Contdict.com > Русско латинский переводчик онлайн
ё
й
ъ
ь
Русско-латинский словарь
|
|
|
|
ветрянка:
|
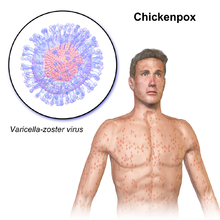
Chickenpox |
Примеры перевода «ветрянка» в контексте:
|
Правая ветрянка воротной вены |
Pullum pox ius porta venam Источник пожаловаться Langcrowd.com |
Популярные направления онлайн-перевода:
Английский-Латынь Английский-Русский Итальянский-Латынь Китайский-Русский Латынь-Английский Латынь-Итальянский Латынь-Немецкий Латынь-Русский Русский-Английский Русский-Китайский
![]()
![]()
![]()
![]()
![]()
![]()
![]()
![]()
![]()
![]()
![]()
© 2023 Contdict.com — онлайн-переводчик
Privacy policy
Terms of use
Contact
ResponsiveVoice-NonCommercial licensed under (CC BY-NC-ND 4.0)
оспа ветряная
-
1
оспаБольшой русско-английский медицинский словарь > оспа
-
2
оспаRussian-english stomatological dctionary > оспа
-
3
оспаРусско-греческий словарь > оспа
-
4
ветряная оспаРусско-английский синонимический словарь > ветряная оспа
-
5
оспаРусско-башкирский словарь > оспа
-
6
ветряная оспаРусско-английский словарь нормативно-технической терминологии > ветряная оспа
-
7
оспаБольшой англо-русский и русско-английский словарь > оспа
-
8
оспаБФРС > оспа
-
9
оспаРусско-английский словарь Смирнитского > оспа
-
10
оспаРусско-английский словарь по общей лексике > оспа
-
11
оспао́сп||а
жἡ εὐλογία, ἡ εὐλογιά, ἡ βλο-γιά:
ветряная оспа ἡ ἀνεμοβλογιά· черная оспа ἡ αίμορραγική εὐλογιά· прививать оспау κάνω ἐμβόλιο κατά τής εὐλογιάς· лицо в оспае πρόσωπο βλογιοκομμένο.
Русско-новогреческий словарь > оспа
-
12
оспаж
1. мед. нағзак; чёрная оспа нағзаки сиёҳ; болеть оспой нағзак баровардан; привить оспу нағзак канондан
2. разг. доғи нағзак <> ветряная оспа гулафшон, гул, нағзак, обакон
Русско-таджикский словарь > оспа
-
13
оспа••
2) buttero м.
* * *
лицо в о́спе — il viso butterato
* * *
n
Universale dizionario russo-italiano > оспа
-
14
оспаРусско-белорусский словарь > оспа
-
15
оспаж
приви́ть о́спу кому-л. — vaccinate (against smallpox)
Американизмы. Русско-английский словарь. > оспа
-
16
оспаНовый русско-итальянский словарь > оспа
-
17
оспа-ы, сущ. ж. I, мн. ч. нет цецг гем, цоохр гем; ветряная оспа цаһан алхц
Русско-калмыцкий словарь > оспа
-
18
оспаРусско-греческий словарь научных и технических терминов > оспа
-
19
ветряная оспаБольшой англо-русский и русско-английский словарь > ветряная оспа
-
20
ветряная оспаБНРС > ветряная оспа
Страницы
- Следующая →
- 1
- 2
- 3
- 4
- 5
- 6
- 7
См. также в других словарях:
-
ОСПА ВЕТРЯНАЯ — мед. Ветряная оспа высококонтагиозное острое вирусное инфекционное заболевание, протекающее с умеренно выраженной интоксикацией и характерной полиморфной сыпью на коже и слизистых оболочках. Этиология Возбудитель ДНК содержащий вирус (Varicella… … Справочник по болезням
-
оспа ветряная — (varicella) острая инфекционная болезнь, вызываемая вирусом ветряной оспы, передающимся воздушно капельным путем; клинически проявляется папуловезикулезной сыпью на коже и повышением температуры; чаще болеют дети до 10 лет … Большой медицинский словарь
-
оспа ветряная — острая инфекционная болезнь, вызываемая вирусом ветряной оспы, передающимся воздушно капельным путем, клинически проявляется папуловезикулезной сыпью на коже и повышением температуры; чаще болеют дети до 10 лет. Источник: Медицинская Популярная… … Медицинские термины
-
Оспа Ветряная (Varicella) — см. Ветрянка. Источник: Медицинский словарь … Медицинские термины
-
ОСПА — ОСПА, оспы, мн. нет, жен. Тяжелая заразная болезнь, сопровождающаяся появлением гнойной сыпи на коже и слизистых оболочках, неизгладимо уродующая кожу. Натуральная оспа. Черная оспа. «В комнату вошел человек лет пятидесяти, с бледным, изрытым… … Толковый словарь Ушакова
-
Ветряная оспа — У этого термина существуют и другие значения, см. Оспа. Ветряная оспа … Википедия
-
ОСПА НАТУРАЛЬНАЯ — мед. Натуральная оспа острая вирусная инфекция, протекавшая с выраженной интоксикацией и кожными высыпаниями. Этиология Возбудитель вирус натуральной оспы рода Orthopoxvirus. Известно 2 штамма вируса: первый вызывает классическую оспу (variola… … Справочник по болезням
-
ветряная оспа — ветрянка (разг.) Словарь синонимов русского языка. Практический справочник. М.: Русский язык. З. Е. Александрова. 2011. ветряная оспа сущ., кол во синонимов: 2 • болезнь … Словарь синонимов
-
ВЕТРЯНАЯ ОСПА — ВЕТРЯНАЯ ОСПА, ветрянка (varicella), представляет собой острое инфекционное заболевание, сопровождающееся пятнисто пузырчатой сыпью. Она контагиозна и при нимает часто эпид. течение. Б нь эта присуща детскому возрасту до 10 лет, у старших детей… … Большая медицинская энциклопедия
-
ОСПА — ОСПА, воспа жен. сыпная повальная болезнь на людей и на животных, напр. на овец, кои мрут от нее поголовно. На людях, оспа бывает: природная, прививная (коровья), и ветряная или ветрянка. Оспа ходит по ночам, с совиными очами, с железным клювом,… … Толковый словарь Даля
-
ВЕТРЯНАЯ ОСПА — острое вирусное заболевание преимущественно детей с лихорадкой и сыпью в виде пузырьков, подсыхающих в корочки. Заражение от больного через воздух … Большой Энциклопедический словарь
| Chickenpox | |
|---|---|
| Other names | Varicella |
 |
|
| A boy presenting with the characteristic blisters of chickenpox | |
| Specialty | Infectious disease |
| Symptoms | Small, itchy blisters, headache, loss of appetite, tiredness, fever[1] |
| Usual onset | 10–21 days after exposure[2] |
| Duration | 5–10 days[1] |
| Causes | Varicella zoster virus[3] |
| Prevention | Varicella vaccine[4] |
| Medication | Calamine lotion, paracetamol (acetaminophen), aciclovir[5] |
| Deaths | 6,400 per year (with shingles)[6] |
Chickenpox, also known as varicella, is a highly contagious disease caused by the initial infection with varicella zoster virus (VZV).[3] The disease results in a characteristic skin rash that forms small, itchy blisters, which eventually scab over.[1] It usually starts on the chest, back, and face.[1] It then spreads to the rest of the body.[1] The rash and other symptoms, such as fever, tiredness, and headaches, usually last five to seven days.[1] Complications may occasionally include pneumonia, inflammation of the brain, and bacterial skin infections.[7] The disease is usually more severe in adults than in children.[8]
Chickenpox is an airborne disease which spreads easily from one person to the next through the coughs and sneezes of an infected person.[5] The incubation period is 10–21 days, after which the characteristic rash appears.[2] It may be spread from one to two days before the rash appears until all lesions have crusted over.[5] It may also spread through contact with the blisters.[5] Those with shingles may spread chickenpox to those who are not immune through contact with the blisters.[5] The disease can usually be diagnosed based on the presenting symptom;[9] however, in unusual cases it may be confirmed by polymerase chain reaction (PCR) testing of the blister fluid or scabs.[8] Testing for antibodies may be done to determine if a person is immune.[8] People usually only get chickenpox once.[5] Although reinfections by the virus occur, these reinfections usually do not cause any symptoms.[10]
Since its introduction in 1995, the varicella vaccine has resulted in a decrease in the number of cases and complications from the disease.[4] It protects about 70–90 percent of people from disease with a greater benefit for severe disease.[8] Routine immunization of children is recommended in many countries.[11] Immunization within three days of exposure may improve outcomes in children.[12] Treatment of those infected may include calamine lotion to help with itching, keeping the fingernails short to decrease injury from scratching, and the use of paracetamol (acetaminophen) to help with fevers.[5] For those at increased risk of complications, antiviral medication such as aciclovir are recommended.[5]
Chickenpox occurs in all parts of the world.[8] In 2013 there were 140 million cases of chickenpox and shingles worldwide.[13] Before routine immunization the number of cases occurring each year was similar to the number of people born.[8] Since immunization the number of infections in the United States has decreased nearly 90%.[8] In 2015 chickenpox resulted in 6,400 deaths globally – down from 8,900 in 1990.[6][14] Death occurs in about 1 per 60,000 cases.[8] Chickenpox was not separated from smallpox until the late 19th century.[8] In 1888 its connection to shingles was determined.[8] The first documented use of the term chicken pox was in 1658.[15] Various explanations have been suggested for the use of «chicken» in the name, one being the relative mildness of the disease.[15]
Signs and symptoms[edit]

A single blister, typical during the early stages of the rash
The early (prodromal) symptoms in adolescents and adults are nausea, loss of appetite, aching muscles, and headache.[16] This is followed by the characteristic rash or oral sores, malaise, and a low-grade fever that signal the presence of the disease. Oral manifestations of the disease (enanthem) not uncommonly may precede the external rash (exanthem). In children the illness is not usually preceded by prodromal symptoms, and the first sign is the rash or the spots in the oral cavity. The rash begins as small red dots on the face, scalp, torso, upper arms and legs; progressing over 10–12 hours to small bumps, blisters and pustules; followed by umbilication and the formation of scabs.[17][18]
At the blister stage, intense itching is usually present. Blisters may also occur on the palms, soles, and genital area. Commonly, visible evidence of the disease develops in the oral cavity and tonsil areas in the form of small ulcers which can be painful or itchy or both; this enanthem (internal rash) can precede the exanthem (external rash) by 1 to 3 days or can be concurrent. These symptoms of chickenpox appear 10 to 21 days after exposure to a contagious person. Adults may have a more widespread rash and longer fever, and they are more likely to experience complications, such as varicella pneumonia.[17]
Because watery nasal discharge containing live virus usually precedes both exanthem (external rash) and enanthem (oral ulcers) by 1 to 2 days, the infected person actually becomes contagious one to two days before recognition of the disease. Contagiousness persists until all vesicular lesions have become dry crusts (scabs), which usually entails four or five days, by which time nasal shedding of live virus ceases.[19] The condition usually resolves by itself within a week or two.[20] The rash may, however, last for up to one month.[medical citation needed][21]
Chickenpox is rarely fatal, although it is generally more severe in adult men than in women or children. Non-immune pregnant women and those with a suppressed immune system are at highest risk of serious complications. Arterial ischemic stroke (AIS) associated with chickenpox in the previous year accounts for nearly one third of childhood AIS.[22] The most common late complication of chickenpox is shingles (herpes zoster), caused by reactivation of the varicella zoster virus decades after the initial, often childhood, chickenpox infection.[21]
-

The back of a 30-year-old male after five days of the rash
-

A 3-year-old girl with a chickenpox rash on her torso
-

Lower leg of a child with chickenpox
-

A child with chickenpox
-

A child with chickenpox on her face.
