof Axel (2011). «The Hoosier Connection: Compulsory Sterilization as Moral Hygiene». In Lombardo, Paul A. (ed.). A Century of Eugenics in America: From the Indiana Experiment to the Human Genome Era. Indiana University Press. p. 19. ISBN 978-0253222695.
- ^ Reilly, Phillip (1991). The Surgical Solution: A History of Involuntary Sterilization in the United States. Johns Hopkins University Press. pp. 30–33.
- ^ a b Schultheiss, Dirk; Engel, Rainer M. (1 November 2003). «G. Frank Lydston (1858–1923) revisited: androgen therapy by testicular implantation in the early twentieth century». World Journal of Urology. 21 (5): 356–363. doi:10.1007/s00345-003-0370-z. ISSN 0724-4983. PMID 14586546. S2CID 12706657.
- ^ Ellmann, Richard (9 May 1985). «Yeats’s Second Puberty». The New York Review of Books. Retrieved 23 August 2017.
- ^ McLaren, Angus (9 March 2012). Reproduction by Design: Sex, Robots, Trees, and Test-Tube Babies in Interwar Britain. University of Chicago Press. ISBN 9780226560694.
- ^ Sharma, Sanjay (April–June 2014). «A Study of Male Sterilization with No Scalpel Vasectomy» (PDF). JK Science. 16 (2): 67. Retrieved 23 October 2015.
- ^ Dean A. Hendrickson; A. N. Baird (5 June 2013). Turner and McIlwraith’s Techniques in Large Animal Surgery. John Wiley & Sons. p. 541. ISBN 978-1-118-68404-7.
- ^ Latham, Melanie (2002). Regulating Reproduction: A Century of Conflict in Britain and France. Manchester University Press. ISBN 978-0-7190-5699-4.
- ^ «Where Can I Buy a Vasectomy & How Much Will It Cost?». Planned Parenthood. Retrieved 30 June 2022.
- ^ «My husband would like to get a vasectomy but when I checked with our insurer, they told me that the plan would cover my sterilization without cost sharing but we would have to pay part of the costs for his procedure. What is the reason for that?». Kaiser Family Foundation. 15 July 2020. Retrieved 30 June 2022.
- ^ Moghtader, Michelle (11 August 2014). «Iranian parliament bans vasectomies in bid to boost birth rate». Reuters. Retrieved 15 July 2018.
- ^ Lunt, Neil; Carrera, Percivil (2010). «Medical tourism: Assessing the evidence on treatment abroad». Maturitas. 66 (1): 27–32. doi:10.1016/j.maturitas.2010.01.017. PMID 20185254.
- ^ «‘I could look down the barrel of the gun. I could see the worm of the gun.’ — RTÉ Radio 1 Highlights».
- ^ Jarlath Regan (26 May 2019). «Dr. Andrew Rynne». An Irishman Abroad (Podcast) (297 ed.). SoundCloud. Archived from the original on 27 May 2019. Retrieved 27 May 2019.
External links[edit]
- MedlinePlus Encyclopedia
- How to treat: vasectomy and reversal, Australian Doctor, 2 July 2014 Archived 10 April 2020 at the Wayback Machine
| Vasectomy | |
|---|---|
|
|
| Background | |
| Type | Sterilization |
| First use | 1899 (experiments from 1785)[1] |
| Failure rates (first year) | |
| Perfect use | 0.10%[2] |
| Typical use | 0.15%[2] «Vas-Clip» nearly 1% |
| Usage | |
| Duration effect | Permanent |
| Reversibility | Possible |
| User reminders | Two consecutive negative semen specimens required to verify no sperm. |
| Clinic review | All |
| Advantages and disadvantages | |
| STI protection | No |
| Benefits | No need for general anesthesia. Lower cost and less invasive than tubal ligation for females. |
| Risks | Temporary local inflammation of the testes, long-term genital pain. |
Vasectomy, or vasoligation, is an elective surgical procedure for male sterilization or permanent contraception. During the procedure, the male vasa deferentia are cut and tied or sealed so as to prevent sperm from entering into the urethra and thereby prevent fertilization of a female through sexual intercourse. Vasectomies are usually performed in a physician’s office, medical clinic, or, when performed on an animal, in a veterinary clinic. Hospitalization is not normally required as the procedure is not complicated, the incisions are small, and the necessary equipment routine. The leading potential complication is post-vasectomy pain syndrome.
There are several methods by which a surgeon might complete a vasectomy procedure, all of which occlude (i.e., «seal») at least one side of each vas deferens. To help reduce anxiety and increase patient comfort, those who have an aversion to needles may consider a «no-needle» application of anesthesia while the ‘no-scalpel’ or ‘open-ended’ techniques help to accelerate recovery times and increase the chance of healthy recovery.[3]
Due to the simplicity of the surgery, a vasectomy usually takes less than 30 minutes to complete. After a short recovery at the doctor’s office (usually less than an hour), the patient is sent home to rest. Because the procedure is minimally invasive, many vasectomy patients find that they can resume their typical sexual behavior within a week, and do so with little or no discomfort.
Because the procedure is considered a permanent method of contraception and is not easily reversed, patients are usually counseled and advised to consider how the long-term outcome of a vasectomy might affect them both emotionally and physically. The procedure is not often encouraged for young single childless people as their chances for biological parenthood are thereby permanently reduced, sometimes completely.
Medical uses[edit]
A vasectomy is done to prevent fertility in males. It ensures that in most cases the person will be sterile after confirmation of success following surgery. The procedure is regarded as permanent because vasectomy reversal is costly and often does not restore the male’s sperm count or sperm motility to prevasectomy levels. Those with vasectomies have a very small (nearly zero) chance of successfully impregnating someone, but a vasectomy has no effect on rates of sexually transmitted infections.[citation needed]
After vasectomy, the testes remain in the scrotum where Leydig cells continue to produce testosterone and other male hormones that continue to be secreted into the bloodstream.
When the vasectomy is complete, sperm cannot exit the body through the penis. Sperm is still produced by the testicles but is broken down and absorbed by the body. Much fluid content is absorbed by membranes in the epididymis, and much solid content is broken down by the responding macrophages and reabsorbed via the bloodstream. Sperm is matured in the epididymis for about a month before leaving the testicles. After vasectomy, the membranes must increase in size to absorb and store more fluid; this triggering of the immune system causes more macrophages to be recruited to break down and reabsorb more solid content. Within one year after vasectomy, sixty to seventy percent of those vasectomized develop antisperm antibodies.[4] In some cases, vasitis nodosa, a benign proliferation of the ductular epithelium, can also result.[5][6] The accumulation of sperm increases pressure in the vas deferens and epididymis. The entry of the sperm into the scrotum can cause sperm granulomas to be formed by the body to contain and absorb the sperm which the body will treat as a foreign biological substance (much like a virus or bacterium).[7]
Efficacy[edit]
| Frequency | Risk | Source |
|---|---|---|
| 1 in 1400 | Unwanted pregnancy (failure of vasectomy) | [8] |
| 1 in 11 | For comparison: unwanted pregnancy w/ typical use of pill | [2] |
| 1 in 6 | For comparison: unwanted pregnancy w/ typical use of condom | [2] |
| 1 in 40 | Infection after surgery | [9] |
| 1 in 7 | Pain at 7 months after vasectomy | [10] |
| 1 in 110 | Pain at 7 months affecting quality of life | [10] |
Vasectomy is the most effective permanent form of contraception available to males. (Removing the entire vas deferens would very likely be more effective, but it is not something that is regularly done.[11]) In nearly every way that vasectomy can be compared to tubal ligation it has a more positive outlook. Vasectomy is more cost effective, less invasive, has techniques that are emerging that may facilitate easier reversal, and has a much lower risk of postoperative complications.
Early failure rates, i.e. pregnancy within a few months after vasectomy, typically result from unprotected sexual intercourse too soon after the procedure while some sperm continue to pass through the vasa deferentia. Most physicians and surgeons who perform vasectomies recommend one (sometimes two) postprocedural semen specimens to verify a successful vasectomy; however, many people fail to return for verification tests citing inconvenience, embarrassment, forgetfulness, or certainty of sterility.[12] In January 2008, the FDA cleared a home test called SpermCheck Vasectomy that allows patients to perform postvasectomy confirmation tests themselves;[13] however, compliance for postvasectomy semen analysis in general remains low.
Late failure, i.e. pregnancy following spontaneous recanalization of the vasa deferentia, has also been documented.[14] This occurs because the epithelium of the vas deferens (similar to the epithelium of some other human body parts) is capable of regenerating and creating a new tube if the vas deferens is damaged and/or severed.[15] Even when as much as five centimeters (or two inches) of the vas deferens is removed, the vas deferens can still grow back together and become reattached—thus allowing sperm to once again pass and flow through the vas deferens, restoring one’s fertility.[15]
The Royal College of Obstetricians and Gynaecologists states there is a generally agreed-upon rate of late failure of about one in 2000 vasectomies— better than tubal ligations for which the failure rate is one in every 200 to 300 cases.[16] A 2005 review including both early and late failures described a total of 183 recanalizations from 43,642 vasectomies (0.4%), and sixty pregnancies after 92,184 vasectomies (0.07%).[8]
Complications[edit]
Short-term possible complications include infection, bruising and bleeding into the scrotum resulting in a collection of blood known as a hematoma.[17] A study in 2012 demonstrated an infection rate of 2.5% postvasectomy.[9] The stitches on the small incisions required are prone to irritation, though this can be minimized by covering them with gauze or small adhesive bandages. The primary long-term complications are chronic pain conditions or syndromes that can affect any of the scrotal, pelvic or lower-abdominal regions, collectively known as post-vasectomy pain syndrome. Though vasectomy results in increases in circulating immune complexes, these increases are transient. Data based on animal and human studies indicate these changes do not result in increased incidence of atherosclerosis. The risk of testicular cancer is not affected by vasectomy.[18]
In 2014 the AUA reaffirmed that vasectomy is not a risk factor for prostate cancer and that it is not necessary for physicians to routinely discuss prostate cancer in their preoperative counseling of vasectomy patients.[19] There remains ongoing debate regarding whether vasectomy is associated with prostate cancer. A 2017 meta-analysis found no statistically significant increase in risk.[20] A 2019 study of 2.1 million Danish males found that vasectomy increased their incidence of prostate cancer by 15%.[21] A 2020 meta-analysis found that vasectomy increased the incidence by 9%.[22] Other recent studies agree on the 15% increase in risk of developing prostate cancer, but found that people who get a vasectomy are not more likely to die from prostate cancer than those without a vasectomy.[23][24]
Postvasectomy pain[edit]
Post-vasectomy pain syndrome is a chronic and sometimes debilitating condition that may develop immediately or several years after vasectomy.[25] The most robust study of post-vasectomy pain, according to the American Urology Association’s Vasectomy Guidelines 2012 (amended 2015)[26] surveyed people just before their vasectomy and again 7 months later. Of those that responded and who said they did not have any scrotal pain prior to vasectomy, 7% had scrotal pain seven months later which they described as «Mild, a bit of a nuisance», 1.6% had pain that was «Moderate, require painkillers» and 0.9% had pain that was «quite severe and noticeably affecting their quality of life».[10] Post-vasectomy pain can be constant orchialgia or epididymal pain (epididymitis), or it can be pain that occurs only at particular times such as with sexual intercourse, ejaculation, or physical exertion.[7]
Psychological effects[edit]
Approximately 90% are generally reported in reviews as being satisfied with having had a vasectomy,[27] while 7–10% of people regret their decision.[28] For those in relationships, regret was less common when both people in the relationship agreed on the procedure.[29]
Younger people who receive a vasectomy are significantly more likely to regret and seek a reversal of their vasectomy, with one study showing people in their twenties being 12.5 times more likely to undergo a vasectomy reversal later in life (and including some who chose sterilization at a young age). Pre-vasectomy counseling is often emphasised for younger patients.[30][31]
Vasectomy can cause:
- depression,[32][unreliable medical source?][33][unreliable medical source?]