-

A child with chickenpox
-

Chickenpox blister closeup, day 7 after start of fever







Pregnancy and neonates[edit]
During pregnancy the dangers to the fetus associated with a primary VZV infection are greater in the first six months. In the third trimester, the mother is more likely to have severe symptoms.[23]
For pregnant women, antibodies produced as a result of immunization or previous infection are transferred via the placenta to the fetus.[24]
Varicella infection in pregnant women could lead to spread via the placenta and infection of the fetus. If infection occurs during the first 28 weeks of gestation, this can lead to fetal varicella syndrome (also known as congenital varicella syndrome).[25] Effects on the fetus can range in severity from underdeveloped toes and fingers to severe anal and bladder malformation.[21] Possible problems include:
- Damage to brain: encephalitis,[26] microcephaly, hydrocephaly,[27] aplasia of brain
- Damage to the eye: optic stalk, optic cup, and lens vesicles, microphthalmia, cataracts, chorioretinitis, optic atrophy
- Other neurological disorder: damage to cervical and lumbosacral spinal cord, motor/sensory deficits, absent deep tendon reflexes, anisocoria/Horner’s syndrome
- Damage to body: hypoplasia of upper/lower extremities, anal and bladder sphincter dysfunction
- Skin disorders: (cicatricial) skin lesions, hypopigmentation
Infection late in gestation or immediately following birth is referred to as «neonatal varicella«.[28] Maternal infection is associated with premature delivery. The risk of the baby developing the disease is greatest following exposure to infection in the period 7 days before delivery and up to 8 days following the birth. The baby may also be exposed to the virus via infectious siblings or other contacts, but this is of less concern if the mother is immune. Newborns who develop symptoms are at a high risk of pneumonia and other serious complications of the disease.[29]
Pathophysiology[edit]
Exposure to VZV in a healthy child initiates the production of host immunoglobulin G (IgG), immunoglobulin M (IgM), and immunoglobulin A (IgA) antibodies; IgG antibodies persist for life and confer immunity. Cell-mediated immune responses are also important in limiting the scope and the duration of primary varicella infection. After primary infection, VZV is hypothesized to spread from mucosal and epidermal lesions to local sensory nerves. VZV then remains latent in the dorsal ganglion cells of the sensory nerves. Reactivation of VZV results in the clinically distinct syndrome of herpes zoster (i.e., shingles), postherpetic neuralgia,[30] and sometimes Ramsay Hunt syndrome type II.[31] Varicella zoster can affect the arteries in the neck and head, producing stroke, either during childhood, or after a latency period of many years.[32]
Shingles[edit]
After a chickenpox infection, the virus remains dormant in the body’s nerve tissues for about 50 years. This, however, does not mean that VZV cannot be contracted later in life. The immune system usually keeps the virus at bay, however it can still manifest itself at any given age between 1 and 60, causing a different form of the viral infection called shingles (also known as herpes zoster).[33] Since the human immune system efficacy decreases with age, the United States Advisory Committee on Immunization Practices (ACIP) suggests that every adult over the age of 50 years get the herpes zoster vaccine.[34]
Shingles affects one in five adults infected with chickenpox as children, especially those who are immune-suppressed, particularly from cancer, HIV, or other conditions. Stress can bring on shingles as well, although scientists are still researching the connection.[35] Adults over the age of 60 who had chickenpox but not shingles are the most prone age demographic.[36]
Diagnosis[edit]
The diagnosis of chickenpox is primarily based on the signs and symptoms, with typical early symptoms followed by a characteristic rash. Confirmation of the diagnosis is by examination of the fluid within the vesicles of the rash, or by testing blood for evidence of an acute immunologic response.[37]
Vesicular fluid can be examined with a Tzanck smear, or by testing for direct fluorescent antibody. The fluid can also be «cultured», whereby attempts are made to grow the virus from a fluid sample. Blood tests can be used to identify a response to acute infection (IgM) or previous infection and subsequent immunity (IgG).[38]
Prenatal diagnosis of fetal varicella infection can be performed using ultrasound, though a delay of 5 weeks following primary maternal infection is advised. A PCR (DNA) test of the mother’s amniotic fluid can also be performed, though the risk of spontaneous abortion due to the amniocentesis procedure is higher than the risk of the baby’s developing fetal varicella syndrome.[29]
Prevention[edit]
Hygiene measures[edit]
The spread of chickenpox can be prevented by isolating affected individuals. Contagion is by exposure to respiratory droplets, or direct contact with lesions, within a period lasting from three days before the onset of the rash, to four days after the onset of the rash.[39] The chickenpox virus is susceptible to disinfectants, notably chlorine bleach (i.e., sodium hypochlorite). Like all enveloped viruses, it is sensitive to drying, heat and detergents.[21]
Vaccine[edit]
Chickenpox can be prevented by vaccination.[2] The side effects are usually mild, such as some pain or swelling at the injection site.[2]
A live attenuated varicella vaccine, the Oka strain, was developed by Michiaki Takahashi and his colleagues in Japan in the early 1970s.[40] In 1981, Merck & Co. licensed the «Oka» strain of the varicella virus in the United States, and Maurice Hilleman’s team at Merck invented a varicella vaccine in the same year.[41][42][43]
The varicella vaccine is recommended in many countries.[11] Some countries require the varicella vaccination or an exemption before entering elementary school. A second dose is recommended five years after the initial immunization.[44] A vaccinated person is likely to have a milder case of chickenpox if they become infected.[45] Immunization within three days following household contact reduces infection rates and severity in children.[12] Being exposed to chickenpox as an adult (for example, through contact with infected children) may boost immunity to shingles. So it was thought, that when the majority of children are vaccinated against chickenpox, adults might lose this natural boosting, so immunity would drop and more shingles cases would occur.[46] On the other hand, current observations suggest that exposure to children with varicella is not a critical factor in the maintenance of immunity. Multiple subclinical reactivations of varicella zoster virus may occur spontaneously and, despite not causing clinical disease, may still provide an endogenous boost to immunity against zoster.[47]
It is part of the routine immunization schedule in the US.[48] Some European countries include it as part of universal vaccinations in children,[49] but not all countries provide the vaccine.[11] In the UK as of 2014, the vaccine is only recommended in people who are particularly vulnerable to chickenpox. This is to keep the virus in circulation thereby exposing the population to the virus at an early age, when it is less harmful, and to reduce the occurrence of shingles in those who have already had chickenpox by repeated exposure to the virus later in life.[50] In populations that have not been immunized or if immunity is questionable, a clinician may order an enzyme immunoassay. An immunoassay measures the levels of antibodies against the virus that give immunity to a person. If the levels of antibodies are low (low titer) or questionable, reimmunization may be done.[51]
Treatment[edit]
Treatment mainly consists of easing the symptoms. As a protective measure, people are usually required to stay at home while they are infectious to avoid spreading the disease to others. Cutting the fingernails short or wearing gloves may prevent scratching and minimize the risk of secondary infections.[52]
Although there have been no formal clinical studies evaluating the effectiveness of topical application of calamine lotion (a topical barrier preparation containing zinc oxide, and one of the most commonly used interventions), it has an excellent safety profile.[53] Maintaining good hygiene and daily cleaning of skin with warm water can help to avoid secondary bacterial infection;[54] scratching may increase the risk of secondary infection.[55]
Paracetamol (acetaminophen) but not aspirin may be used to reduce fever. Aspirin use by someone with chickenpox may cause serious, sometimes fatal disease of the liver and brain, Reye syndrome. People at risk of developing severe complications who have had significant exposure to the virus may be given intra-muscular varicella zoster immune globulin (VZIG), a preparation containing high titres of antibodies to varicella zoster virus, to ward off the disease.[56][57]
Antivirals are sometimes used.[58][59]
Children[edit]
If aciclovir by mouth is started within 24 hours of rash onset, it decreases symptoms by one day but has no effect on complication rates.[60][61] Use of aciclovir therefore is not currently recommended for individuals with normal immune function. Children younger than 12 years old and older than one month are not meant to receive antiviral drugs unless they have another medical condition which puts them at risk of developing complications.[62]
Treatment of chickenpox in children is aimed at symptoms while the immune system deals with the virus. With children younger than 12 years, cutting fingernails and keeping them clean is an important part of treatment as they are more likely to scratch their blisters more deeply than adults.[63]
Aspirin is highly contraindicated in children younger than 16 years, as it has been related to Reye syndrome.[64]
Adults[edit]
Infection in otherwise healthy adults tends to be more severe.[65] Treatment with antiviral drugs (e.g. aciclovir or valaciclovir) is generally advised, as long as it is started within 24–48 hours from rash onset.[62] Remedies to ease the symptoms of chickenpox in adults are basically the same as those used for children. Adults are more often prescribed antiviral medication, as it is effective in reducing the severity of the condition and the likelihood of developing complications. Adults are advised to increase water intake to reduce dehydration and to relieve headaches. Painkillers such as paracetamol (acetaminophen) are recommended, as they are effective in relieving itching and other symptoms such as fever or pains. Antihistamines relieve itching and may be used in cases where the itching prevents sleep, because they also act as a sedative. As with children, antiviral medication is considered more useful for those adults who are more prone to develop complications. These include pregnant women or people who have a weakened immune system.[66]
Prognosis[edit]
The duration of the visible blistering caused by varicella zoster virus varies in children usually from 4 to 7 days, and the appearance of new blisters begins to subside after the fifth day. Chickenpox infection is milder in young children, and symptomatic treatment, with sodium bicarbonate baths or antihistamine medication may ease itching.
In adults, the disease is more severe,[67] though the incidence is much less common. Infection in adults is associated with greater morbidity and mortality due to pneumonia (either direct viral pneumonia or secondary bacterial pneumonia),[68] bronchitis (either viral bronchitis or secondary bacterial bronchitis),[68] hepatitis,[69] and encephalitis.[70] In particular, up to 10% of pregnant women with chickenpox develop pneumonia, the severity of which increases with onset later in gestation. In England and Wales, 75% of deaths due to chickenpox are in adults.[29] Inflammation of the brain, encephalitis, can occur in immunocompromised individuals, although the risk is higher with herpes zoster.[71] Necrotizing fasciitis is also a rare complication.[72]
Varicella can be lethal to individuals with impaired immunity. The number of people in this high-risk group has increased, due to the HIV epidemic and the increased use of immunosuppressive therapies.[73] Varicella is a particular problem in hospitals when there are patients with immune systems weakened by drugs (e.g., high-dose steroids) or HIV.[74]
Secondary bacterial infection of skin lesions, manifesting as impetigo, cellulitis, and erysipelas, is the most common complication in healthy children. Disseminated primary varicella infection usually seen in the immunocompromised may have high morbidity. Ninety percent of cases of varicella pneumonia occur in the adult population. Rarer complications of disseminated chickenpox include myocarditis, hepatitis, and glomerulonephritis.[75]
Hemorrhagic complications are more common in the immunocompromised or immunosuppressed populations, although healthy children and adults have been affected. Five major clinical syndromes have been described: febrile purpura, malignant chickenpox with purpura, postinfectious purpura, purpura fulminans, and anaphylactoid purpura. These syndromes have variable courses, with febrile purpura being the most benign of the syndromes and having an uncomplicated outcome. In contrast, malignant chickenpox with purpura is a grave clinical condition that has a mortality rate of greater than 70%. The cause of these hemorrhagic chickenpox syndromes is not known.[75]
Epidemiology[edit]
Primary varicella occurs in all countries worldwide. In 2015 chickenpox resulted in 6,400 deaths globally – down from 8,900 in 1990.[6] There were 7,000 deaths in 2013.[14] Varicella is highly transmissible, with an infection rate of 90% in close contacts.[76]
In temperate countries, chickenpox is primarily a disease of children, with most cases occurring during the winter and spring, most likely due to school contact. In such countries it is one of the classic diseases of childhood, with most cases occurring in children up to age 15;[77] most people become infected before adulthood, and 10% of young adults remain susceptible.
In the United States, a temperate country, the Centers for Disease Control and Prevention (CDC) do not require state health departments to report infections of chickenpox, and only 31 states volunteered this information as of 2013.[78] A 2013 study conducted by the social media disease surveillance tool called Sickweather used anecdotal reports of chickenpox infections on social media systems Facebook and Twitter to measure and rank states with the most infections per capita, with Maryland, Tennessee and Illinois in the top three.[79]
In the tropics, chickenpox often occurs in older people and may cause more serious disease.[80] In adults, the pock marks are darker and the scars more prominent than in children.[81]
Society and culture[edit]
Etymology[edit]
How the term chickenpox originated is not clear but it may be due to it being a relatively mild disease.[15] It has been said to be derived from chickpeas, based on resemblance of the vesicles to chickpeas,[15][82][83] or to come from the rash resembling chicken pecks.[83] Other suggestions include the designation chicken for a child (i.e., literally ‘child pox’), a corruption of itching-pox,[82][84] or the idea that the disease may have originated in chickens.[85] Samuel Johnson explained the designation as «from its being of no very great danger».[86]
Intentional exposure[edit]
Because chickenpox is usually more severe in adults than it is in children, some parents deliberately expose their children to the virus, for example by taking them to «chickenpox parties».[87] Doctors say that children are safer getting the vaccine, which is a weakened form of the virus, than getting the disease, which can be fatal or lead to shingles later in life.[87][88][89] Repeated exposure to chickenpox may protect against zoster.[90]
Other animals[edit]
Humans are the only known species that the disease affects naturally.[8] However, chickenpox has been caused in other primates, including chimpanzees[91] and gorillas.[92]
Research[edit]
Sorivudine, a nucleoside analog, has been reported to be effective in the treatment of primary varicella in healthy adults (case reports only), but large-scale clinical trials are still needed to demonstrate its efficacy.[93] There was speculation in 2005 that continuous dosing of aciclovir by mouth for a period of time could eradicate VZV from the host, although further trials were required to discern whether eradication was actually viable.[94]
See also[edit]
- Measles
References[edit]
- ^ a b c d e f «Chickenpox (Varicella) Signs & Symptoms». Centers for Disease Control and Prevention (cdc.gov). 16 November 2011. Archived from the original on 4 February 2015. Retrieved 4 February 2015.
- ^ a b c d «Chickenpox (Varicella) For Healthcare Professionals». Centers for Disease Control and Prevention (cdc.gov). 31 December 2018. Archived from the original on 6 December 2011. Retrieved 1 January 2021.
- ^ a b «Chickenpox (Varicella) Overview». Centers for Disease Control and Prevention (cdc.gov). 16 November 2011. Archived from the original on 4 February 2015. Retrieved 4 February 2015.
- ^ a b «Routine vaccination against chickenpox?». Drug Ther Bull. 50 (4): 42–45. 2012. doi:10.1136/dtb.2012.04.0098. PMID 22495050. S2CID 42875272.
- ^ a b c d e f g h «Chickenpox (Varicella) Prevention & Treatment». cdc.gov. 16 November 2011. Archived from the original on 4 February 2015. Retrieved 4 February 2015.
- ^ a b c GBD 2015 Mortality and Causes of Death Collaborators. (8 October 2016). «Global, regional, and national life expectancy, all-cause mortality, and cause-specific mortality for 249 causes of death, 1980–2015: a systematic analysis for the Global Burden of Disease Study 2015». Lancet. 388 (10053): 1459–1544. doi:10.1016/s0140-6736(16)31012-1. PMC 5388903. PMID 27733281.
- ^ «Chickenpox (Varicella) Complications». Centers for Disease Control and Prevention (cdc.gov). 16 November 2011. Archived from the original on 4 February 2015. Retrieved 4 February 2015.
- ^ a b c d e f g h i j k Atkinson, William (2011). Epidemiology and Prevention of Vaccine-Preventable Diseases (12 ed.). Public Health Foundation. pp. 301–323. ISBN 978-0983263135. Archived from the original on 7 February 2015. Retrieved 4 February 2015.
- ^ «Chickenpox (Varicella) Interpreting Laboratory Tests». cdc.gov. 19 June 2012. Archived from the original on 4 February 2015. Retrieved 4 February 2015.
- ^ Breuer J (2010). «VZV molecular epidemiology». Varicella-zoster Virus. Current Topics in Microbiology and Immunology. Vol. 342. pp. 15–42. doi:10.1007/82_2010_9. ISBN 978-3-642-12727-4. PMID 20229231.
- ^ a b c Flatt, A; Breuer, J (September 2012). «Varicella vaccines». British Medical Bulletin. 103 (1): 115–127. doi:10.1093/bmb/lds019. PMID 22859715.
- ^ a b Macartney, K; Heywood, A; McIntyre, P (23 June 2014). «Vaccines for post-exposure prophylaxis against varicella (chickenpox) in children and adults». The Cochrane Database of Systematic Reviews. 6 (6): CD001833. doi:10.1002/14651858.CD001833.pub3. PMC 7061782. PMID 24954057. S2CID 43465932.
- ^ Global Burden of Disease Study 2013 Collaborators (22 August 2015). «Global, regional, and national incidence, prevalence, and years lived with disability for 301 acute and chronic diseases and injuries in 188 countries, 1990–2013: a systematic analysis for the Global Burden of Disease Study 2013». Lancet. 386 (9995): 743–800. doi:10.1016/s0140-6736(15)60692-4. PMC 4561509. PMID 26063472.
- ^ a b GBD 2013 Mortality and Causes of Death Collaborators (17 December 2014). «Global, regional, and national age-sex specific all-cause and cause-specific mortality for 240 causes of death, 1990-2013: a systematic analysis for the Global Burden of Disease Study 2013». Lancet. 385 (9963): 117–171. doi:10.1016/S0140-6736(14)61682-2. PMC 4340604. PMID 25530442.
- ^ a b c d Oxford University Press (December 2014). «chickenpox, n.» oed.com. Retrieved 4 February 2015.
- ^ «Chickenpox». Mayo Clinic. Retrieved 10 September 2020.
- ^ a b Anthony J Papadopoulos. Dirk M Elston (ed.). «Chickenpox Clinical Presentation». Medscape Reference. Retrieved 4 August 2012.
- ^ «Symptoms of Chickenpox». Chickenpox. NHS Choices. Archived from the original on 18 March 2013. Retrieved 14 March 2013.
- ^ «Chickenpox (Varicella): Clinical Overview». Centers for Disease Control and Prevention. 22 April 2019. Archived from the original on 25 February 2017.
- ^ «Chickenpox (varicella)». Archived from the original on 5 December 2010. Retrieved 6 November 2010.
- ^ a b c d «Chickenpox — Symptoms and causes». Mayo Clinic. Retrieved 27 April 2022.
- ^ Askalan R, Laughlin S, Mayank S, Chan A, MacGregor D, Andrew M, Curtis R, Meaney B, deVeber G (June 2001). «Chickenpox and stroke in childhood: a study of frequency and causation». Stroke. 32 (6): 1257–1262. doi:10.1161/01.STR.32.6.1257. PMID 11387484.
- ^ Heuchan AM, Isaacs D (19 March 2001). «The management of varicella-zoster virus exposure and infection in pregnancy and the newborn period. Australasian Subgroup in Paediatric Infectious Diseases of the Australasian Society for Infectious Diseases». The Medical Journal of Australia. 174 (6): 288–292. doi:10.5694/j.1326-5377.2001.tb143273.x. PMID 11297117. S2CID 37646516. Archived from the original on 12 February 2013.
- ^ Brannon, Heather (22 July 2007). «Chickenpox in Pregnanc». Dermatology. About.com. Archived from the original on 27 July 2009. Retrieved 20 June 2009.
- ^ Boussault P, Boralevi F, Labbe L, Sarlangue J, Taïeb A, Leaute-Labreze C (2007). «Chronic varicella-zoster skin infection complicating the congenital varicella syndrome». Pediatr Dermatol. 24 (4): 429–432. doi:10.1111/j.1525-1470.2007.00471.x. PMID 17845179. S2CID 22389596.
- ^ Matsuo T, Koyama M, Matsuo N (July 1990). «Acute retinal necrosis as a novel complication of chickenpox in adults». Br J Ophthalmol. 74 (7): 443–444. doi:10.1136/bjo.74.7.443. PMC 1042160. PMID 2378860.
- ^ Mazzella M, Arioni C, Bellini C, Allegri AE, Savioli C, Serra G (2003). «Severe hydrocephalus associated with congenital varicella syndrome». Canadian Medical Association Journal. 168 (5): 561–563. PMC 149248. PMID 12615748.
- ^ Sauerbrei A, Wutzler P (December 2001). «Neonatal varicella». J Perinatol. 21 (8): 545–549. doi:10.1038/sj.jp.7210599. PMID 11774017.
- ^ a b c Royal College of Obstetricians and Gynaecologists (September 2007). «Chickenpox in Pregnancy» (PDF). Archived from the original (PDF) on 11 November 2010. Retrieved 22 July 2009.
- ^ Kanbayashi Y, Onishi K, Fukazawa K, Okamoto K, Ueno H, Takagi T, Hosokawa T (2012). «Predictive Factors for Postherpetic Neuralgia Using Ordered Logistic Regression Analysis». The Clinical Journal of Pain. 28 (8): 712–714. doi:10.1097/AJP.0b013e318243ee01. PMID 22209800. S2CID 11980597.
- ^ Pino Rivero V, González Palomino A, Pantoja Hernández CG, Mora Santos ME, Trinidad Ramos G, Blasco Huelva A (2006). «Ramsay-Hunt syndrome associated to unilateral recurrential paralysis». Anales Otorrinolaringologicos Ibero-americanos. 33 (5): 489–494. PMID 17091862.
- ^ Nagel MA, Cohrs RJ, Mahalingam R, Wellish MC, Forghani B, Schiller A, Safdieh JE, Kamenkovich E, Ostrow LW, Levy M, Greenberg B, Russman AN, Katzan I, Gardner CJ, Häusler M, Nau R, Saraya T, Wada H, Goto H, de Martino M, Ueno M, Brown WD, Terborg C, Gilden DH (March 2008). «The varicella zoster virus vasculopathies: clinical, CSF, imaging, and virologic features». Neurology. 70 (11): 853–860. doi:10.1212/01.wnl.0000304747.38502.e8. PMC 2938740. PMID 18332343.
- ^ «Chickenpox». NHS Choices. UK Department of Health. 19 April 2012. Archived from the original on 24 November 2009.
- ^ «Shingles Vaccine». WebMD. Archived from the original on 29 January 2013.
- ^ «An Overview of Shingles». WebMD. Archived from the original on 8 February 2013.