- mental pain,[32][unreliable medical source?][33][unreliable medical source?][34][unreliable medical source?]
- misunderstandings with partners or new partners,[35][unreliable medical source?][34][unreliable medical source?]
- increased thoughts about masculinity,[35][unreliable medical source?]
- thinking about a revasectomy.[34][unreliable medical source?]
Dementia[edit]
An association between vasectomy and primary progressive aphasia, a rare variety of frontotemporal dementia, was reported.[29] However, it is doubtful that there is a causal relationship.[36] The putative mechanism is a cross-reactivity between brain and sperm, including the shared presence of neural surface antigens.[37] In addition, the cytoskeletal tau protein has been found only to exist outside of the CNS in the manchette of sperm.[37]
Procedure[edit]
The traditional incision approach of vasectomy involves numbing of the scrotum with local anesthetic (although some people’s physiology may make access to the vas deferens more difficult in which case general anesthesia may be recommended) after which a scalpel is used to make two small incisions, one on each side of the scrotum at a location that allows the surgeon to bring each vas deferens to the surface for excision. The vasa deferentia are cut (sometimes a section may be removed altogether), separated, and then at least one side is sealed by ligating (suturing), cauterizing (electrocauterization), or clamping.[38] There are several variations to this method that may improve healing, effectiveness, and which help mitigate long-term pain such as post-vasectomy pain syndrome or epididymitis, however the data supporting one over another are limited.[39]
- Fascial interposition: Recanalization of the vas deferens is a known cause of vasectomy failure(s).[40] Fascial interposition («FI»), in which a tissue barrier is placed between the cut ends of the vas by suturing, may help to prevent this type of failure, increasing the overall success rate of vasectomy while leaving the testicular end within the confines of the fascia.[41] The fascia is a fibrous protective sheath that surrounds the vas deferens as well as all other body muscle tissue. This method, when combined with intraluminal cautery (where one or both sides of the vas deferens are electrically «burned» closed to prevent recanalization), has been shown to increase the success rate of vasectomy procedures.
- No-needle anesthesia: Fear of needles for injection of local anesthesia is well known.[42] In 2005, a method of local anesthesia was introduced for vasectomy which allows the surgeon to apply it painlessly with a special jet-injection tool, as opposed to traditional needle application. The numbing agent is forced/pushed onto and deep enough into the scrotal tissue to allow for a virtually pain-free surgery. Lidocaine applied in this manner achieves anesthesia in less than one minute.[citation needed] Initial surveys show a very high satisfaction rate amongst vasectomy patients.[42] Once the effects of no-needle anesthesia set in, the vasectomy procedure is performed in the routine manner. However, unlike in conventional local anesthesia where needles and syringes are used on one patient only, the applicator is not single use and cannot be properly cleaned leading to concerns regarding infection control.
- No-scalpel vasectomy (NSV): Also known as a «key-hole» vasectomy,[38] is a vasectomy in which a sharp hemostat (as opposed to a scalpel) is used to puncture the scrotum. This method has come into widespread use as the resulting smaller «incision» or puncture wound typically limits bleeding and hematomas. Also the smaller wound has less chance of infection, resulting in faster healing times compared to the larger/longer incisions made with a scalpel. The surgical wound created by the no-scalpel method usually does not require stitches. NSV is the most commonly performed type of minimally invasive vasectomy, and both describe the method of vasectomy that leads to access of the vas deferens.[43]
- Open-ended vasectomy: In this procedure the testicular end of the vas deferens is not sealed, which allows continued streaming of sperm into the scrotum. This method may avoid testicular pain resulting from increased back-pressure in the epididymis.[7] Studies suggest that this method may reduce long-term complications such as post-vasectomy pain syndrome.[44][45]
- Vas irrigation: Injections of sterile water or euflavine (which kills sperm) are put into the distal portion of the vas at the time of surgery which then brings about a near-immediate sterile («azoospermatic») condition. The use of euflavine does however, tend to decrease time (or, number of ejaculations) to azoospermia vs. the water irrigation by itself. This additional step in the vasectomy procedure, (and similarly, fascial interposition), has shown positive results but is not as prominently in use, and few surgeons offer it as part of their vasectomy procedure.[39]
Other techniques[edit]
The following vasectomy methods have purportedly had a better chance of later reversal but have seen less use by virtue of known higher failure rates (i.e., recanalization). An earlier clip device, the VasClip, is no longer on the market, due to unacceptably high failure rates.[46][47][48][unreliable medical source?]
The VasClip method, though considered reversible, has had a higher cost and resulted in lower success rates. Also, because the vasa deferentia are not cut or tied with this method, it could technically be classified as other than a vasectomy. Vasectomy reversal (and the success thereof) was conjectured to be higher as it only required removing the Vas-Clip device. This method achieved limited use, and scant reversal data are available.[48]
Vas occlusion techniques[edit]
- Injected plugs: There are two types of injected plugs which can be used to block the vasa deferentia. Medical-grade polyurethane (MPU) or medical-grade silicone rubber (MSR) starts as a liquid polymer that is injected into the vas deferens after which the liquid is clamped in place until is solidifies (usually in a few minutes).[49]
- Intra-vas device: The vasa deferentia can also be occluded by an intra-vas device (IVD). A small cut is made in the lower abdomen after which a soft silicone or urethane plug is inserted into each vas tube thereby blocking (occluding) sperm. This method allows for the vas to remain intact. IVD technique is done in an out-patient setting with local anesthetic, similar to a traditional vasectomy. IVD reversal can be performed under the same conditions making it much less costly than vasovasostomy which can require general anesthesia and longer surgery time.[50]
Both vas occlusion techniques require the same basic patient setup: local anesthesia, puncturing of the scrotal sac for access of the vas, and then plug or injected plug occlusion. The success of the aforementioned vas occlusion techniques is not clear and data are still limited. Studies have shown, however, that the time to achieve sterility is longer than the more prominent techniques mentioned in the beginning of this article. The satisfaction rate of patients undergoing IVD techniques has a high rate of satisfaction with regard to the surgery experience itself.[51]
Recovery[edit]
14 days after vasectomy surgery
Sexual intercourse can usually be resumed in about a week (depending on recovery); however, pregnancy is still possible as long as the sperm count is above zero. Another method of contraception must be relied upon until a sperm count is performed either two months after the vasectomy or after 10–20 ejaculations have occurred.[52]
After a vasectomy, contraceptive precautions must be continued until azoospermia is confirmed. Usually two semen analyses at three and four months are necessary to confirm azoospermia. The British Andrological Society has recommended that a single semen analysis confirming azoospermia after sixteen weeks is sufficient.[53]
Post-vasectomy, testicles will continue to produce sperm cells. As before vasectomy, unused sperm are reabsorbed by the body.[54]
Conceiving after vasectomy[edit]
In order to allow the possibility of reproduction via artificial insemination after vasectomy, some opt for cryopreservation of sperm before sterilization. Dr Allan Pacey, senior lecturer in andrology at Sheffield University and secretary of the British Fertility Society, notes that those he sees for a vasectomy reversal which has not worked express wishing they had known they could have stored sperm. Pacey notes, «The problem is you’re asking a man to foresee a future where he might not necessarily be with his current partner—and that may be quite hard to do when she’s sitting next to you.»[55]
The cost of cryo-preservation (sperm banking) may also be substantially less than alternative vaso-vasectomy procedures, compared to the costs of in-vitro fertilization (IVF) which usually run from $12,000 to $25,000.[56]
Sperm can be aspirated from the testicles or the epididymis, and while there is not enough for successful artificial insemination, there is enough to fertilize an ovum by intracytoplasmic sperm injection. This avoids the problem of antisperm antibodies and may result in a faster pregnancy. IVF may be less costly per cycle than reversal in some health-care systems, but a single IVF cycle is often insufficient for conception. Disadvantages include the need for procedures on the woman, and the standard potential side-effects of IVF for both the mother and the child.[57]
Vasectomy reversal[edit]
Although those considering vasectomies should not think of them as reversible, and most people and their partners are satisfied with the operation,[58][59] life circumstances and outlooks can change, and there is a surgical procedure to reverse vasectomies using vasovasostomy (a form of microsurgery first performed by Earl Owen in 1971[60][61]). Vasovasostomy is effective at achieving pregnancy in a variable percentage of cases, and total out-of-pocket costs in the United States are often upwards of $10,000.[62] The typical success rate of pregnancy following a vasectomy reversal is around 55% if performed within 10 years, and drops to around 25% if performed after 10 years.[63] After reversal, sperm counts and motility are usually much lower than pre-vasectomy levels. There is evidence that those who had a vasectomy may produce more abnormal sperm, which would explain why even a mechanically successful reversal does not always restore fertility.[64][65] The higher rates of aneuploidy and diploidy in the sperm cells of those who have undergone vasectomy reversal may lead to a higher rate of birth defects.[64]
Approximately 2% of men who have undergone vasectomy will undergo a reversal within 10 years of the procedure.[31] Some reasons that people seek vasectomy reversals include wanting a family with a new partner following a relationship breakdown or divorce, their original partner dying and subsequently going on to repartner and to want children, the unexpected death of a child, or a long-standing couple changing their minds some time later, often prompted by situations such as improved finances or existing children approaching the age of school or leaving home.[55] Patients often comment that they never anticipated the possibility of a relationship breakdown or death, or how that might affect their situation at the time of having their vasectomy. A small number of vasectomy reversals are also performed in attempts to relieve post-vasectomy pain syndrome.[66]
Prevalence[edit]
Internationally, vasectomy rates are vastly different.[67] While female sterilisation is the most widely used method worldwide, with 223 million women relying on it, only 28 million women rely on their partner’s vasectomy.[68] In the world’s 69 least developed countries less than 0.1% of males use vasectomies on average. Of 54 African countries, only ten report measurable vasectomy use and only Swaziland, Botswana, and South Africa exceed 0.1% prevalence.[67]
| country | vasectomy usage[67] | notes |
|---|---|---|
| Canada | 22% | «of all women rely on vasectomy» |
| UK | 17% — 21% | only range given |
| New Zealand | 17% — 21% | only range given |
| South Korea | 17% — 21% | only range given |
| Australia | ~10% | |
| Belgium | ~10% | |
| Denmark | ~10% | |
| Spain | ~10% | |
| Switzerland | ~10% | |
| Nepal | 7.8% | |
| Brazil | 5.1% | |
| Colombia | 3.4% | |
| Swaziland | 0.3% | |
| Botswana | 0.4% | |
| South Africa | 0.7% |
In North America and Europe vasectomy usage is on the order of 10% with some countries reaching 20%.[67] Despite its high efficacy, in the United States, vasectomy is utilized less than half the rate of the alternative female tubal ligation.[69] According to the research, vasectomy in the US is least utilized among black and Latino populations, the groups that have the highest rates of female sterilization.[69]
New Zealand, in contrast, has higher levels of vasectomy than tubal ligation. 18% of all males, and 25% of all married males, have had a vasectomy. The age cohort with the highest level of vasectomy was 40–49, where 57% of males had taken it up.[70] Canada, the UK, Bhutan and the Netherlands all have similar levels of uptake.[71]
History[edit]
The first human vasectomies were performed in the late 19th century. The procedure was initially used mainly as a treatment for prostate enlargement and as a eugenic method for sterilizing «degenerates».[72] Vasectomy as a method of voluntary birth control began during the Second World War.[73]
The first recorded vasectomy was performed on a dog in 1823.[73] The first human vasectomies were performed to treat benign prostatic hyperplasia, or enlargement of the prostate. Castration had sometimes been used as a treatment for this condition in the 1880s, but, given the serious side effects, doctors sought alternative treatments. The first to suggest vasectomy as an alternative to castration may have been James Ewing Mears (in 1890), or Jean Casimir Félix Guyon.[72]
The first human vasectomy is thought to have been performed by Reginald Harrison.[73][additional citation(s) needed] By 1900, Harrison reported that he had performed more than 100 vasectomies with no adverse outcomes.[72]
In the late 1890s, vasectomy also came to be proposed as a eugenic measure for the sterilization of men considered unfit to reproduce. The first case report of vasectomy in the United States was in 1897, by A. J. Ochsner, a surgeon in Chicago, in a paper titled, «Surgical treatment of habitual criminals». He believed vasectomy to be a simple, effective means for stemming the tide of racial degeneration widely believed to be occurring.[74][75] In 1902, Harry C. Sharp, the surgeon at the Indiana Reformatory, reported that he had sterilized 42 inmates in an effort to both reduce criminal behavior in those individuals and prevent the birth of future criminals.[76]
Eugen Steinach (1861–1944), an Austrian physician, believed that a unilateral vasectomy (severing only one of the two vasa deferentia) in older individuals could restore general vigor and sexual potency, shrink enlarged prostates, and cure various ailments by somehow boosting the hormonal output of the vasectomized testicle.[77] This surgery, which became very popular in the 1920s, was undertaken by many wealthy individuals, including Sigmund Freud and W. B. Yeats.[78] Since these operations lacked rigorous controlled trials, any rejuvenating effect was likely due to the placebo effect, and with the later development of synthetic injectable hormones, this operation fell out of vogue.[77][79]
Vasectomy began to be regarded as a method of consensual birth control during the Second World War.[73] The first vasectomy program on a national scale was launched in 1954 in India.[80]
The procedure is seldom performed on dogs, with castration remaining the preferred reproductive control option for canines. It is regularly performed on bulls.[81]
Society and culture[edit]
Availability and legality[edit]
Vasectomy costs are (or may be) covered in different countries, as a method of both contraception or population control, with some offering it as a part of a national health insurance. The procedure was generally considered illegal in France until 2001, due to provisions in the Napoleonic Code forbidding «self-mutilation». No French law specifically mentioned vasectomy until a 2001 law on contraception and infanticide permitted the procedure.[82]
The U.S. Affordable Care Act (signed into law in 2010) does not cover vasectomies,[83] although eight states require state-health insurance plans to cover the cost. These include: Illinois, Maryland, New Jersey, New Mexico, New York, Oregon, Vermont and Washington.[84]
In 2014, the Iranian parliament voted for a bill that would ban the procedure.[85]
Tourism[edit]
Medical tourism, where a patient travels to a less-developed location where a procedure is cheaper to save money and combine convalescence with a vacation, is infrequently used for vasectomy due to its low cost, but is more likely to be used for vasectomy reversal. Many hospitals list vasectomy as being available. Medical tourism has been scrutinized by some governments for quality of care and postoperative care issues.[86]
Shooting of Andrew Rynne[edit]
In 1990 Andrew Rynne, chairperson of the Irish Family Planning Association, and the Republic of Ireland’s first vasectomy specialist,[87] was shot by a former client, but he survived. The incident is the subject of a short film, The Vasectomy Doctor, by Paul Webster.[88]
See also[edit]
- Caroline Deys, a noted vasectomy specialist
- List of surgeries by type
- Male contraceptive
- Orchiectomy
- Testicular sperm extraction
- World Vasectomy Day
References[edit]
- ^ Popenoe P (1934). «The progress of eugenic sterilization». Journal of Heredity. 25 (1): 19.
- ^ a b c d Trussell, James (2011). «Contraceptive efficacy». In Hatcher, Robert A.; Trussell, James; Nelson, Anita L.; Cates, Willard Jr.; Kowal, Deborah; Policar, Michael S. (eds.). Contraceptive technology (20th revised ed.). New York: Ardent Media. pp. 779–863. ISBN 978-1-59708-004-0. ISSN 0091-9721. OCLC 781956734. Table 26–1 = Table 3–2 Percentage of women experiencing an unintended pregnancy during the first year of typical use and the first year of perfect use of contraception, and the percentage continuing use at the end of the first year. United States.
- ^ «What Happens When I Get a Vasectomy?». WebMD. Retrieved 7 October 2021.
- ^ Hattikudur, S.; Shanta, S. RAO; Shahani, S.K.; Shastri, P.R.; Thakker, P.V.; Bordekar, A.D. (2009). «Immunological and Clinical Consequences of Vasectomy*». Andrologia. 14 (1): 15–22. doi:10.1111/j.1439-0272.1982.tb03089.x. PMID 7039414. S2CID 10468133.
- ^ Deshpande RB, Deshpande J, Mali BN, Kinare SG (1985). «Vasitis nodosa (a report of 7 cases)». J Postgrad Med. 31 (2): 105–8. PMID 4057111.
- ^ Hirschowitz, L; Rode, J; Guillebaud, J; Bounds, W; Moss, E (1988). «Vasitis nodosa and associated clinical findings». Journal of Clinical Pathology. 41 (4): 419–423. doi:10.1136/jcp.41.4.419. PMC 1141468. PMID 3366928.
- ^ a b c Christiansen C, Sandlow J (2003). «Testicular Pain Following Vasectomy: A Review of Post vasectomy Pain Syndrome». Journal of Andrology. 24 (3): 293–8. doi:10.1002/j.1939-4640.2003.tb02675.x. PMID 12721203.
- ^ a b Griffin, T; Tooher, R; Nowakowski, K; Lloyd, M; Maddern, G (2005). «How Little is Enough? The Evidence for Post-Vasectomy Testing». The Journal of Urology. 174 (1): 29–36. doi:10.1097/01.ju.0000161595.82642.fc. PMID 15947571.
- ^ a b Nevill et al (2013) Surveillance of surgical site infection post vasectomy. Journal of Infection Prevention. January 2013. Vol 14(1) [1]
- ^ a b c Leslie TA; Illing RO; Cranston DW; et al. (2007). «The incidence of chronic scrotal pain after vasectomy: a prospective audit». BJU Int. 100 (6): 1330–3. doi:10.1111/j.1464-410X.2007.07128.x. PMID 17850378. S2CID 23328539.
- ^ «Is it possible to have my entire vas deferens removed? — Vasectomy Questions & Answers | Vasectomy.com». www.vasectomy.com.
- ^ Christensen, R. E.; Maples, D. C. (2005). «Postvasectomy Semen Analysis: Are Men Following Up?». The Journal of the American Board of Family Medicine. 18 (1): 44–47. doi:10.3122/jabfm.18.1.44. PMID 15709063.
- ^ Klotz, Kenneth L.; Coppola, Michael A.; Labrecque, Michel; Brugh Vm, Victor M.; Ramsey, Kim; Kim, Kyung-ah; Conaway, Mark R.; Howards, Stuart S.; Flickinger, Charles J.; Herr, John C. (2008). «Clinical and Consumer Trial Performance of a Sensitive Immunodiagnostic Home Test That Qualitatively Detects Low Concentrations of Sperm Following Vasectomy». The Journal of Urology. 180 (6): 2569–2576. doi:10.1016/j.juro.2008.08.045. PMC 2657845. PMID 18930494.
- ^ Philp, T; Guillebaud, J; Budd, D (1984). «Late failure of vasectomy after two documented analyses showing azoospermic semen». BMJ. 289 (6437): 77–79. doi:10.1136/bmj.289.6437.77. PMC 1441962. PMID 6428685.
- ^ a b Rolnick, H. C. (1924). «Regeneration of the Vas Deferens». Archives of Surgery. 9: 188. doi:10.1001/archsurg.1924.01120070191008.
- ^ Royal College of Obstetricians and Gynaecologists. «Sterilisation for women and men: what you need to know». Archived from the original on 4 January 2011. Retrieved 31 January 2011.
- ^ Yang, Fang; Li, Junjun; Dong, Liang; Tan, Kun; Huang, Xiaopeng; Zhang, Peihai; Liu, Xiaozhang; Chang, Degui; Yu, Xujun (2021). «Review of Vasectomy Complications and Safety Concerns». The World Journal of Men’s Health. 39 (3): 406–418. doi:10.5534/wjmh.200073. ISSN 2287-4208. PMC 8255399. PMID 32777870.
- ^ Schwingl, Pamela J; Guess, Harry A (2000). «Safety and effectiveness of vasectomy». Fertility and Sterility. 73 (5): 923–936. CiteSeerX 10.1.1.494.1247. doi:10.1016/S0015-0282(00)00482-9. PMID 10785217.
- ^ «AUA Responds to Study Linking Vasectomy with Prostate Cancer». American Urological Association. Archived from the original on 31 March 2016. Retrieved 19 March 2016.
- ^ Bhindi, Bimal; Wallis, Christopher J. D.; Nayan, Madhur; Farrell, Ann M.; Trost, Landon W.; Hamilton, Robert J.; Kulkarni, Girish S.; Finelli, Antonio; Fleshner, Neil E.; Boorjian, Stephen A.; Karnes, R. Jeffrey (17 July 2017). «The Association Between Vasectomy and Prostate Cancer: A Systematic Review and Meta-analysis». JAMA Internal Medicine. 177 (9): 1273–1286. doi:10.1001/jamainternmed.2017.2791. PMC 5710573. PMID 28715534.
- ^ Husby, Anders; Wohlfahrt, Jan; Melbye, Mads (1 January 2020). «Vasectomy and Prostate Cancer Risk: A 38-Year Nationwide Cohort Study». Journal of the National Cancer Institute. 112 (1): 71–77. doi:10.1093/jnci/djz099. ISSN 1460-2105. PMID 31119294.
- ^ Cheng, Sheng; Yang, Bo; Xu, Liwei; Zheng, Qiming; Ding, Guoqing; Li, Gonghui (9 August 2020). «Vasectomy and prostate cancer risk: a meta-analysis of prospective studies». Carcinogenesis. 42 (1): 31–37. doi:10.1093/carcin/bgaa086. ISSN 1460-2180. PMID 32772072.