- ^ «Shingles». PubMed Health.
- ^ Ayoade, Folusakin; Kumar, Sandeep (2020), «Varicella Zoster (Chickenpox)», StatPearls, Treasure Island (FL): StatPearls Publishing, PMID 28846365, retrieved 21 October 2020
- ^ Pincus, Matthew R.; McPherson, Richard A.; Henry, John Bernard (2007). «Ch. 54». Henry’s clinical diagnosis and management by laboratory methods (21st ed.). Saunders Elsevier. ISBN 978-1-4160-0287-1.
- ^ Murray, Patrick R.; Rosenthal, Ken S.; Pfaller, Michael A. (2005). Medical Microbiology (5th ed.). Elsevier Mosby. p. 551. ISBN 978-0-323-03303-9., edition (Elsevier), p.
- ^ Gershon, Anne A. (2007), Arvin, Ann; Campadelli-Fiume, Gabriella; Mocarski, Edward; Moore, Patrick S. (eds.), «Varicella-zoster vaccine», Human Herpesviruses: Biology, Therapy, and Immunoprophylaxis, Cambridge: Cambridge University Press, ISBN 978-0-521-82714-0, PMID 21348127, retrieved 6 February 2021
- ^ Tulchinsky, Theodore H. (2018). «Maurice Hilleman: Creator of Vaccines That Changed the World». Case Studies in Public Health: 443–470. doi:10.1016/B978-0-12-804571-8.00003-2. ISBN 9780128045718. PMC 7150172.
- ^ «Chickenpox (Varicella) | History of Vaccines». www.historyofvaccines.org. Retrieved 6 February 2021.
- ^ «Maurice Ralph Hilleman (1919–2005) | The Embryo Project Encyclopedia». embryo.asu.edu. Retrieved 6 February 2021.
- ^ Chaves SS, Gargiullo P, Zhang JX, Civen R, Guris D, Mascola L, Seward JF (2007). «Loss of vaccine-induced immunity to varicella over time». N Engl J Med. 356 (11): 1121–1129. doi:10.1056/NEJMoa064040. PMID 17360990.
- ^ «Chickenpox (varicella) vaccination». NHS Choices. UK Department of Health. 19 April 2012. Archived from the original on 13 July 2010.
- ^ «Chickenpox vaccine FAQs». 23 January 2019.
- ^ «Live Attenuated Varicella Vaccine: Prevention of Varicella and of Zoster». 30 September 2021.
- ^ «Child, Adolescent & «Catch-up» Immunization Schedules». Immunization Schedules. Centers for Disease Control and Prevention. 11 March 2019. Archived from the original on 5 March 2016.
- ^ Carrillo-Santisteve, P; Lopalco, PL (May 2014). «Varicella vaccination: a laboured take-off». Clinical Microbiology and Infection. 20 Suppl 5: 86–91. doi:10.1111/1469-0691.12580. PMID 24494784.
- ^ «Why aren’t children in the UK vaccinated against chickenpox?». NHS. UK National Health Service. 26 June 2018. Archived from the original on 31 July 2018. Retrieved 11 November 2018.
- ^ Leeuwen, Anne (2015). Davis’s comprehensive handbook of laboratory & diagnostic tests with nursing implications. Philadelphia: F.A. Davis Company. p. 1579. ISBN 978-0803644052.
- ^ CDC (28 April 2021). «Chickenpox Prevention and Treatment». Centers for Disease Control and Prevention. Retrieved 27 April 2022.
- ^ Tebruegge M, Kuruvilla M, Margarson I (2006). «Does the use of calamine or antihistamine provide symptomatic relief from pruritus in children with varicella zoster infection?». Arch. Dis. Child. 91 (12): 1035–1036. doi:10.1136/adc.2006.105114. PMC 2082986. PMID 17119083.
- ^ Domino, Frank J. (2007). The 5-Minute Clinical Consult. Lippincott Williams & Wilkins. p. 248. ISBN 978-0-7817-6334-9.
- ^ Brannon, Heather (21 May 2008). Chicken Pox Treatments Archived 26 August 2009 at the Wayback Machine. About.com.
- ^ Parmet S, Lynm C, Glass RM (February 2004). «JAMA patient page. Chickenpox». JAMA. 291 (7): 906. doi:10.1001/jama.291.7.906. PMID 14970070.
- ^ Naus M; et al. (15 October 2006). «Varizig™ as the Varicella Zoster Immune Globulin for the Prevention of Varicella in At-Risk Patients». Canada Communicable Disease Report. 32 (ACS-8). Archived from the original on 17 January 2013.
- ^ Huff JC (January 1988). «Antiviral treatment in chickenpox and herpes zoster». Journal of the American Academy of Dermatology. 18 (1 Pt 2): 204–206. doi:10.1016/S0190-9622(88)70029-8. PMID 3339143.
- ^ Gnann, John W. Jr. (2007). «Chapter 65Antiviral therapy of varicella-zoster virus infections». In Arvin, Ann; et al. (eds.). Human herpesviruses : biology, therapy, and immunoprophylaxis. Cambridge: Cambridge University Press. ISBN 978-0-521-82714-0. Retrieved 20 January 2014.
- ^ Kay, A. B. (2001). «Allergy and allergic diseases. First of two parts». The New England Journal of Medicine. 344 (1): 30–37. doi:10.1056/NEJM200101043440106. PMID 11136958.
- ^ Kay, A. B. (2001). «Allergy and allergic diseases. Second of two parts». The New England Journal of Medicine. 344 (2): 109–113. doi:10.1056/NEJM200101113440206. PMID 11150362.
- ^ a b «Antiviral medications for chickenpox». Archived from the original on 28 December 2010. Retrieved 27 March 2011.
- ^ «Chickenpox in Children Under 12». Retrieved 6 November 2010.
- ^ «Reye’s Syndrome-Topic Overview». Archived from the original on 5 April 2011. Retrieved 27 March 2011.
- ^ Tunbridge AJ, Breuer J, Jeffery KJ (August 2008). «Chickenpox in adults – clinical management». The Journal of Infection. 57 (2): 95–102. doi:10.1016/j.jinf.2008.03.004. PMID 18555533.
- ^ «What is chickenpox?». Retrieved 6 November 2010.
- ^ Baren JM, Henneman PL, Lewis RJ (August 1996). «Primary Varicella in Adults: Pneumonia, Pregnancy, and Hospital Admissions». Annals of Emergency Medicine. 28 (2): 165–169. doi:10.1016/S0196-0644(96)70057-4. PMID 8759580.
- ^ a b Mohsen AH, McKendrick M (May 2003). «Varicella pneumonia in adults». Eur. Respir. J. 21 (5): 886–891. doi:10.1183/09031936.03.00103202. PMID 12765439.
- ^ Anderson, D.R.; Schwartz, J.; Hunter, N.J.; Cottrill, C.; Bissaccia, E.; Klainer, A.S. (1994). «Varicella Hepatitis: A Fatal Case in a Previously Healthy, Immunocompetent Adult». Archives of Internal Medicine. 154 (18): 2101–2106. doi:10.1001/archinte.1994.00420180111013. PMID 8092915.
- ^ Abro AH, Ustadi AM, Das K, Abdou AM, Hussaini HS, Chandra FS (December 2009). «Chickenpox: presentation and complications in adults». Journal of Pakistan Medical Association. 59 (12): 828–831. PMID 20201174. Archived from the original on 20 May 2014. Retrieved 17 April 2013.
- ^ «Definition of Chickenpox». MedicineNet.com. Archived from the original on 28 July 2006. Retrieved 18 August 2006.
- ^ «Is Necrotizing Fasciitis a complication of Chickenpox of Cutaneous Vasculitis?». atmedstu.com. Archived from the original on 15 April 2008. Retrieved 18 January 2008.
- ^ Strangfeld A, Listing J, Herzer P, Liebhaber A, Rockwitz K, Richter C, Zink A (February 2009). «Risk of herpes zoster in patients with rheumatoid arthritis treated with anti-TNF-alpha agents». JAMA. 301 (7): 737–744. doi:10.1001/jama.2009.146. PMID 19224750.
- ^ Weller TH (1997). «Varicella-herpes zoster virus». In Evans AS, Kaslow RA (eds.). Viral Infections of Humans: Epidemiology and Control. Plenum Press. pp. 865–892. ISBN 978-0-306-44855-3.
- ^ a b Chicken Pox Complications Archived 28 April 2008 at the Wayback Machine
- ^ CDC (11 August 2021). «Chickenpox for HCPs». Centers for Disease Control and Prevention. Retrieved 29 March 2022.
- ^ Di Pietrantonj, Carlo; Rivetti, Alessandro; Marchione, Pasquale; Debalini, Maria Grazia; Demicheli, Vittorio (22 November 2021). «Vaccines for measles, mumps, rubella, and varicella in children». The Cochrane Database of Systematic Reviews. 2021 (11): CD004407. doi:10.1002/14651858.CD004407.pub5. ISSN 1469-493X. PMC 8607336. PMID 34806766.
- ^ «Georgia ranks 10th for social media admissions of chickenpox». Archived from the original on 21 June 2013. Retrieved 13 June 2013.
- ^ «Chickenpox in the USA». Archived from the original on 26 July 2013. Retrieved 12 June 2013.
- ^ Wharton M (1996). «The epidemiology of varicella-zoster virus infections». Infect Dis Clin North Am. 10 (3): 571–581. doi:10.1016/S0891-5520(05)70313-5. PMID 8856352.
- ^ «Epidemiology of Varicella Zoster Virus Infection, Epidemiology of VZV Infection, Epidemiology of Chicken Pox, Epidemiology of Shingles». Archived from the original on 13 June 2008. Retrieved 22 April 2008.
- ^ a b Belshe, Robert B. (1984). Textbook of human virology (2nd ed.). Littleton, MA: PSG. p. 829. ISBN 978-0-88416-458-6.
- ^ a b Teri Shors (2011). «Herpesviruses: Varicella Zoster Virus (VZV)». Understanding Viruses (2nd ed.). Jones & Bartlett. p. 459. ISBN 978-0-7637-8553-6.
- ^ Pattison, John; Zuckerman, Arie J.; Banatvala, J.E. (1994). Principles and practice of clinical virology (3rd ed.). Wiley. p. 37. ISBN 978-0-471-93106-5.
- ^ Chicken-pox is recorded in Oxford English Dictionary 2nd ed. since 1684; the OED records several suggested etymologies
- ^ Johnson, Samuel (1839). Dictionary of the English language. London: Williamson. p. 195.
- ^ a b Charles, M.D., Shamard (22 March 2019). «Doctors say Kentucky Gov. Matt Bevin is wrong about ‘chickenpox on purpose’«. NBC News. Retrieved 22 March 2019.
Chickenpox parties were once a popular way for parents to expose their children to the virus so they would get sick, recover and build up immunity to the disease. … Most doctors believe that deliberately infecting a child with the full-blown virus is a bad idea. While chickenpox is mild for most children, it can be a dangerous virus for others – and there’s no way to know which child will have a serious case, experts say.
- ^ «Chicken Pox parties do more harm than good, says doctor». KSLA News 12 Shreveport, Louisiana News Weather & Sports. Archived from the original on 27 January 2012. Retrieved 17 December 2011.
- ^ Committee to Review Adverse Effects of Vaccines; Institute of, Medicine; Stratton, K.; Ford, A.; Rusch, E.; Clayton, E. W. (2011). Adverse Effects of Vaccines: Evidence and Causality. doi:10.17226/13164. ISBN 978-0-309-21435-3. PMID 24624471. S2CID 67935593.
- ^ Ogunjimi, B; Van Damme, P; Beutels, P (2013). «Herpes Zoster Risk Reduction through Exposure to Chickenpox Patients: A Systematic Multidisciplinary Review». PLOS ONE. 8 (6): e66485. Bibcode:2013PLoSO…866485O. doi:10.1371/journal.pone.0066485. PMC 3689818. PMID 23805224.
- ^ Cohen JI, Moskal T, Shapiro M, Purcell RH (December 1996). «Varicella in Chimpanzees». Journal of Medical Virology. 50 (4): 289–292. doi:10.1002/(SICI)1096-9071(199612)50:4<289::AID-JMV2>3.0.CO;2-4. PMID 8950684. S2CID 28842789.
- ^ Myers MG, Kramer LW, Stanberry LR (December 1987). «Varicella in a gorilla». Journal of Medical Virology. 23 (4): 317–322. doi:10.1002/jmv.1890230403. PMID 2826674. S2CID 84875752.
- ^ «Chickenpox Treatment & Management: Approach Considerations, Treatment in Healthy Children, Treatment in Immunocompetent Adults». Medscape emedicine. 3 June 2022.
- ^ Klassen, TP; Hartling, L. (2005). «Acyclovir for treating varicella in otherwise healthy children and adolescents». Cochrane Database of Systematic Reviews. 2011 (4): CD002980. doi:10.1002/14651858.CD002980.pub3. PMC 8407192. PMID 16235308. S2CID 11018303.
External links[edit]
![]()
Wikimedia Commons has media related to Chickenpox.
- Chickenpox at Curlie
- Prevention of Varicella: Recommendations of the Advisory Committee on Immunization Practices (ACIP), 1996
- Antiviral therapy of varicella-zoster virus infections, 2007
- Epidemiology and Prevention of Vaccine-Preventable Diseases: Varicella, US CDC’s «Pink Book»
- Chickenpox at MedlinePlus
| Chickenpox | |
|---|---|
| Other names | Varicella |
|
|
| A boy presenting with the characteristic blisters of chickenpox | |
| Specialty | Infectious disease |
| Symptoms | Small, itchy blisters, headache, loss of appetite, tiredness, fever[1] |
| Usual onset | 10–21 days after exposure[2] |
| Duration | 5–10 days[1] |
| Causes | Varicella zoster virus[3] |
| Prevention | Varicella vaccine[4] |
| Medication | Calamine lotion, paracetamol (acetaminophen), aciclovir[5] |
| Deaths | 6,400 per year (with shingles)[6] |
Chickenpox, also known as varicella, is a highly contagious disease caused by the initial infection with varicella zoster virus (VZV).[3] The disease results in a characteristic skin rash that forms small, itchy blisters, which eventually scab over.[1] It usually starts on the chest, back, and face.[1] It then spreads to the rest of the body.[1] The rash and other symptoms, such as fever, tiredness, and headaches, usually last five to seven days.[1] Complications may occasionally include pneumonia, inflammation of the brain, and bacterial skin infections.[7] The disease is usually more severe in adults than in children.[8]
Chickenpox is an airborne disease which spreads easily from one person to the next through the coughs and sneezes of an infected person.[5] The incubation period is 10–21 days, after which the characteristic rash appears.[2] It may be spread from one to two days before the rash appears until all lesions have crusted over.[5] It may also spread through contact with the blisters.[5] Those with shingles may spread chickenpox to those who are not immune through contact with the blisters.[5] The disease can usually be diagnosed based on the presenting symptom;[9] however, in unusual cases it may be confirmed by polymerase chain reaction (PCR) testing of the blister fluid or scabs.[8] Testing for antibodies may be done to determine if a person is immune.[8] People usually only get chickenpox once.[5] Although reinfections by the virus occur, these reinfections usually do not cause any symptoms.[10]
Since its introduction in 1995, the varicella vaccine has resulted in a decrease in the number of cases and complications from the disease.[4] It protects about 70–90 percent of people from disease with a greater benefit for severe disease.[8] Routine immunization of children is recommended in many countries.[11] Immunization within three days of exposure may improve outcomes in children.[12] Treatment of those infected may include calamine lotion to help with itching, keeping the fingernails short to decrease injury from scratching, and the use of paracetamol (acetaminophen) to help with fevers.[5] For those at increased risk of complications, antiviral medication such as aciclovir are recommended.[5]
Chickenpox occurs in all parts of the world.[8] In 2013 there were 140 million cases of chickenpox and shingles worldwide.[13] Before routine immunization the number of cases occurring each year was similar to the number of people born.[8] Since immunization the number of infections in the United States has decreased nearly 90%.[8] In 2015 chickenpox resulted in 6,400 deaths globally – down from 8,900 in 1990.[6][14] Death occurs in about 1 per 60,000 cases.[8] Chickenpox was not separated from smallpox until the late 19th century.[8] In 1888 its connection to shingles was determined.[8] The first documented use of the term chicken pox was in 1658.[15] Various explanations have been suggested for the use of «chicken» in the name, one being the relative mildness of the disease.[15]
Signs and symptoms[edit]
A single blister, typical during the early stages of the rash
The early (prodromal) symptoms in adolescents and adults are nausea, loss of appetite, aching muscles, and headache.[16] This is followed by the characteristic rash or oral sores, malaise, and a low-grade fever that signal the presence of the disease. Oral manifestations of the disease (enanthem) not uncommonly may precede the external rash (exanthem). In children the illness is not usually preceded by prodromal symptoms, and the first sign is the rash or the spots in the oral cavity. The rash begins as small red dots on the face, scalp, torso, upper arms and legs; progressing over 10–12 hours to small bumps, blisters and pustules; followed by umbilication and the formation of scabs.[17][18]
At the blister stage, intense itching is usually present. Blisters may also occur on the palms, soles, and genital area. Commonly, visible evidence of the disease develops in the oral cavity and tonsil areas in the form of small ulcers which can be painful or itchy or both; this enanthem (internal rash) can precede the exanthem (external rash) by 1 to 3 days or can be concurrent. These symptoms of chickenpox appear 10 to 21 days after exposure to a contagious person. Adults may have a more widespread rash and longer fever, and they are more likely to experience complications, such as varicella pneumonia.[17]
Because watery nasal discharge containing live virus usually precedes both exanthem (external rash) and enanthem (oral ulcers) by 1 to 2 days, the infected person actually becomes contagious one to two days before recognition of the disease. Contagiousness persists until all vesicular lesions have become dry crusts (scabs), which usually entails four or five days, by which time nasal shedding of live virus ceases.[19] The condition usually resolves by itself within a week or two.[20] The rash may, however, last for up to one month.[medical citation needed][21]
Chickenpox is rarely fatal, although it is generally more severe in adult men than in women or children. Non-immune pregnant women and those with a suppressed immune system are at highest risk of serious complications. Arterial ischemic stroke (AIS) associated with chickenpox in the previous year accounts for nearly one third of childhood AIS.[22] The most common late complication of chickenpox is shingles (herpes zoster), caused by reactivation of the varicella zoster virus decades after the initial, often childhood, chickenpox infection.[21]
-
The back of a 30-year-old male after five days of the rash
-
A 3-year-old girl with a chickenpox rash on her torso
-
Lower leg of a child with chickenpox
-
A child with chickenpox
-
A child with chickenpox on her face.
-
A child with chickenpox
-
Chickenpox blister closeup, day 7 after start of fever
Pregnancy and neonates[edit]
During pregnancy the dangers to the fetus associated with a primary VZV infection are greater in the first six months. In the third trimester, the mother is more likely to have severe symptoms.[23]
For pregnant women, antibodies produced as a result of immunization or previous infection are transferred via the placenta to the fetus.[24]
Varicella infection in pregnant women could lead to spread via the placenta and infection of the fetus. If infection occurs during the first 28 weeks of gestation, this can lead to fetal varicella syndrome (also known as congenital varicella syndrome).[25] Effects on the fetus can range in severity from underdeveloped toes and fingers to severe anal and bladder malformation.[21] Possible problems include:
- Damage to brain: encephalitis,[26] microcephaly, hydrocephaly,[27] aplasia of brain
- Damage to the eye: optic stalk, optic cup, and lens vesicles, microphthalmia, cataracts, chorioretinitis, optic atrophy
- Other neurological disorder: damage to cervical and lumbosacral spinal cord, motor/sensory deficits, absent deep tendon reflexes, anisocoria/Horner’s syndrome
- Damage to body: hypoplasia of upper/lower extremities, anal and bladder sphincter dysfunction
- Skin disorders: (cicatricial) skin lesions, hypopigmentation
Infection late in gestation or immediately following birth is referred to as «neonatal varicella«.[28] Maternal infection is associated with premature delivery. The risk of the baby developing the disease is greatest following exposure to infection in the period 7 days before delivery and up to 8 days following the birth. The baby may also be exposed to the virus via infectious siblings or other contacts, but this is of less concern if the mother is immune. Newborns who develop symptoms are at a high risk of pneumonia and other serious complications of the disease.[29]
Pathophysiology[edit]
Exposure to VZV in a healthy child initiates the production of host immunoglobulin G (IgG), immunoglobulin M (IgM), and immunoglobulin A (IgA) antibodies; IgG antibodies persist for life and confer immunity. Cell-mediated immune responses are also important in limiting the scope and the duration of primary varicella infection. After primary infection, VZV is hypothesized to spread from mucosal and epidermal lesions to local sensory nerves. VZV then remains latent in the dorsal ganglion cells of the sensory nerves. Reactivation of VZV results in the clinically distinct syndrome of herpes zoster (i.e., shingles), postherpetic neuralgia,[30] and sometimes Ramsay Hunt syndrome type II.[31] Varicella zoster can affect the arteries in the neck and head, producing stroke, either during childhood, or after a latency period of many years.[32]
Shingles[edit]
After a chickenpox infection, the virus remains dormant in the body’s nerve tissues for about 50 years. This, however, does not mean that VZV cannot be contracted later in life. The immune system usually keeps the virus at bay, however it can still manifest itself at any given age between 1 and 60, causing a different form of the viral infection called shingles (also known as herpes zoster).[33] Since the human immune system efficacy decreases with age, the United States Advisory Committee on Immunization Practices (ACIP) suggests that every adult over the age of 50 years get the herpes zoster vaccine.[34]
Shingles affects one in five adults infected with chickenpox as children, especially those who are immune-suppressed, particularly from cancer, HIV, or other conditions. Stress can bring on shingles as well, although scientists are still researching the connection.[35] Adults over the age of 60 who had chickenpox but not shingles are the most prone age demographic.[36]
Diagnosis[edit]
The diagnosis of chickenpox is primarily based on the signs and symptoms, with typical early symptoms followed by a characteristic rash. Confirmation of the diagnosis is by examination of the fluid within the vesicles of the rash, or by testing blood for evidence of an acute immunologic response.[37]
Vesicular fluid can be examined with a Tzanck smear, or by testing for direct fluorescent antibody. The fluid can also be «cultured», whereby attempts are made to grow the virus from a fluid sample. Blood tests can be used to identify a response to acute infection (IgM) or previous infection and subsequent immunity (IgG).[38]
Prenatal diagnosis of fetal varicella infection can be performed using ultrasound, though a delay of 5 weeks following primary maternal infection is advised. A PCR (DNA) test of the mother’s amniotic fluid can also be performed, though the risk of spontaneous abortion due to the amniocentesis procedure is higher than the risk of the baby’s developing fetal varicella syndrome.[29]
Prevention[edit]
Hygiene measures[edit]
The spread of chickenpox can be prevented by isolating affected individuals. Contagion is by exposure to respiratory droplets, or direct contact with lesions, within a period lasting from three days before the onset of the rash, to four days after the onset of the rash.[39] The chickenpox virus is susceptible to disinfectants, notably chlorine bleach (i.e., sodium hypochlorite). Like all enveloped viruses, it is sensitive to drying, heat and detergents.[21]