- ^ Seikkula, Heikki; Kaipia, Antti; Hirvonen, Elli; Rantanen, Matti; Pitkäniemi, Janne; Malila, Nea; Boström, Peter J. (February 2020). «Vasectomy and the risk of prostate cancer in a Finnish nationwide population-based cohort». Cancer Epidemiology. 64: 101631. doi:10.1016/j.canep.2019.101631. ISSN 1877-783X. PMID 31760357. S2CID 208276171.
- ^ Xu, Yawei; Li, Lei; Yang, Wuping; Zhang, Kenan; Ma, Kaifang; Xie, Haibiao; Zhou, Jingcheng; Cai, Lin; Gong, Yanqing; Zhang, Zheng; Gong, Kan (29 April 2021). «Association between vasectomy and risk of prostate cancer: a meta-analysis». Prostate Cancer and Prostatic Diseases. 24 (4): 962–975. doi:10.1038/s41391-021-00368-7. ISSN 1476-5608. PMID 33927357. S2CID 233458537.
- ^ Nangia, Ajay K.; Myles, Jonathan L.; Thomas Aj, Anthony J. (2000). «Vasectomy Reversal for the Post-Vasectomy Pain Syndrome: : A Clinical and Histological Evaluation». The Journal of Urology. 164 (6): 1939–1942. doi:10.1016/S0022-5347(05)66923-6. PMID 11061886.
- ^ «Vasectomy Guideline — American Urological Association». www.auanet.org.
- ^ THONNEAU, P.; D’ISLE, BÉATRICE (1990). «Does vasectomy have long-term effects on somatic and psychological health status?». International Journal of Andrology. 13 (6): 419–432. doi:10.1111/j.1365-2605.1990.tb01050.x. PMID 2096110.
- ^ Labrecque, Michel; Paunescu, Cristina; Plesu, Ioana; Stacey, Dawn; Légaré, France (2010). «Evaluation of the effect of a patient decision aid about vasectomy on the decision-making process: a randomized trial». Contraception. 82 (6): 556–562. doi:10.1016/j.contraception.2010.05.003. PMID 21074020.
- ^ a b Köhler TS, Fazili AA, Brannigan RE (August 2009). «Putative health risks associated with vasectomy». Urol. Clin. North Am. 36 (3): 337–45. doi:10.1016/j.ucl.2009.05.004. PMID 19643236.
- ^ POTTS, J.M.; PASQUALOTTO, F.F.; NELSON, D.; THOMAS, A.J.; AGARWAL, A. (June 1999). «Patient Characteristics Associated with Vasectomy Reversal» (PDF). The Journal of Urology. 161 (6): 1835–1839. doi:10.1016/S0022-5347(05)68819-2. PMID 10332448.
- ^ a b Dohle, Gert R.; Diemer, Thorsten; Kopa, Zsolt; Krausz, Csilla; Giwercman, Aleksander; Jungwirth, Andreas; European Association of Urology Working Group on Male Infertility (January 2012). «European Association of Urology guidelines on vasectomy». European Urology. 61 (1): 159–163. doi:10.1016/j.eururo.2011.10.001. ISSN 1873-7560. PMID 22033172.
- ^ a b No-Reply (4 November 2014). «Psychological Effects of a Vasectomy». Dr. Elist. Retrieved 15 January 2023.
- ^ a b Vogel, Kaitlin. «There’s a Fascinating Connection That Might Exist Between Vasectomies and Depression—Here’s What to Know About It». Parade: Entertainment, Recipes, Health, Life, Holidays. Retrieved 15 January 2023.
- ^ a b c shucosmetic (29 June 2013). «Psychological Effects of Vasectomy | Minnesota». Medical Center Minneapolis | Varicose Veins St. Paul | Nail Fungus MN. Retrieved 15 January 2023.
- ^ a b «Emotional Reactions After a Vasectomy». His Choice. Retrieved 15 January 2023.
- ^ Köhler, TS.; Choy, JT.; Fazili, AA.; Koenig, JF.; Brannigan, RE. (November 2012). «A critical analysis of the reported association between vasectomy and frontotemporal dementia». Asian J Androl. 14 (6): 903–4. doi:10.1038/aja.2012.94. PMC 3720109. PMID 23064682.
- ^ a b Rogalski E, Weintraub S, Mesulam MM (2013). «Are there susceptibility factors for primary progressive aphasia?». Brain Lang. 127 (2): 135–8. doi:10.1016/j.bandl.2013.02.004. PMC 3740011. PMID 23489582.
- ^ a b Cook, LA; Pun, A; Gallo, MF; Lopez, LM; Van Vliet, HA (30 March 2014). «Scalpel versus no-scalpel incision for vasectomy». The Cochrane Database of Systematic Reviews. 2014 (3): CD004112. doi:10.1002/14651858.CD004112.pub4. PMC 6464377. PMID 24683021.
- ^ a b Cook, Lynley A.; Van Vliet, Huib AAM; Lopez, Laureen M; Pun, Asha; Gallo, Maria F (2014). Cook, Lynley A. (ed.). «Vasectomy occlusion techniques for male sterilization». Cochrane Database of Systematic Reviews. 2014 (2): CD003991. doi:10.1002/14651858.CD003991.pub4. PMC 7173716. PMID 24683020.
- ^ webmaster@vasectomy-information.com (14 September 2007). «Recanalization of the vas deferens». Vasectomy-information.com. Archived from the original on 4 January 2012. Retrieved 28 December 2011.
- ^ Sokal, David; Irsula, Belinda; Hays, Melissa; Chen-Mok, Mario; Barone, Mark A; Investigator Study, Group (2004). «Vasectomy by ligation and excision, with or without fascial interposition: a randomized controlled trial ISRCTN77781689». BMC Medicine. 2 (1): 6. doi:10.1186/1741-7015-2-6. PMC 406425. PMID 15056388.
- ^ a b Weiss, RS; Li, PS (2005). «No-needle jet anesthetic technique for no-scalpel vasectomy». The Journal of Urology. 173 (5): 1677–80. doi:10.1097/01.ju.0000154698.03817.d4. PMID 15821547. S2CID 13097425.
- ^ Sharlip ID, Belker AM, Honig S, Labrecque M, Marmar JL, Ross LS, Sandlow JI, Sokal DC (December 2012). «Vasectomy: AUA guideline». The Journal of Urology. 188 (6 Suppl): 2482–91. doi:10.1016/j.juro.2012.09.080. PMID 23098786.
- ^ Moss, WM (December 1992). «A comparison of open-end versus closed-end vasectomies: a report on 6220 cases». Contraception. 46 (6): 521–5. doi:10.1016/0010-7824(92)90116-B. PMID 1493712.
- ^ Shapiro, EI; Silber, SJ (November 1979). «Open-ended vasectomy, sperm granuloma, and postvasectomy orchialgia». Fertility and Sterility. 32 (5): 546–50. doi:10.1016/S0015-0282(16)44357-8. PMID 499585.
- ^ Levine, LA; Abern, MR; Lux, MM (2006). «Persistent motile sperm after ligation band vasectomy». The Journal of Urology. 176 (5): 2146–8. doi:10.1016/j.juro.2006.07.028. PMID 17070280.
- ^ «Male Contraception Update for the public — August 2008, 3(8)». Imccoalition.org. Archived from the original on 27 March 2012. Retrieved 28 December 2011.
- ^ a b «VasClip». www.vasweb.com. Archived from the original on 19 October 2011.
- ^ «Injected plugs». MaleContraceptives.org. 27 July 2011. Retrieved 28 December 2011.
- ^ «Intra Vas Device (IVD)». MaleContraceptives.org. Retrieved 28 December 2011.
- ^ Cook, LA; Van Vliet, HA; Lopez, LM; Pun, A; Gallo, MF (30 March 2014). «Vasectomy occlusion techniques for male sterilization». The Cochrane Database of Systematic Reviews. 2014 (3): CD003991. doi:10.1002/14651858.CD003991.pub4. PMC 7173716. PMID 24683020.
- ^ Healthwise Staff (13 May 2010). «Vasectomy Procedure, Effects, Risks, Effectiveness, and More». webmd.com. Retrieved 29 March 2012.
- ^ «Post Vasectomy Semen Analysis». Cambridge IVF. Cambridge IVF. Archived from the original on 26 February 2021. Retrieved 23 October 2015.
- ^ «Vasectomy». University of Miami Health System, Miller School of Medicine. University of Miami Health System, Miller School of Medicine. Retrieved 28 December 2019.
- ^ a b Murphy, Clare. «Divorce fuels vasectomy reversals», BBC News, 18 March 2009. Retrieved 19 September 2012.
- ^ Klein, Amy (20 June 2019). «I.V.F. is Expensive. Here’s How to Bring Down the Cost». The New York Times. Retrieved 8 July 2021.
- ^ Shridharani, Anand; Sandlow, Jay I (2010). «Vasectomy reversal versus IVF with sperm retrieval: which is better?». Current Opinion in Urology. 20 (6): 503–509. doi:10.1097/MOU.0b013e32833f1b35. PMID 20852426. S2CID 42105503.
- ^ Landry E, Ward V (1997). «Perspectives from Couples on the Vasectomy Decision: A Six-Country Study» (PDF). Reproductive Health Matters. (special issue): 58–67. Archived from the original (PDF) on 4 March 2016. Retrieved 17 June 2006.
- ^ Jamieson, D (2002). «A comparison of women’s regret after vasectomy versus tubal sterilization». Obstetrics & Gynecology. 99 (6): 1073–1079. doi:10.1016/S0029-7844(02)01981-6. PMID 12052602. S2CID 6586905.
- ^ «About Vasectomy Reversal». Professor Earl Owen’s homepage. Archived from the original on 6 December 2007. Retrieved 29 November 2007.
- ^ Owen ER (1977). «Microsurgical vasovasostomy: a reliable vasectomy reversal». Urology. 167 (2 Pt 2): 1205. doi:10.1016/S0022-5347(02)80388-3. PMID 11905902.
- ^ Vasectomy Reversal http://www.epigee.org/guide/vasectomy_reversal.html
- ^ Cited in Laurance, Jeremy (2009) «Vasectomy Reversal: First Cut Isn’t Final» in The Independent 30 March 2009 https://www.independent.co.uk/life-style/health-and-families/health-news/vasectomy-reversal-first-cut-isnt-final-1657039.html
- ^ a b Sukcharoen, Nares; Ngeamvijawat, J; Sithipravej, T; Promviengchai, S (2003). «High sex chromosome aneuploidy and diploidy rate of epididymal spermatozoa in obstructive azoospermic men». Journal of Assisted Reproduction and Genetics. 20 (5): 196–203. doi:10.1023/A:1023674110940. PMC 3455301. PMID 12812463.
- ^ Abdelmassih, V.; Balmaceda, JP; Tesarik, J; Abdelmassih, R; Nagy, ZP (2002). «Relationship between time period after vasectomy and the reproductive capacity of sperm obtained by epididymal aspiration». Human Reproduction. 17 (3): 736–740. doi:10.1093/humrep/17.3.736. PMID 11870128.
- ^ Horovitz, D. (February 2012). «Vasectomy reversal provides long-term pain relief for men with the post-vasectomy pain syndrome». Journal of Urology. 187 (2): 613–7. doi:10.1016/j.juro.2011.10.023. PMID 22177173.