Vaccine[edit]
Chickenpox can be prevented by vaccination.[2] The side effects are usually mild, such as some pain or swelling at the injection site.[2]
A live attenuated varicella vaccine, the Oka strain, was developed by Michiaki Takahashi and his colleagues in Japan in the early 1970s.[40] In 1981, Merck & Co. licensed the «Oka» strain of the varicella virus in the United States, and Maurice Hilleman’s team at Merck invented a varicella vaccine in the same year.[41][42][43]
The varicella vaccine is recommended in many countries.[11] Some countries require the varicella vaccination or an exemption before entering elementary school. A second dose is recommended five years after the initial immunization.[44] A vaccinated person is likely to have a milder case of chickenpox if they become infected.[45] Immunization within three days following household contact reduces infection rates and severity in children.[12] Being exposed to chickenpox as an adult (for example, through contact with infected children) may boost immunity to shingles. So it was thought, that when the majority of children are vaccinated against chickenpox, adults might lose this natural boosting, so immunity would drop and more shingles cases would occur.[46] On the other hand, current observations suggest that exposure to children with varicella is not a critical factor in the maintenance of immunity. Multiple subclinical reactivations of varicella zoster virus may occur spontaneously and, despite not causing clinical disease, may still provide an endogenous boost to immunity against zoster.[47]
It is part of the routine immunization schedule in the US.[48] Some European countries include it as part of universal vaccinations in children,[49] but not all countries provide the vaccine.[11] In the UK as of 2014, the vaccine is only recommended in people who are particularly vulnerable to chickenpox. This is to keep the virus in circulation thereby exposing the population to the virus at an early age, when it is less harmful, and to reduce the occurrence of shingles in those who have already had chickenpox by repeated exposure to the virus later in life.[50] In populations that have not been immunized or if immunity is questionable, a clinician may order an enzyme immunoassay. An immunoassay measures the levels of antibodies against the virus that give immunity to a person. If the levels of antibodies are low (low titer) or questionable, reimmunization may be done.[51]
Treatment[edit]
Treatment mainly consists of easing the symptoms. As a protective measure, people are usually required to stay at home while they are infectious to avoid spreading the disease to others. Cutting the fingernails short or wearing gloves may prevent scratching and minimize the risk of secondary infections.[52]
Although there have been no formal clinical studies evaluating the effectiveness of topical application of calamine lotion (a topical barrier preparation containing zinc oxide, and one of the most commonly used interventions), it has an excellent safety profile.[53] Maintaining good hygiene and daily cleaning of skin with warm water can help to avoid secondary bacterial infection;[54] scratching may increase the risk of secondary infection.[55]
Paracetamol (acetaminophen) but not aspirin may be used to reduce fever. Aspirin use by someone with chickenpox may cause serious, sometimes fatal disease of the liver and brain, Reye syndrome. People at risk of developing severe complications who have had significant exposure to the virus may be given intra-muscular varicella zoster immune globulin (VZIG), a preparation containing high titres of antibodies to varicella zoster virus, to ward off the disease.[56][57]
Antivirals are sometimes used.[58][59]
Children[edit]
If aciclovir by mouth is started within 24 hours of rash onset, it decreases symptoms by one day but has no effect on complication rates.[60][61] Use of aciclovir therefore is not currently recommended for individuals with normal immune function. Children younger than 12 years old and older than one month are not meant to receive antiviral drugs unless they have another medical condition which puts them at risk of developing complications.[62]
Treatment of chickenpox in children is aimed at symptoms while the immune system deals with the virus. With children younger than 12 years, cutting fingernails and keeping them clean is an important part of treatment as they are more likely to scratch their blisters more deeply than adults.[63]
Aspirin is highly contraindicated in children younger than 16 years, as it has been related to Reye syndrome.[64]
Adults[edit]
Infection in otherwise healthy adults tends to be more severe.[65] Treatment with antiviral drugs (e.g. aciclovir or valaciclovir) is generally advised, as long as it is started within 24–48 hours from rash onset.[62] Remedies to ease the symptoms of chickenpox in adults are basically the same as those used for children. Adults are more often prescribed antiviral medication, as it is effective in reducing the severity of the condition and the likelihood of developing complications. Adults are advised to increase water intake to reduce dehydration and to relieve headaches. Painkillers such as paracetamol (acetaminophen) are recommended, as they are effective in relieving itching and other symptoms such as fever or pains. Antihistamines relieve itching and may be used in cases where the itching prevents sleep, because they also act as a sedative. As with children, antiviral medication is considered more useful for those adults who are more prone to develop complications. These include pregnant women or people who have a weakened immune system.[66]
Prognosis[edit]
The duration of the visible blistering caused by varicella zoster virus varies in children usually from 4 to 7 days, and the appearance of new blisters begins to subside after the fifth day. Chickenpox infection is milder in young children, and symptomatic treatment, with sodium bicarbonate baths or antihistamine medication may ease itching.
In adults, the disease is more severe,[67] though the incidence is much less common. Infection in adults is associated with greater morbidity and mortality due to pneumonia (either direct viral pneumonia or secondary bacterial pneumonia),[68] bronchitis (either viral bronchitis or secondary bacterial bronchitis),[68] hepatitis,[69] and encephalitis.[70] In particular, up to 10% of pregnant women with chickenpox develop pneumonia, the severity of which increases with onset later in gestation. In England and Wales, 75% of deaths due to chickenpox are in adults.[29] Inflammation of the brain, encephalitis, can occur in immunocompromised individuals, although the risk is higher with herpes zoster.[71] Necrotizing fasciitis is also a rare complication.[72]
Varicella can be lethal to individuals with impaired immunity. The number of people in this high-risk group has increased, due to the HIV epidemic and the increased use of immunosuppressive therapies.[73] Varicella is a particular problem in hospitals when there are patients with immune systems weakened by drugs (e.g., high-dose steroids) or HIV.[74]
Secondary bacterial infection of skin lesions, manifesting as impetigo, cellulitis, and erysipelas, is the most common complication in healthy children. Disseminated primary varicella infection usually seen in the immunocompromised may have high morbidity. Ninety percent of cases of varicella pneumonia occur in the adult population. Rarer complications of disseminated chickenpox include myocarditis, hepatitis, and glomerulonephritis.[75]
Hemorrhagic complications are more common in the immunocompromised or immunosuppressed populations, although healthy children and adults have been affected. Five major clinical syndromes have been described: febrile purpura, malignant chickenpox with purpura, postinfectious purpura, purpura fulminans, and anaphylactoid purpura. These syndromes have variable courses, with febrile purpura being the most benign of the syndromes and having an uncomplicated outcome. In contrast, malignant chickenpox with purpura is a grave clinical condition that has a mortality rate of greater than 70%. The cause of these hemorrhagic chickenpox syndromes is not known.[75]
Epidemiology[edit]
Primary varicella occurs in all countries worldwide. In 2015 chickenpox resulted in 6,400 deaths globally – down from 8,900 in 1990.[6] There were 7,000 deaths in 2013.[14] Varicella is highly transmissible, with an infection rate of 90% in close contacts.[76]
In temperate countries, chickenpox is primarily a disease of children, with most cases occurring during the winter and spring, most likely due to school contact. In such countries it is one of the classic diseases of childhood, with most cases occurring in children up to age 15;[77] most people become infected before adulthood, and 10% of young adults remain susceptible.
In the United States, a temperate country, the Centers for Disease Control and Prevention (CDC) do not require state health departments to report infections of chickenpox, and only 31 states volunteered this information as of 2013.[78] A 2013 study conducted by the social media disease surveillance tool called Sickweather used anecdotal reports of chickenpox infections on social media systems Facebook and Twitter to measure and rank states with the most infections per capita, with Maryland, Tennessee and Illinois in the top three.[79]
In the tropics, chickenpox often occurs in older people and may cause more serious disease.[80] In adults, the pock marks are darker and the scars more prominent than in children.[81]
Society and culture[edit]
Etymology[edit]
How the term chickenpox originated is not clear but it may be due to it being a relatively mild disease.[15] It has been said to be derived from chickpeas, based on resemblance of the vesicles to chickpeas,[15][82][83] or to come from the rash resembling chicken pecks.[83] Other suggestions include the designation chicken for a child (i.e., literally ‘child pox’), a corruption of itching-pox,[82][84] or the idea that the disease may have originated in chickens.[85] Samuel Johnson explained the designation as «from its being of no very great danger».[86]
Intentional exposure[edit]
Because chickenpox is usually more severe in adults than it is in children, some parents deliberately expose their children to the virus, for example by taking them to «chickenpox parties».[87] Doctors say that children are safer getting the vaccine, which is a weakened form of the virus, than getting the disease, which can be fatal or lead to shingles later in life.[87][88][89] Repeated exposure to chickenpox may protect against zoster.[90]
Other animals[edit]
Humans are the only known species that the disease affects naturally.[8] However, chickenpox has been caused in other primates, including chimpanzees[91] and gorillas.[92]
Research[edit]
Sorivudine, a nucleoside analog, has been reported to be effective in the treatment of primary varicella in healthy adults (case reports only), but large-scale clinical trials are still needed to demonstrate its efficacy.[93] There was speculation in 2005 that continuous dosing of aciclovir by mouth for a period of time could eradicate VZV from the host, although further trials were required to discern whether eradication was actually viable.[94]
See also[edit]
- Measles
References[edit]
- ^ a b c d e f «Chickenpox (Varicella) Signs & Symptoms». Centers for Disease Control and Prevention (cdc.gov). 16 November 2011. Archived from the original on 4 February 2015. Retrieved 4 February 2015.
- ^ a b c d «Chickenpox (Varicella) For Healthcare Professionals». Centers for Disease Control and Prevention (cdc.gov). 31 December 2018. Archived from the original on 6 December 2011. Retrieved 1 January 2021.
- ^ a b «Chickenpox (Varicella) Overview». Centers for Disease Control and Prevention (cdc.gov). 16 November 2011. Archived from the original on 4 February 2015. Retrieved 4 February 2015.
- ^ a b «Routine vaccination against chickenpox?». Drug Ther Bull. 50 (4): 42–45. 2012. doi:10.1136/dtb.2012.04.0098. PMID 22495050. S2CID 42875272.
- ^ a b c d e f g h «Chickenpox (Varicella) Prevention & Treatment». cdc.gov. 16 November 2011. Archived from the original on 4 February 2015. Retrieved 4 February 2015.
- ^ a b c GBD 2015 Mortality and Causes of Death Collaborators. (8 October 2016). «Global, regional, and national life expectancy, all-cause mortality, and cause-specific mortality for 249 causes of death, 1980–2015: a systematic analysis for the Global Burden of Disease Study 2015». Lancet. 388 (10053): 1459–1544. doi:10.1016/s0140-6736(16)31012-1. PMC 5388903. PMID 27733281.
- ^ «Chickenpox (Varicella) Complications». Centers for Disease Control and Prevention (cdc.gov). 16 November 2011. Archived from the original on 4 February 2015. Retrieved 4 February 2015.
- ^ a b c d e f g h i j k Atkinson, William (2011). Epidemiology and Prevention of Vaccine-Preventable Diseases (12 ed.). Public Health Foundation. pp. 301–323. ISBN 978-0983263135. Archived from the original on 7 February 2015. Retrieved 4 February 2015.
- ^ «Chickenpox (Varicella) Interpreting Laboratory Tests». cdc.gov. 19 June 2012. Archived from the original on 4 February 2015. Retrieved 4 February 2015.
- ^ Breuer J (2010). «VZV molecular epidemiology». Varicella-zoster Virus. Current Topics in Microbiology and Immunology. Vol. 342. pp. 15–42. doi:10.1007/82_2010_9. ISBN 978-3-642-12727-4. PMID 20229231.
- ^ a b c Flatt, A; Breuer, J (September 2012). «Varicella vaccines». British Medical Bulletin. 103 (1): 115–127. doi:10.1093/bmb/lds019. PMID 22859715.
- ^ a b Macartney, K; Heywood, A; McIntyre, P (23 June 2014). «Vaccines for post-exposure prophylaxis against varicella (chickenpox) in children and adults». The Cochrane Database of Systematic Reviews. 6 (6): CD001833. doi:10.1002/14651858.CD001833.pub3. PMC 7061782. PMID 24954057. S2CID 43465932.
- ^ Global Burden of Disease Study 2013 Collaborators (22 August 2015). «Global, regional, and national incidence, prevalence, and years lived with disability for 301 acute and chronic diseases and injuries in 188 countries, 1990–2013: a systematic analysis for the Global Burden of Disease Study 2013». Lancet. 386 (9995): 743–800. doi:10.1016/s0140-6736(15)60692-4. PMC 4561509. PMID 26063472.
- ^ a b GBD 2013 Mortality and Causes of Death Collaborators (17 December 2014). «Global, regional, and national age-sex specific all-cause and cause-specific mortality for 240 causes of death, 1990-2013: a systematic analysis for the Global Burden of Disease Study 2013». Lancet. 385 (9963): 117–171. doi:10.1016/S0140-6736(14)61682-2. PMC 4340604. PMID 25530442.
- ^ a b c d Oxford University Press (December 2014). «chickenpox, n.» oed.com. Retrieved 4 February 2015.
- ^ «Chickenpox». Mayo Clinic. Retrieved 10 September 2020.
- ^ a b Anthony J Papadopoulos. Dirk M Elston (ed.). «Chickenpox Clinical Presentation». Medscape Reference. Retrieved 4 August 2012.
- ^ «Symptoms of Chickenpox». Chickenpox. NHS Choices. Archived from the original on 18 March 2013. Retrieved 14 March 2013.
- ^ «Chickenpox (Varicella): Clinical Overview». Centers for Disease Control and Prevention. 22 April 2019. Archived from the original on 25 February 2017.
- ^ «Chickenpox (varicella)». Archived from the original on 5 December 2010. Retrieved 6 November 2010.
- ^ a b c d «Chickenpox — Symptoms and causes». Mayo Clinic. Retrieved 27 April 2022.
- ^ Askalan R, Laughlin S, Mayank S, Chan A, MacGregor D, Andrew M, Curtis R, Meaney B, deVeber G (June 2001). «Chickenpox and stroke in childhood: a study of frequency and causation». Stroke. 32 (6): 1257–1262. doi:10.1161/01.STR.32.6.1257. PMID 11387484.
- ^ Heuchan AM, Isaacs D (19 March 2001). «The management of varicella-zoster virus exposure and infection in pregnancy and the newborn period. Australasian Subgroup in Paediatric Infectious Diseases of the Australasian Society for Infectious Diseases». The Medical Journal of Australia. 174 (6): 288–292. doi:10.5694/j.1326-5377.2001.tb143273.x. PMID 11297117. S2CID 37646516. Archived from the original on 12 February 2013.
- ^ Brannon, Heather (22 July 2007). «Chickenpox in Pregnanc». Dermatology. About.com. Archived from the original on 27 July 2009. Retrieved 20 June 2009.
- ^ Boussault P, Boralevi F, Labbe L, Sarlangue J, Taïeb A, Leaute-Labreze C (2007). «Chronic varicella-zoster skin infection complicating the congenital varicella syndrome». Pediatr Dermatol. 24 (4): 429–432. doi:10.1111/j.1525-1470.2007.00471.x. PMID 17845179. S2CID 22389596.
- ^ Matsuo T, Koyama M, Matsuo N (July 1990). «Acute retinal necrosis as a novel complication of chickenpox in adults». Br J Ophthalmol. 74 (7): 443–444. doi:10.1136/bjo.74.7.443. PMC 1042160. PMID 2378860.
- ^ Mazzella M, Arioni C, Bellini C, Allegri AE, Savioli C, Serra G (2003). «Severe hydrocephalus associated with congenital varicella syndrome». Canadian Medical Association Journal. 168 (5): 561–563. PMC 149248. PMID 12615748.
- ^ Sauerbrei A, Wutzler P (December 2001). «Neonatal varicella». J Perinatol. 21 (8): 545–549. doi:10.1038/sj.jp.7210599. PMID 11774017.
- ^ a b c Royal College of Obstetricians and Gynaecologists (September 2007). «Chickenpox in Pregnancy» (PDF). Archived from the original (PDF) on 11 November 2010. Retrieved 22 July 2009.
- ^ Kanbayashi Y, Onishi K, Fukazawa K, Okamoto K, Ueno H, Takagi T, Hosokawa T (2012). «Predictive Factors for Postherpetic Neuralgia Using Ordered Logistic Regression Analysis». The Clinical Journal of Pain. 28 (8): 712–714. doi:10.1097/AJP.0b013e318243ee01. PMID 22209800. S2CID 11980597.
- ^ Pino Rivero V, González Palomino A, Pantoja Hernández CG, Mora Santos ME, Trinidad Ramos G, Blasco Huelva A (2006). «Ramsay-Hunt syndrome associated to unilateral recurrential paralysis». Anales Otorrinolaringologicos Ibero-americanos. 33 (5): 489–494. PMID 17091862.
- ^ Nagel MA, Cohrs RJ, Mahalingam R, Wellish MC, Forghani B, Schiller A, Safdieh JE, Kamenkovich E, Ostrow LW, Levy M, Greenberg B, Russman AN, Katzan I, Gardner CJ, Häusler M, Nau R, Saraya T, Wada H, Goto H, de Martino M, Ueno M, Brown WD, Terborg C, Gilden DH (March 2008). «The varicella zoster virus vasculopathies: clinical, CSF, imaging, and virologic features». Neurology. 70 (11): 853–860. doi:10.1212/01.wnl.0000304747.38502.e8. PMC 2938740. PMID 18332343.
- ^ «Chickenpox». NHS Choices. UK Department of Health. 19 April 2012. Archived from the original on 24 November 2009.
- ^ «Shingles Vaccine». WebMD. Archived from the original on 29 January 2013.
- ^ «An Overview of Shingles». WebMD. Archived from the original on 8 February 2013.
- ^ «Shingles». PubMed Health.
- ^ Ayoade, Folusakin; Kumar, Sandeep (2020), «Varicella Zoster (Chickenpox)», StatPearls, Treasure Island (FL): StatPearls Publishing, PMID 28846365, retrieved 21 October 2020
- ^ Pincus, Matthew R.; McPherson, Richard A.; Henry, John Bernard (2007). «Ch. 54». Henry’s clinical diagnosis and management by laboratory methods (21st ed.). Saunders Elsevier. ISBN 978-1-4160-0287-1.
- ^ Murray, Patrick R.; Rosenthal, Ken S.; Pfaller, Michael A. (2005). Medical Microbiology (5th ed.). Elsevier Mosby. p. 551. ISBN 978-0-323-03303-9., edition (Elsevier), p.
- ^ Gershon, Anne A. (2007), Arvin, Ann; Campadelli-Fiume, Gabriella; Mocarski, Edward; Moore, Patrick S. (eds.), «Varicella-zoster vaccine», Human Herpesviruses: Biology, Therapy, and Immunoprophylaxis, Cambridge: Cambridge University Press, ISBN 978-0-521-82714-0, PMID 21348127, retrieved 6 February 2021
- ^ Tulchinsky, Theodore H. (2018). «Maurice Hilleman: Creator of Vaccines That Changed the World». Case Studies in Public Health: 443–470. doi:10.1016/B978-0-12-804571-8.00003-2. ISBN 9780128045718. PMC 7150172.
- ^ «Chickenpox (Varicella) | History of Vaccines». www.historyofvaccines.org. Retrieved 6 February 2021.
- ^ «Maurice Ralph Hilleman (1919–2005) | The Embryo Project Encyclopedia». embryo.asu.edu. Retrieved 6 February 2021.
- ^ Chaves SS, Gargiullo P, Zhang JX, Civen R, Guris D, Mascola L, Seward JF (2007). «Loss of vaccine-induced immunity to varicella over time». N Engl J Med. 356 (11): 1121–1129. doi:10.1056/NEJMoa064040. PMID 17360990.
- ^ «Chickenpox (varicella) vaccination». NHS Choices. UK Department of Health. 19 April 2012. Archived from the original on 13 July 2010.
- ^ «Chickenpox vaccine FAQs». 23 January 2019.
- ^ «Live Attenuated Varicella Vaccine: Prevention of Varicella and of Zoster». 30 September 2021.
- ^ «Child, Adolescent & «Catch-up» Immunization Schedules». Immunization Schedules. Centers for Disease Control and Prevention. 11 March 2019. Archived from the original on 5 March 2016.
- ^ Carrillo-Santisteve, P; Lopalco, PL (May 2014). «Varicella vaccination: a laboured take-off». Clinical Microbiology and Infection. 20 Suppl 5: 86–91. doi:10.1111/1469-0691.12580. PMID 24494784.
- ^ «Why aren’t children in the UK vaccinated against chickenpox?». NHS. UK National Health Service. 26 June 2018. Archived from the original on 31 July 2018. Retrieved 11 November 2018.
- ^ Leeuwen, Anne (2015). Davis’s comprehensive handbook of laboratory & diagnostic tests with nursing implications. Philadelphia: F.A. Davis Company. p. 1579. ISBN 978-0803644052.
- ^ CDC (28 April 2021). «Chickenpox Prevention and Treatment». Centers for Disease Control and Prevention. Retrieved 27 April 2022.
- ^ Tebruegge M, Kuruvilla M, Margarson I (2006). «Does the use of calamine or antihistamine provide symptomatic relief from pruritus in children with varicella zoster infection?». Arch. Dis. Child. 91 (12): 1035–1036. doi:10.1136/adc.2006.105114. PMC 2082986. PMID 17119083.
- ^ Domino, Frank J. (2007). The 5-Minute Clinical Consult. Lippincott Williams & Wilkins. p. 248. ISBN 978-0-7817-6334-9.
- ^ Brannon, Heather (21 May 2008). Chicken Pox Treatments Archived 26 August 2009 at the Wayback Machine. About.com.
- ^ Parmet S, Lynm C, Glass RM (February 2004). «JAMA patient page. Chickenpox». JAMA. 291 (7): 906. doi:10.1001/jama.291.7.906. PMID 14970070.
- ^ Naus M; et al. (15 October 2006). «Varizig™ as the Varicella Zoster Immune Globulin for the Prevention of Varicella in At-Risk Patients». Canada Communicable Disease Report. 32 (ACS-8). Archived from the original on 17 January 2013.