- ^ a b c d Jacobstein, Roy (December 2015). «The kindest cut: global need to increase vasectomy availability». The Lancet. Global Health. 3 (12): e733–734. doi:10.1016/S2214-109X(15)00168-0. ISSN 2214-109X. PMID 26545447.
- ^ «Contraceptive Use 2011». UN Department of Economic and Social Affairs, Population Division, 2012. Archived from the original on 28 September 2014. Retrieved 8 October 2017.
- ^ a b Shih G, Turok DK, Parker WJ (April 2011). «Vasectomy: the other (better) form of sterilization». Contraception. 83 (4): 310–5. doi:10.1016/j.contraception.2010.08.019. PMID 21397087.[permanent dead link]
- ^ Sneyd, Mary Jane; Cox, Brian; Paul, Charlotte; Skegg, David C.G. (2001). «High prevalence of vasectomy in New Zealand». Contraception. 64 (3): 155–159. doi:10.1016/S0010-7824(01)00242-6. PMID 11704094.
- ^ Pile, John M.; Barone, Mark A. (2009). «Demographics of Vasectomy—USA and International». Urologic Clinics of North America. 36 (3): 295–305. doi:10.1016/j.ucl.2009.05.006. PMID 19643232.
- ^ a b c Drake, M.J.; Mills, I.W.; Cranston, D. (1999). «On the chequered history of vasectomy». BJU International. 84 (4): 475–481. doi:10.1046/j.1464-410x.1999.00206.x. PMID 10468765. S2CID 20563820.
- ^ a b c d Leavesley, JH (1980). «Brief history of vasectomy». Family Planning Information Service. 1 (5): 2–3. PMID 12336890.
- ^ A.J., Ochsner (1969). «Surgical Treatment of Habitual Criminals». Buck V Bell Documents.
- ^ Carlson, Elof Axel (2011). «The Hoosier Connection: Compulsory Sterilization as Moral Hygiene». In Lombardo, Paul A. (ed.). A Century of Eugenics in America: From the Indiana Experiment to the Human Genome Era. Indiana University Press. p. 19. ISBN 978-0253222695.
- ^ Reilly, Phillip (1991). The Surgical Solution: A History of Involuntary Sterilization in the United States. Johns Hopkins University Press. pp. 30–33.
- ^ a b Schultheiss, Dirk; Engel, Rainer M. (1 November 2003). «G. Frank Lydston (1858–1923) revisited: androgen therapy by testicular implantation in the early twentieth century». World Journal of Urology. 21 (5): 356–363. doi:10.1007/s00345-003-0370-z. ISSN 0724-4983. PMID 14586546. S2CID 12706657.
- ^ Ellmann, Richard (9 May 1985). «Yeats’s Second Puberty». The New York Review of Books. Retrieved 23 August 2017.
- ^ McLaren, Angus (9 March 2012). Reproduction by Design: Sex, Robots, Trees, and Test-Tube Babies in Interwar Britain. University of Chicago Press. ISBN 9780226560694.
- ^ Sharma, Sanjay (April–June 2014). «A Study of Male Sterilization with No Scalpel Vasectomy» (PDF). JK Science. 16 (2): 67. Retrieved 23 October 2015.
- ^ Dean A. Hendrickson; A. N. Baird (5 June 2013). Turner and McIlwraith’s Techniques in Large Animal Surgery. John Wiley & Sons. p. 541. ISBN 978-1-118-68404-7.
- ^ Latham, Melanie (2002). Regulating Reproduction: A Century of Conflict in Britain and France. Manchester University Press. ISBN 978-0-7190-5699-4.
- ^ «Where Can I Buy a Vasectomy & How Much Will It Cost?». Planned Parenthood. Retrieved 30 June 2022.
- ^ «My husband would like to get a vasectomy but when I checked with our insurer, they told me that the plan would cover my sterilization without cost sharing but we would have to pay part of the costs for his procedure. What is the reason for that?». Kaiser Family Foundation. 15 July 2020. Retrieved 30 June 2022.
- ^ Moghtader, Michelle (11 August 2014). «Iranian parliament bans vasectomies in bid to boost birth rate». Reuters. Retrieved 15 July 2018.
- ^ Lunt, Neil; Carrera, Percivil (2010). «Medical tourism: Assessing the evidence on treatment abroad». Maturitas. 66 (1): 27–32. doi:10.1016/j.maturitas.2010.01.017. PMID 20185254.
- ^ «‘I could look down the barrel of the gun. I could see the worm of the gun.’ — RTÉ Radio 1 Highlights».
- ^ Jarlath Regan (26 May 2019). «Dr. Andrew Rynne». An Irishman Abroad (Podcast) (297 ed.). SoundCloud. Archived from the original on 27 May 2019. Retrieved 27 May 2019.
External links[edit]
- MedlinePlus Encyclopedia
- How to treat: vasectomy and reversal, Australian Doctor, 2 July 2014 Archived 10 April 2020 at the Wayback Machine

![]()
Красным обозначено место перевязывания (или удаления фрагмента в данном месте) семявыводящих протоков
Вазэктоми́я (лат. Vas — сосуд, проток + эктомия) — хирургическая операция, при которой производится перевязка или удаление фрагмента семявыносящих протоков (лат. Vas deferens) у мужчин (самцов). Эта операция приводит к стерильности (неспособности иметь потомство) при сохранении половых функций. У мужчины (самца) после вазэктомии сохраняется половое поведение: либидо, эрекция, эякуляция. Но поскольку семявыносящие протоки становятся непроходимы, то в эякуляте отсутствуют сперматозоиды. Внешний вид спермы обычный. Яички сохраняют свои функции. Вазэктомию применяют в качестве радикального средства контрацепции. В медицине обычно рекомендуется мужчинам, обладающим детьми и решившим отказаться от деторождения в будущем. В ветеринарии используют для стерилизации самцов бродячих собак, которые, сохраняя половое поведение, блокируют контакт молодых нестерилизованных самцов с самками, тем самым препятствуя увеличению численности бродячих собак.
После осуществления вазэктомии, сперматозоиды продолжают вырабатываться яичками, но уже не могут покидать тело через половой орган. Сперматозоиды вместе с несущей их жидкостью расщепляются и абсорбируется телом[источник не указан 58 дней].
Не следует путать вазэктомию с кастрацией: при вазэктомии яички сохраняют свои функции.
Содержание
- 1 Законодательство
- 1.1 Россия
- 1.2 Белоруссия
- 2 Примечания
Законодательство
Россия
Гражданам России стерилизация (и вазэктомия, и стерилизация женщины) разрешается только при возрасте выше 35 лет или наличии 2 детей, или при наличии медицинских показаний[1].
Белоруссия
Гражданам Белоруссии стерилизация (и вазэктомия, и стерилизация женщины) разрешается с 18 лет[2].
Примечания
- ↑ Федеральный закон Российской Федерации от 21 ноября 2011 г. N 323-ФЗ «Об основах охраны здоровья граждан в Российской Федерации», статья 57 «Медицинская стерилизация»
- ↑ Закон Республики Беларусь «О здравоохранении», статья 26 «Стерилизация»
|
Методы контрацепции |
||
|---|---|---|
| Естественные методы контрацепции | Температурный метод · Цервикальный метод · Симптотермальный метод · Календарный метод · Прерванный половой акт · Метод лактационной аменореи |
|
| Барьерные методы | Презерватив · Женский презерватив · Диафрагма · Маточный колпачок | |
| Гормональная контрацепция | Комбинированные оральные контрацептивы · Мини-пили · Гормональные инъекции · Гормональные имплантаты · Гормональное кольцо · Гормональный пластырь · Гормональная внутриматочная спираль · Посткоитальная контрацепция | |
| Химические методы | Спермициды · Медьсодержащая внутриматочная спираль | |
| Хирургические методы | Стерилизация мужчины · Стерилизация женщины |

| Вазэктомия | |
|---|---|
|
|
| Фон | |
| Тип | Стерилизация |
| Первое использование | 1899 (эксперименты с 1785) |
| Частота отказов (первый год) | |
| Идеальное использование | 0,10% |
| Обычное использование | 0,15%. «Vas-Clip» почти 1% |
| Использование | |
| Эффект длительности | Постоянный |
| Обратимость | Возможно, но дорого. |
| Напоминания для пользователя | Для проверки требуются два последовательных отрицательных образца спермы нет спермы. |
| Обзор клиники | Все |
| Преимущества и недостатки | |
| ИППП защита | No |
| Преимущества | Нет необходимости в общей анестезии. Более низкая стоимость и менее инвазивная процедура, чем перевязка маточных труб для женщин. |
| Риски | Временное локальное воспаление яичек, длительная генитальная боль. |
Вазэктомия хирургическая процедура мужской стерилизации или постоянной контрацепции. Во время процедуры мужской семявыносящий проток разрезают и связывают или герметизируют, чтобы предотвратить попадание сперматозоидов в уретру и тем самым предотвратить оплодотворение женщины в результате полового акта. Вазэктомия обычно выполняется в кабинете врача, медицинской клинике или, если она проводится на животном, в ветеринарной клинике — госпитализация обычно не требуется, поскольку процедура не сложна, разрезы небольшие, а необходимое оборудование стандартно.
Существует несколько методов, с помощью которых хирург может завершить процедуру вазэктомии, все из которых перекрывают (т. Е. «Запечатывают») по крайней мере одну сторону каждого семявыносящего протока. Чтобы уменьшить беспокойство и повысить уровень комфорта пациента, мужчины, которые не любят иглы, могут рассмотреть возможность применения анестезии «без иглы», в то время как методы «без скальпеля » или «открытые» методы помогают ускорить время восстановления и увеличивает шанс здорового восстановления.
Из-за простоты операции вазэктомия обычно занимает менее тридцати минут. После непродолжительного выздоровления в кабинете врача (обычно менее часа) пациента отправляют домой для отдыха. Поскольку процедура является минимально инвазивной, многие пациенты после вазэктомии обнаруживают, что они могут возобновить свое типичное сексуальное поведение в течение недели и делают это с небольшим дискомфортом или без него.
Поскольку процедура считается постоянным методом контрацепции и ее нелегко отменить, мужчин обычно консультируют и советуют подумать о том, как отдаленные результаты вазэктомии могут повлиять на них как эмоционально, так и физически. Эта процедура не часто поощряется для молодых одиноких бездетных мужчин, поскольку их шансы на биологическое отцовство тем самым более или менее постоянно снижаются почти до нуля, но в конечном итоге зависит от их собственного комфорта, возможно, желая зачать ребенка от партнера. Это редко выполняется на собаках (кастрация, другая процедура, остается предпочтительным вариантом контроля репродуктивной функции для собак), но регулярно выполняется на быках.
Содержание
- 1 Применение в медицине
- 1.1 Эффективность
- 2 Осложнения
- 2.1 Боль после вазэктомии
- 2.2 Психологические эффекты
- 2.3 Деменция
- 3 Процедура
- 3.1 Другие методы
- 3.1.1 Методы окклюзии сосудов
- 3.2 Восстановление
- 3.1 Другие методы
- 4 Зачатие после вазэктомии
- 4.1 Отмена вазэктомии
- 5 Распространенность
- 6 История
- 7 Общество и культура
- 7.1 Доступность и законность
- 7.2 Идеологические проблемы
- 7.3 Туризм
- 7.4 Стрельба доктора Эндрю Райна
- 8 См. также
- 9 Ссылки
- 10 Внешние ссылки
Использование в медицине
Вазэктомия проводится для предотвращения фертильности у мужчин. Это гарантирует, что в большинстве случаев человек будет бесплодным после подтверждения успеха после операции. Процедура считается постоянной, потому что обратная вазэктомия является дорогостоящей и часто не восстанавливает количество сперматозоидов или подвижность сперматозоидов до уровня предвазэктомии. Мужчины, перенесшие вазэктомию, имеют очень малый (почти нулевой) шанс успешного оплодотворения женщины, но вазэктомия не влияет на частоту инфекций, передаваемых половым путем.
После вазэктомии яички остаются в мошонке, где Лейдиг клетки продолжают вырабатывать тестостерон и другие мужские гормоны, которые продолжают секретироваться в кровоток. Некоторые исследования показали, что сексуальное желание после вазэктомии может несколько уменьшиться.
Когда вазэктомия завершена, сперма не может выйти из организма через пенис. Сперма по-прежнему вырабатывается яичками, но расщепляется и поглощается организмом. Большая часть жидкости поглощается мембранами в придатке яичка, а большая часть твердого содержимого расщепляется отвечающими макрофагами и реабсорбируется через кровоток. Сперма созревает в придатке яичка примерно за месяц, прежде чем выйти из яичек. После вазэктомии мембраны должны увеличиваться в размерах, чтобы впитывать и накапливать больше жидкости; это срабатывание иммунной системы заставляет задействовать больше макрофагов для разрушения и реабсорбции более твердого содержимого. В течение одного года после вазэктомии у 60–70% мужчин, подвергшихся вазэктомии, вырабатываются антиспермальные антитела. В некоторых случаях также может развиться узелковый вазит — доброкачественное разрастание эпителия протоков. Скопление спермы увеличивает давление в семявыносящем протоке и придатке яичка. Попадание сперматозоидов в мошонку может вызвать формирование гранулем сперматозоидов, содержащих и поглощающих сперму, которую организм будет рассматривать как чужеродное биологическое вещество (как вирус или бактерия).
Эффективность
| Частота | Риск | Источник |
|---|---|---|
| 1 из 1400 | Нежелательная беременность (неудачная вазэктомия) | |
| 1 из 11 | Для сравнения: нежелательная беременность с обычным использованием таблетки | |
| 1 из 6 | Для сравнения: нежелательная беременность с обычным использованием презерватива | |
| 1 из 40 | Инфекция после операции | |
| 1 из 7 | Боль через 7 месяцев после вазэктомии | |
| 1 из 110 | Боль через 7 месяцев, влияющая на качество жизни |
Вазэктомия является наиболее эффективной постоянная форма контрацепции, доступная мужчинам. (Удаление всего семявыносящего протока, скорее всего, будет более эффективным, но это не то, что делается регулярно.) Практически во всех отношениях эта вазэктомия может быть сравнена с перевязкой маточных труб, она имеет более позитивные перспективы. Вазэктомия более рентабельна, менее инвазивна, в ней используются новые методы, которые могут способствовать более легкому обращению, и имеет гораздо меньший риск послеоперационных осложнений. Частота неудач на раннем этапе, то есть беременность в течение нескольких месяцев после вазэктомии, обычно возникает в результате незащищенного полового акта слишком скоро после процедуры, когда некоторое количество сперматозоидов продолжает проходить через семявыносящий проток. Большинство врачей и хирургов, выполняющих вазэктомию, рекомендуют один (иногда два) забор спермы после процедуры для проверки успешности вазэктомии; однако многие мужчины не возвращаются на контрольные тесты, ссылаясь на неудобства, смущение, забывчивость или уверенность в бесплодии. В январе 2008 года FDA одобрило домашний тест под названием SpermCheck Vasectomy, который позволяет пациентам самостоятельно выполнять тесты подтверждения после вазэктомии; тем не менее, соблюдение режима поствазэктомического анализа спермы в целом остается низким.
Также была задокументирована поздняя недостаточность, то есть беременность после спонтанной реканализации семявыносящего протока. Это происходит из-за того, что эпителий семявыносящего протока (аналогичный эпителию некоторых других частей тела человека) способен регенерировать и создавать новую трубку в случае повреждения семявыносящего протока и / или разорваны. Даже когда удалено пять сантиметров (или два дюймов ) семявыносящего протока, семявыносящие протоки могут снова срастаться и снова прикрепляться, что позволяет сперматозоидам снова срастаться. проходят и протекают по семявыносящему протоку, восстанавливая фертильность.
Королевский колледж акушеров и гинекологов заявляет, что, по общему мнению, частота поздних неудач составляет примерно одну вазэктомию на 2000 — лучше, чем перевязка маточных труб, для которой частота неудач составляет 1 на каждые 200–300 случаев. Обзор 2005 года, включающий как ранние, так и поздние неудачи, описал в общей сложности 183 реканализации после 43 642 вазэктомий (0,4%) и 60 беременностей после 92 184 вазэктомий (0,07%).
Осложнения
Краткосрочные возможные осложнения включают инфекцию, синяк и кровотечение в мошонку, приводящее к скоплению крови, известному как гематома. Исследование 2012 года показало, что частота инфицирования после вазэктомии составляет 2,5%. Наложение швов на требуемых небольших разрезах склонно к раздражению, хотя это можно свести к минимуму, накрыв их марлей или небольшими пластырями. Первичные долгосрочные осложнения — это состояния или синдромы хронической боли, которые могут поражать любую из областей мошонки, таза или нижней части живота, все вместе известные как болевой синдром после вазэктомии. Хотя вазэктомия приводит к увеличению циркулирующих иммунных комплексов, это увеличение носит временный характер. Данные, основанные на исследованиях на животных и людях, показывают, что эти изменения не приводят к увеличению заболеваемости атеросклерозом. Вазэктомия не влияет на риск рака яичек.
В 2014 году AUA подтвердила, что вазэктомия не является фактором риска рака простаты и что врачам нет необходимости регулярно обсуждать рак простаты во время предоперационного консультирования. пациенты с вазэктомией. Продолжаются дискуссии о том, связана ли вазэктомия с раком простаты. Мета-анализ 2017 года не выявил статистически значимого увеличения риска. Исследование, проведенное в 2019 году с участием 2,1 миллиона датских мужчин, показало, что вазэктомия увеличила заболеваемость раком простаты на 15%. Метаанализ 2020 года показал, что вазэктомия увеличивает частоту рака простаты на 9%.
Боль после вазэктомии
Болевой синдром после вазэктомии (PVPS) — это хроническое и иногда изнурительное состояние, которое может развиться сразу или через несколько лет после вазэктомии. Согласно наиболее надежному исследованию боли после вазэктомии, согласно Руководству по вазэктомии Американской ассоциации урологов, 2012 г. (с поправками в 2015 г.), 14,7% респондентов сообщили о впервые возникшей боли в мошонке через 7 месяцев после вазэктомии, при этом 0,9% назвали боль «довольно сильной». и заметно сказывается на качестве их жизни «. Боль может быть постоянной орхиалгией или болью в придатке яичка (эпидидимит ), или это может быть боль, которая возникает только в определенное время, например, при половом акте, эякуляции или физической нагрузке.
Психологические эффекты
В обзорах обычно сообщается, что примерно 90% удовлетворены вазэктомией, а 7–10% мужчин сожалеют о своем решении. Для мужчин, состоящих в отношениях, сожаление было менее распространено, когда оба человека в отношениях согласились на процедуру.
Мужчины, которые были моложе возраста на момент вазэктомии, значительно чаще сожалеют и ищут обратного их вазэктомии, с одним исследованием, показывающим, например, что мужчины в возрасте от двадцати лет в 12,5 раз чаще подвергаются инверсии вазэктомии в более позднем возрасте (включая тех, кто выбрал стерилизацию в молодом возрасте). Поэтому консультирование перед вазэктомией особенно важно для молодых пациентов.
Деменция
Сообщалось о связи между вазэктомией и первичной прогрессирующей афазией, редкой разновидностью лобно-височной деменции. Однако сомнительно, что существует причинно-следственная связь. Предполагаемый механизм — это перекрестная реактивность между мозгом и сперматозоидами, включая общее присутствие поверхностных нейронных антигенов. Кроме того, было обнаружено, что цитоскелетный тау-белок существует только за пределами ЦНС в манжете сперматозоидов.
Процедура
Традиционная Разрезной подход к вазэктомии включает онемение мошонки местным анестетиком (хотя физиология некоторых мужчин может затруднить доступ к семявыносящему протоку, и в этом случае может быть рекомендована общая анестезия), после чего с помощью скальпеля делают два небольших разреза, по одному на каждом сторона мошонки в месте, позволяющем хирургу вывести каждый семявыносящий проток на поверхность для иссечения. Семявыносящий проток разрезают (иногда часть может быть удален полностью), отделяют, а затем, по крайней мере, одну сторону закрывают лигированием (наложение швов ), прижиганием (электрокаутеризацией ) или зажима. Есть несколько вариантов этого метода, которые могут улучшить заживление, эффективность и уменьшить длительную боль, такие как болевой синдром после вазэктомии (PVPS) или эпидидимит, однако данные поддержка друг друга ограничены.
- Фасциальное взаимодействие: Реканализация семявыносящего протока — известная причина неудач вазэктомии. Фасциальная интерпозиция (FI), при которой тканевой барьер помещается между обрезанными концами семявыносящего протока путем наложения швов, может помочь предотвратить этот тип неудачи, увеличивая общую эффективность вазэктомии, оставляя конец яичка в пределах фасция. фасция представляет собой волокнистую защитную оболочку, которая окружает семявыносящий проток, а также все остальные мышечные ткани тела. Было показано, что этот метод в сочетании с внутрипросветной прижиганием (когда одна или обе стороны семявыносящего протока электрически «обожжены» закрытыми, чтобы предотвратить реканализацию), увеличивает вероятность успеха процедур вазэктомии.
- Без иглы анестезия: Боязнь игл для введения местной анестезии хорошо известна. В 2005 году для вазэктомии был внедрен метод местной анестезии, который позволяет хирургу безболезненно применять его с помощью специального инструмента для струйной инъекции, в отличие от традиционного применения иглы. Обезболивающее средство вводится в ткань мошонки достаточно глубоко, чтобы сделать операцию практически безболезненной. Лидокаин, применяемый таким образом, обеспечивает анестезию менее чем за одну минуту. Первоначальные опросы показывают очень высокий уровень удовлетворенности пациентов после вазэктомии. После того, как проявятся эффекты безыгольной анестезии, процедура вазэктомии выполняется в обычном порядке. Однако, в отличие от традиционной местной анестезии, где иглы и шприцы используются только для одного пациента, аппликатор не предназначен для одноразового использования и не может быть должным образом очищен, что вызывает опасения относительно инфекционного контроля.
- Безскальпельная вазэктомия (NSV): Также известная как вазэктомия «замочная скважина» — это вазэктомия, при которой острый гемостат (в отличие от скальпеля) используется для прокола мошонки. Этот метод получил широкое распространение, так как получающаяся в результате меньшая «надрез» или колотая рана обычно ограничивает кровотечение и гематомы. Кроме того, меньшая рана имеет меньшую вероятность инфицирования, что приводит к более быстрому заживлению по сравнению с более крупными / длинными разрезами, сделанными с помощью скальпеля. Хирургическая рана, созданная бесскальпельным методом, обычно не требует наложения швов. NSV — это наиболее часто выполняемый тип минимально инвазивной вазэктомии, и оба описывают метод вазэктомии, который приводит к доступу к семявыносящему протоку.
Открытая вазэктомия
- Открытая вазэктомия: в этой процедуре конец семявыносящего протока яичка не запечатан, что позволяет сперматозоидам продолжать течь в мошонку. Этот метод позволяет избежать боли в яичках, возникающей из-за повышенного давления в придатке яичка. Исследования показывают, что этот метод может уменьшить долгосрочные осложнения, такие как болевой синдром после вазэктомии.
- орошение сосудов: инъекции стерильной воды или эуфлавин (который убивает сперматозоиды) дистальная часть семявыносящего протока во время операции, которая затем вызывает почти немедленное стерильное («азоосперматическое») состояние. Однако использование эуфлавина имеет тенденцию к сокращению времени (или количества) эякуляций до азооспермии по сравнению с орошением водой само по себе. Этот дополнительный шаг в процедуре вазэктомии (и аналогично фасциальная вставка) показал положительные результаты, но не так широко используется, и лишь немногие хирурги предлагают его как часть своей процедуры вазэктомии.
Другие методы
Следующие ниже методы вазэктомии предположительно имеют больше шансов на последующее обращение, но менее широко используются из-за известной более высокой частоты неудач (т. Е. Реканализации). Более раннее зажимное устройство, VasClip, больше не продается из-за неприемлемо высокой частоты отказов.
Метод VasClip, хотя и считается обратимым, имел более высокую стоимость и приводил к более низким показателям успешности. Кроме того, поскольку семявыносящий проток не перерезается и не перевязывается с помощью этого метода, технически он может быть классифицирован не как вазэктомия. Было высказано предположение, что реверсирование вазэктомии (и ее успех) будет выше, поскольку потребовалось только удаление устройства Vas-Clip.
Методы окклюзии сосудов
- Инъекционные заглушки: Существует два типа инъекционных заглушек, которые можно использовать для блокирования семявыносящего протока. Медицинский полиуретан (MPU) или медицинский силиконовый каучук (MSR) начинается с жидкого полимера, который вводится в семявыносящий проток, после чего жидкость зажимается на месте до тех пор, пока не затвердеет (обычно в течение нескольких минут).
- Внутрисосудистое устройство: Семявыносящий проток также можно перекрыть с помощью внутрисосудистого устройства (IVD). В нижней части живота делается небольшой разрез, после чего в каждую семявыносящую трубку вставляется мягкая силиконовая или уретановая пробка, тем самым блокируя (закупоривая) сперму. Этот метод позволяет не повредить семявыносящие протоки. Техника IVD выполняется в амбулаторных условиях под местной анестезией, аналогично традиционной вазэктомии. Реверсирование МПД может быть выполнено в тех же условиях, что делает его гораздо менее затратным, чем вазовазостомия, которая может потребовать общей анестезии и более длительного времени операции.
Оба метода окклюзии сосудов требуют одинаковой базовой настройки пациента: местная анестезия, пункция мошоночного мешка для доступа к семявыносящему каналу, а затем закупорка пробкой или инъекцией пробки. Успех вышеупомянутых методов окклюзии сосудов не ясен, и данные все еще ограничены. Однако исследования показали, что время для достижения бесплодия больше, чем у более известных методов, упомянутых в начале этой статьи. Степень удовлетворенности пациентов, перенесших технику IVD, является высокой степенью удовлетворенности собственно хирургическим опытом.
Восстановление
Разрез наложены швы и выбритая мошонка 14 дней после операции вазэктомии
Половой акт обычно можно возобновить примерно через неделю (в зависимости от выздоровления); однако беременность все еще возможна, если количество сперматозоидов больше нуля. Следует полагаться на другой метод контрацепции до тех пор, пока не будет проведен подсчет сперматозоидов либо через два месяца после вазэктомии, либо после того, как произошло от десяти до двадцати эякуляций.
После вазэктомии меры контрацепции необходимо продолжать до азооспермии подтверждено. Обычно для подтверждения азооспермии необходимы два анализа спермы через три и четыре месяца. Британское андрологическое общество рекомендовало, чтобы одного анализа спермы, подтверждающего азооспермию, через шестнадцать недель было достаточно.
После вазэктомии яички будут продолжать производить сперматозоиды. Как и до вазэктомии, неиспользованные сперматозоиды реабсорбируются организмом.
Зачатие после вазэктомии
Чтобы обеспечить возможность воспроизводства через искусственное оплодотворение после вазэктомии, некоторые мужчины выбирают для криоконсервации спермы перед стерилизацией. Всем мужчинам, перенесшим вазэктомию, рекомендуется рассмотреть возможность замораживания некоторого количества спермы перед процедурой. Доктор Аллан Пейси, старший преподаватель андрологии в Шеффилдском университете и секретарь Британского общества фертильности, отмечает, что мужчины, которых он видит по поводу отмены вазэктомии, которая не сработала, выражают желание, чтобы они знали, что они могли сохранить сперму. Пейси отмечает: «Проблема в том, что вы просите мужчину предвидеть будущее, в котором он не обязательно будет со своим нынешним партнером — а это может быть довольно сложно сделать, когда она сидит рядом с вами».
Стоимость криоконсервации (сперма банковское дело) также может быть значительно меньше, чем при альтернативных процедурах вазо-вазэктомии, по сравнению с затратами на экстракорпоральное оплодотворение (ЭКО), которое обычно достигает 15000 долларов.
Сперма может быть аспирирована из яички или придатки яичка, и хотя их недостаточно для успешного искусственного оплодотворения, их достаточно для оплодотворения яйцеклетки посредством внутрицитоплазматической инъекции сперматозоидов. Это позволяет избежать проблемы антиспермальных антител и может привести к более быстрой беременности. В некоторых системах здравоохранения цикл ЭКО может быть менее затратным, чем обращение вспять, но одного цикла ЭКО часто недостаточно для зачатия. К недостаткам можно отнести необходимость проведения процедур для женщины и стандартные возможные побочные эффекты ЭКО для матери и ребенка.
Отмена вазэктомии
Хотя мужчинам, рассматривающим возможность вазэктомии, не следует думать о них как обратимый, и большинство мужчин и их партнеров довольны операцией, жизненные обстоятельства и перспективы могут измениться, и существует хирургическая процедура для отмены вазэктомии с использованием вазовазостомии (разновидность микрохирургии впервые исполнен Эрлом Оуэном в 1971 году). Вазовазостомия эффективна при достижении беременности в разном проценте случаев, а общие личные расходы в США часто превышают 10 000 долларов. Типичный показатель успешности беременности после отмены вазэктомии составляет около 55%, если она выполняется в течение 10 лет, и снижается примерно до 25%, если она выполняется через 10 лет. После реверсирования количество и подвижность сперматозоидов обычно намного ниже, чем уровни до вазэктомии. Есть свидетельства того, что мужчины, перенесшие вазэктомию, могут производить больше ненормальной спермы, что объясняет, почему даже механически успешное обращение не всегда восстанавливает фертильность. Более высокий уровень анеуплоидии и диплоидии в сперматозоидах мужчин, перенесших обратную вазэктомию, может привести к более высокому уровню врожденных дефектов.
Некоторые причины, по которым мужчины стремление к обратным действиям вазэктомии включает в себя желание семьи с новым партнером после разрыва отношений или развода, смерть их первоначального партнера, а затем переход к новому партнеру и желание детей, неожиданная смерть ребенка или давнишняя пара, передумавшая некоторые время спустя, часто это связано с такими ситуациями, как улучшение финансового положения или приближение существующих детей к школьному возрасту или уход из дома. Пациенты часто отмечают, что они никогда не ожидали разрыва отношений или смерти или как это может повлиять на их ситуацию во время вазэктомии. Небольшое количество обращений вазэктомии также выполняется в попытках облегчить поствазэктомический болевой синдром.
Распространенность
На международном уровне частота вазэктомий сильно различается. В то время как женская стерилизация является наиболее широко используемым методом во всем мире: 223 миллиона женщин полагаются на нее, только 28 миллионов женщин полагаются на вазэктомию своего партнера. В 69 наименее развитых странах мира вазэктомией в среднем пользуются менее 0,1% мужчин. Из 54 африканских стран только десять сообщили об использовании измеримых вазэктомий, и только в Свазиленде, Ботсване и Южной Африке показатель распространенности превышает 0,1%.
| страна | использование вазэктомии | примечания |
|---|---|---|
| Канада | 22% | «всех женщин, прибегающих к вазэктомии» |
| Великобритания | 17% — 21% | только диапазон дан |
| Новая Зеландия | 17% — 21% | задан только диапазон |
| Южная Корея | 17% — 21% | задан только диапазон |
| Австралия | ~ 10% | |
| Бельгия | ~ 10% | |
| Дания | ~ 10% | |
| Испания | ~ 10% | |
| Швейцария | ~ 10% | |
| Свазиленд | 0,3% | |
| Ботсвана | 0,4% | |
| Южная Африка | 0,7% |
В В Северной Америке и Европе использование вазэктомии составляет порядка 10%, а в некоторых странах достигает 20%. Несмотря на свою высокую эффективность, в США вазэктомия используется менее чем вдвое реже, чем альтернативная перевязка маточных труб у женщин . Согласно исследованию, вазэктомия в США меньше всего используется среди чернокожих и латиноамериканцев, групп, которые имеют самый высокий уровень женской стерилизации.
В Новой Зеландии, напротив, уровень вазэктомии выше, чем перевязка маточных труб. 18% всех мужчин и 25% всех женатых мужчин перенесли вазэктомию. Возрастная когорта с наивысшим уровнем вазэктомии составляла 40–49 лет, из них 57% мужчин сделали это. Канада, Великобритания, Бутан и Нидерланды имеют схожие уровни поглощения.
История
Первая зарегистрированная вазэктомия была выполнена собаке в 1823 году. Вскоре после этого Р. Харрисон из Лондона выполнила первую вазэктомию у человека; Однако операция была сделана не для стерилизации, а для того, чтобы вызвать атрофию простаты. Вскоре, однако, считалось, что это принесло пользу евгенике. Первое сообщение о случае вазэктомии в Соединенных Штатах было сделано в 1897 году А.Дж. Окснер, хирург из Чикаго, в статье под названием «Хирургическое лечение обычных преступников». Он считал вазэктомию простым и эффективным средством для сдерживания волны расовой дегенерации, которая, как широко распространено, происходила. В 1902 году Гарри К. Шарп, хирург исправительного учреждения Индианы, сообщил, что он стерилизовал сорок два заключенных, чтобы уменьшить преступное поведение этих людей и предотвратить рождение будущих преступников.
Нет. все вазэктомии выполнялись с целью стерилизации. Евгений Штайнах (1861–1944), австрийский врач, считал, что односторонняя вазэктомия (перерезание только одного из двух семявыносящих протоков) у пожилых мужчин может восстановить общую бодрость и сексуальную потенцию, уменьшать увеличенную простату и лечить различные недуги, каким-то образом повышая гормональный фон вазэктомированного яичка. Эта операция, которая стала очень популярной в 1920-х годах, была предпринята многими богатыми людьми, в том числе Зигмундом Фрейдом и В. Б. Йейтс. Поскольку эти операции не проходили тщательные контролируемые испытания, любой омолаживающий эффект, вероятно, был обусловлен эффектом плацебо, а с последующим развитием синтетических инъекционных гормонов эта операция вышла из моды.
Началась вазэктомия. считаться методом согласованного контроля над рождаемостью во время Второй мировой войны. Первая программа вазэктомии в национальном масштабе была запущена в 1954 году в Индии.
Общество и культура
Доступность и законность
Затраты на вазэктомию покрываются (или могут покрываться) в разных странах, как метод контрацепции или контроля населения, причем некоторые предлагают его как часть национального медицинского страхования. Закон США о доступном медицинском обслуживании не распространяется на вазэктомию. Вазэктомия обычно считалась незаконной в Франции до 2001 года из-за положений Наполеоновского кодекса, запрещающих «членовредительство». Ни в одном французском законе конкретно не упоминается вазэктомия, пока закон о контрацепции и детоубийстве 2001 года не разрешил эту процедуру. В 2014 году иранский парламент проголосовал за законопроект, запрещающий вазэктомию.
Идеологические проблемы
Акцент на «совместной ответственности» был поднят в недавних исследованиях и статьях Терри и Брауна. которые считают большую часть ранних психологических исследований по вазэктомии кажущимися негативными или «подозрительными». В исследовании, основанном на 16 новозеландских мужчинах (выбранных за их энтузиазм в отношении темы вазэктомии), исследователи извлекли из своих интервью основные темы «взятия на себя ответственности» и «вазэктомии как акта незначительного героизма».
Необходимость «нацеливания на вовлечение мужчин в репродуктивную практику и методы контрацепции» исторически поднималась в глобальном масштабе на Международной конференции по народонаселению и развитию (МКНР) в Каире в 1994 г. в связи как с контролем над населением, так и с уменьшением уровней неравенства в «бремени контрацепции», которое традиционно несправедливо возлагает ответственность за контрацепцию на женщин. Вигойя сослался на глобальную «cultura anticonceptiva femenina» — культуру женской контрацепции, где, несмотря на возможность того, что мужчины берут на себя большую ответственность за контрацепцию, практически нигде в мире не существует истинного равенства в контрацептивах.
Critical Исследователи в области здравоохранения подчеркивают положительную идентичность мужчин после вазэктомии, которые они считают «мужчиной, который берет на себя ответственность за противозачаточные средства», и мужчиной, который готов «пожертвовать» своей фертильностью ради партнера и семьи. Часто такого рода отчеты строятся в рамках «контрацептивной экономики» отношений, в которых женщины несут ответственность за контрацепцию до момента операции. Терри отмечает, что мужчина, перенесший вазэктомию, также может означать, что он получает высокую степень благодарности и положительного подкрепления за выбор стерилизации, возможно, больше, чем женщина, которая много лет назад принимала оральный контрацептив или аналогичный препарат.
Туризм
Медицинский туризм, когда пациент едет в менее развитое место, где процедура дешевле, чтобы сэкономить деньги и совместить выздоровление с отпуском, редко используется для вазэктомии из-за его низкой стоимости, но с большей вероятностью будет использоваться для отмены вазэктомии. Многие больницы считают вазэктомию доступной. Некоторые правительства тщательно изучают медицинский туризм с точки зрения качества ухода и вопросов послеоперационного ухода.
Убийство доктора Эндрю Райна
В 1990 году председатель Ирландской ассоциации планирования семьи, а первый специалист по вазэктомии Ирландской Республики, Эндрю Райн, был застрелен бывшим клиентом, но выжил. Об этом инциденте рассказывается в короткометражном фильме Пола Вебстера «Доктор вазэктомии».
См. Также
- Мужские противозачаточные средства
- Гранулема спермы
- Удаление спермы из яичек
- Орхиэктомия
- Список операций по типу
- Всемирный день вазэктомии
Источники
Внешние ссылки
- Энциклопедия MedlinePlus
- Как лечить: вазэктомия и обратное лечение, австралийский врач, 2 июля 2014 г.

Красным обозначено место перевязывания (или удаления фрагмента в данном месте) семявыводящих протоков
Вазэктоми́я (лат. Vas — сосуд, проток + эктомия греч. ἐκτομή — вырезание, усечение) — хирургическая операция, при которой производится перевязка или удаление фрагмента семявыносящих протоков (лат. ductus deferens) у мужчин. Эта операция приводит к стерильности (неспособности иметь потомство) при сохранении половых функций. У мужчины после вазэктомии сохраняется половое поведение: либидо, эрекция, эякуляция. Но непроходимость семявыносящих протоков приводит к отсутствию в эякуляте сперматозоидов (азооспермии). Внешний вид спермы обычный. Яички сохраняют свои функции. Вазэктомию применяют в качестве радикального средства контрацепции. В медицине обычно рекомендуется мужчинам, обладающим детьми и решившим отказаться от деторождения в будущем. В ветеринарии используют для стерилизации самцов бродячих собак, которые, сохраняя половое поведение, блокируют контакт молодых нестерилизованных самцов с самками, тем самым препятствуя увеличению численности бродячих собак.[источник не указан 327 дней]
Не следует путать вазэктомию с кастрацией: при вазэктомии яички сохраняют свои функции.
В одном проценте случаев после проведения вазэктомии функция семявыводящих протоков частично восстанавливается, что может привести к появлению функционирующих сперматозоидов в семенной жидкости.
Содержание
- 1 Законодательство
- 1.1 Белоруссия
- 1.2 Дания
- 1.3 Казахстан
- 1.4 Киргизия
- 1.5 Россия
- 1.6 Украина
- 1.7 Швеция
- 2 Известные личности, подвергшиеся вазэктомии
- 3 Примечания
Законодательство
|
|
Эта статья или раздел описывает ситуацию применительно лишь к одному региону, возможно, нарушая при этом правило о взвешенности изложения. Вы можете помочь Википедии, добавив информацию для других стран и регионов. |
Белоруссия
Гражданам и гостям Белоруссии стерилизация (и вазэктомия, и стерилизация женщины) разрешается с 35 лет или при наличии двух детей или при наличии медицинских показаний в возрасте старше 18 лет[1].
По состоянию на 2009 год этот метод контрацепции в Белоруссии малопопулярен. За 2008 год в Минской области вазэктомия была проведена два раза[2][3].
Дания
Гражданам Дании старше 25 лет стерилизация проводится по разрешению специального комитета или апелляционной комиссии. Женщинам моложе 25 лет стерилизация разрешается в случае, если беременность угрожает их жизни или здоровью. Стерилизация недееспособного может быть проведена по заявке его опекуна в вышеуказанный комитет или апелляционную комиссию[4].
Казахстан
Гражданам Казахстана стерилизация (и вазэктомия, и стерилизация женщины) разрешается только при возрасте выше 35 лет или наличии 2 и более детей, или при наличии медицинских показаний. Проводить стерилизацию разрешается не только организациям здравоохранения, но и физическим лицам, занимающимся частной медицинской практикой и имеющим лицензию на осуществление данной деятельности[5].
Киргизия
Гражданам и гостям Киргизии стерилизация (и вазэктомия, и стерилизация женщины) разрешается с 18 лет[6].
Россия
В связи с ведущейся кампанией по прекращению демографического кризиса и по увеличению рождаемости гражданам России стерилизация (и вазэктомия, и стерилизация женщины) разрешается только при возрасте выше 35 лет или наличии двух и более детей, или при наличии медицинских показаний[7].
Украина
Гражданам и гостям Украины стерилизация (и вазэктомия, и стерилизация женщины) разрешается с 18 лет по медицинским показаниям. Стерилизация недееспособного лица осуществляется только с согласия его опекуна[8].
Швеция
Гражданам Швеции стерилизация (и вазэктомия, и стерилизация женщины) разрешается с 25 лет. В 2012 году стерилизовалось 4 800 граждан, более 2/3 из них — женщины. Цена стерилизации значительно различается в зависимости от округов страны. В большинстве округов она равна 300 шведским кронам. В 8 округах цена — 2400 крон, а на юге страны — 13 200 крон[9].
Известные личности, подвергшиеся вазэктомии
- Пеле, бразильский футболист[10].
- Роналдо, бразильский футболист[11].
- Уильям Холден, популярный американский актёр.
- Крис Хэдфилд, канадский астронавт[12].
- Даг Стенхоуп, американский стендап-комик.
- Оззи Осборн, британский рок-певец[13].
Примечания
- ↑ Закон Республики Беларусь «О здравоохранении», статья 26 «Стерилизация» (10 июля 2012). Проверено 3 мая 2013.
- ↑ На стерилизацию белорусы идут неохотно. Naviny.by (19 мая 2009). Проверено 3 мая 2013.
- ↑ Белорусские мужчины не сторонники стерилизации как средства контрацепции. Комсомольская правда-Украина, 19 мая 2009
- ↑ Law No. 318 on Sterilization and Castration of 13 June 1973, as amended by Law No. 280 of 26 May 1976 (англ.). Popline.org. Проверено 13 мая 2013. Архивировано 21 мая 2013 года.
- ↑ Кодекс Республики Казахстан о здоровье народа и системе здравоохранения с изменениями и дополнениями по состоянию на 08.01.2013 года, статья 103 «Хирургическая стерилизация». online.zakon.kz (8 января 2013). Проверено 3 мая 2013. Архивировано 11 мая 2013 года.
- ↑ Закон Кыргызской республики «Об охране здоровья граждан в Кыргызской Республике». Статья 36 «Применение методов стерилизации». Фонд обязательного медицинского страхования при Правительстве Кыргызской Республики (17 апреля 2009). Проверено 3 мая 2013. Архивировано 11 мая 2013 года.
- ↑ Федеральный закон Российской Федерации от 21 ноября 2011 г. N 323-ФЗ «Об основах охраны здоровья граждан в Российской Федерации», статья 57 «Медицинская стерилизация». Российская газета (21 ноября 2011). Проверено 3 мая 2013.
- ↑ Основы законодательства Украины о здравоохранении, статья 49 (укр.). Официальный сайт Верховной Рады. Верховная Рада (5 января 2013). Проверено 3 мая 2013. Архивировано 11 мая 2013 года.
- ↑ Шведки все чаще выбирают стерилизацию как радикальное средство контрацепции. «Здоровье Украины» (26 декабря 2012). Проверено 3 мая 2013. Архивировано 11 мая 2013 года.
- ↑ 10 подвигов Пеле. «Спортс.Ру» (23 октября 2010). Проверено 9 июля 2017.
- ↑ Легендарного Роналдо стерилизовали. Один из лучших футболистов современности бразилец Роналдо подверг себя вазэктомии и больше не сможет стать отцом. «ПроСпорт» (28 декабря 2010). Проверено 3 мая 2013. Архивировано 11 мая 2013 года.
- ↑ Хэдфилд К. Руководство астронавта по жизни на Земле. — М. Альпина нон-фикшн, 2015.
- ↑ Читать онлайн «Я — Оззи» автора Осборн Оззи — RuLit — Страница 60. www.rulit.me. Проверено 18 декабря 2017.