- ^ Huff JC (January 1988). «Antiviral treatment in chickenpox and herpes zoster». Journal of the American Academy of Dermatology. 18 (1 Pt 2): 204–206. doi:10.1016/S0190-9622(88)70029-8. PMID 3339143.
- ^ Gnann, John W. Jr. (2007). «Chapter 65Antiviral therapy of varicella-zoster virus infections». In Arvin, Ann; et al. (eds.). Human herpesviruses : biology, therapy, and immunoprophylaxis. Cambridge: Cambridge University Press. ISBN 978-0-521-82714-0. Retrieved 20 January 2014.
- ^ Kay, A. B. (2001). «Allergy and allergic diseases. First of two parts». The New England Journal of Medicine. 344 (1): 30–37. doi:10.1056/NEJM200101043440106. PMID 11136958.
- ^ Kay, A. B. (2001). «Allergy and allergic diseases. Second of two parts». The New England Journal of Medicine. 344 (2): 109–113. doi:10.1056/NEJM200101113440206. PMID 11150362.
- ^ a b «Antiviral medications for chickenpox». Archived from the original on 28 December 2010. Retrieved 27 March 2011.
- ^ «Chickenpox in Children Under 12». Retrieved 6 November 2010.
- ^ «Reye’s Syndrome-Topic Overview». Archived from the original on 5 April 2011. Retrieved 27 March 2011.
- ^ Tunbridge AJ, Breuer J, Jeffery KJ (August 2008). «Chickenpox in adults – clinical management». The Journal of Infection. 57 (2): 95–102. doi:10.1016/j.jinf.2008.03.004. PMID 18555533.
- ^ «What is chickenpox?». Retrieved 6 November 2010.
- ^ Baren JM, Henneman PL, Lewis RJ (August 1996). «Primary Varicella in Adults: Pneumonia, Pregnancy, and Hospital Admissions». Annals of Emergency Medicine. 28 (2): 165–169. doi:10.1016/S0196-0644(96)70057-4. PMID 8759580.
- ^ a b Mohsen AH, McKendrick M (May 2003). «Varicella pneumonia in adults». Eur. Respir. J. 21 (5): 886–891. doi:10.1183/09031936.03.00103202. PMID 12765439.
- ^ Anderson, D.R.; Schwartz, J.; Hunter, N.J.; Cottrill, C.; Bissaccia, E.; Klainer, A.S. (1994). «Varicella Hepatitis: A Fatal Case in a Previously Healthy, Immunocompetent Adult». Archives of Internal Medicine. 154 (18): 2101–2106. doi:10.1001/archinte.1994.00420180111013. PMID 8092915.
- ^ Abro AH, Ustadi AM, Das K, Abdou AM, Hussaini HS, Chandra FS (December 2009). «Chickenpox: presentation and complications in adults». Journal of Pakistan Medical Association. 59 (12): 828–831. PMID 20201174. Archived from the original on 20 May 2014. Retrieved 17 April 2013.
- ^ «Definition of Chickenpox». MedicineNet.com. Archived from the original on 28 July 2006. Retrieved 18 August 2006.
- ^ «Is Necrotizing Fasciitis a complication of Chickenpox of Cutaneous Vasculitis?». atmedstu.com. Archived from the original on 15 April 2008. Retrieved 18 January 2008.
- ^ Strangfeld A, Listing J, Herzer P, Liebhaber A, Rockwitz K, Richter C, Zink A (February 2009). «Risk of herpes zoster in patients with rheumatoid arthritis treated with anti-TNF-alpha agents». JAMA. 301 (7): 737–744. doi:10.1001/jama.2009.146. PMID 19224750.
- ^ Weller TH (1997). «Varicella-herpes zoster virus». In Evans AS, Kaslow RA (eds.). Viral Infections of Humans: Epidemiology and Control. Plenum Press. pp. 865–892. ISBN 978-0-306-44855-3.
- ^ a b Chicken Pox Complications Archived 28 April 2008 at the Wayback Machine
- ^ CDC (11 August 2021). «Chickenpox for HCPs». Centers for Disease Control and Prevention. Retrieved 29 March 2022.
- ^ Di Pietrantonj, Carlo; Rivetti, Alessandro; Marchione, Pasquale; Debalini, Maria Grazia; Demicheli, Vittorio (22 November 2021). «Vaccines for measles, mumps, rubella, and varicella in children». The Cochrane Database of Systematic Reviews. 2021 (11): CD004407. doi:10.1002/14651858.CD004407.pub5. ISSN 1469-493X. PMC 8607336. PMID 34806766.
- ^ «Georgia ranks 10th for social media admissions of chickenpox». Archived from the original on 21 June 2013. Retrieved 13 June 2013.
- ^ «Chickenpox in the USA». Archived from the original on 26 July 2013. Retrieved 12 June 2013.
- ^ Wharton M (1996). «The epidemiology of varicella-zoster virus infections». Infect Dis Clin North Am. 10 (3): 571–581. doi:10.1016/S0891-5520(05)70313-5. PMID 8856352.
- ^ «Epidemiology of Varicella Zoster Virus Infection, Epidemiology of VZV Infection, Epidemiology of Chicken Pox, Epidemiology of Shingles». Archived from the original on 13 June 2008. Retrieved 22 April 2008.
- ^ a b Belshe, Robert B. (1984). Textbook of human virology (2nd ed.). Littleton, MA: PSG. p. 829. ISBN 978-0-88416-458-6.
- ^ a b Teri Shors (2011). «Herpesviruses: Varicella Zoster Virus (VZV)». Understanding Viruses (2nd ed.). Jones & Bartlett. p. 459. ISBN 978-0-7637-8553-6.
- ^ Pattison, John; Zuckerman, Arie J.; Banatvala, J.E. (1994). Principles and practice of clinical virology (3rd ed.). Wiley. p. 37. ISBN 978-0-471-93106-5.
- ^ Chicken-pox is recorded in Oxford English Dictionary 2nd ed. since 1684; the OED records several suggested etymologies
- ^ Johnson, Samuel (1839). Dictionary of the English language. London: Williamson. p. 195.
- ^ a b Charles, M.D., Shamard (22 March 2019). «Doctors say Kentucky Gov. Matt Bevin is wrong about ‘chickenpox on purpose’«. NBC News. Retrieved 22 March 2019.
Chickenpox parties were once a popular way for parents to expose their children to the virus so they would get sick, recover and build up immunity to the disease. … Most doctors believe that deliberately infecting a child with the full-blown virus is a bad idea. While chickenpox is mild for most children, it can be a dangerous virus for others – and there’s no way to know which child will have a serious case, experts say.
- ^ «Chicken Pox parties do more harm than good, says doctor». KSLA News 12 Shreveport, Louisiana News Weather & Sports. Archived from the original on 27 January 2012. Retrieved 17 December 2011.
- ^ Committee to Review Adverse Effects of Vaccines; Institute of, Medicine; Stratton, K.; Ford, A.; Rusch, E.; Clayton, E. W. (2011). Adverse Effects of Vaccines: Evidence and Causality. doi:10.17226/13164. ISBN 978-0-309-21435-3. PMID 24624471. S2CID 67935593.
- ^ Ogunjimi, B; Van Damme, P; Beutels, P (2013). «Herpes Zoster Risk Reduction through Exposure to Chickenpox Patients: A Systematic Multidisciplinary Review». PLOS ONE. 8 (6): e66485. Bibcode:2013PLoSO…866485O. doi:10.1371/journal.pone.0066485. PMC 3689818. PMID 23805224.
- ^ Cohen JI, Moskal T, Shapiro M, Purcell RH (December 1996). «Varicella in Chimpanzees». Journal of Medical Virology. 50 (4): 289–292. doi:10.1002/(SICI)1096-9071(199612)50:4<289::AID-JMV2>3.0.CO;2-4. PMID 8950684. S2CID 28842789.
- ^ Myers MG, Kramer LW, Stanberry LR (December 1987). «Varicella in a gorilla». Journal of Medical Virology. 23 (4): 317–322. doi:10.1002/jmv.1890230403. PMID 2826674. S2CID 84875752.
- ^ «Chickenpox Treatment & Management: Approach Considerations, Treatment in Healthy Children, Treatment in Immunocompetent Adults». Medscape emedicine. 3 June 2022.
- ^ Klassen, TP; Hartling, L. (2005). «Acyclovir for treating varicella in otherwise healthy children and adolescents». Cochrane Database of Systematic Reviews. 2011 (4): CD002980. doi:10.1002/14651858.CD002980.pub3. PMC 8407192. PMID 16235308. S2CID 11018303.
External links[edit]
![]()
Wikimedia Commons has media related to Chickenpox.
- Chickenpox at Curlie
- Prevention of Varicella: Recommendations of the Advisory Committee on Immunization Practices (ACIP), 1996
- Antiviral therapy of varicella-zoster virus infections, 2007
- Epidemiology and Prevention of Vaccine-Preventable Diseases: Varicella, US CDC’s «Pink Book»
- Chickenpox at MedlinePlus
Ветряная оспа — детская инфекция, которая вызывает повышение температуры и пузырьковые высыпания по всему телу.
Поражает главным образом непривитых детей от 2 до 10 лет. Пол, генетика, образ жизни значения не имеют.
Вирус передается воздушно-капельным путем через кашель и чихание инфицированных людей, а также при непосредственном контакте с волдырями. Если у человека нет иммунитета к этой инфекции, он может заразиться и заболеть либо ветряной оспой либо опоясывающим герпесом.
Симптомы
У детей болезнь обычно протекает легко, но симптомы ее могут быть более тяжелыми у грудных детей, подростков и взрослых. Очень тяжело ветряная оспа протекает у людей с пониженным иммунитетом, таких, как больные СПИДом.
Симптомы болезни появляются через 1–3 недели после заражения. У детей болезнь часто начинается с небольшого повышения температуры или головной боли; у взрослых ее начальные проявления могут быть похожи на грипп. По мере прогрессирования инфекции начинают появляться следующие симптомы:
- Сыпь в виде россыпи мелких красных пятнышек, которые сразу начинают зудеть и превращаются в наполненные жидкостью пузырьки. В течение 24 часов пузырьки лопаются, на их поверхности образуются корочки. Новые пузырьки продолжают появляться в течение 1–6 дней. Высыпания могут или распространяться по всему телу, или поражать лишь некоторые участки кожи головы и тела.
- В некоторых случаях самый большой дискомфорт во время приема пищи вызывают волдыри в полости рта, которые затем превращаются в язвы.
Самым распространенным осложнением ветряной оспы является бактериальная инфекция расчесанных пузырьков. Другие возможные осложнения — пневмония, которая чаще бывает у взрослых и (крайне редко) — воспаление головного мозга. Развитие осложнений наиболее вероятно у новорожденных и у людей, иммунитет которых ослаблен в силу различных причин.
Диагностика
Ветряную оспу обычно диагностируют по виду сыпи.
Лечение
Детям с легкой формой инфекции нужен покой и меры по снижению температуры. Для уменьшения зуда можно применять жидкость от солнечных ожогов. Для профилактики бактериальной инфекции больному следует обрезать ногти и стараться не расчесывать пузырьки. К пациентам из группы риска — грудничкам, подросткам и больным со сниженным иммунитетом — необходимо немедленно вызвать врача при первых симптомах ветряной оспы. Для уменьшения развития инфекции можно принимать противовирусные препараты, но они эффективны только на ранних стадиях болезни.
Дети обычно выздоравливают в течение 10–14 дней с момента появления сыпи, но у них могут остаться шрамики на местах расчесанных пузырьков, инфицированных бактериями. У людей, переболевших ветряной оспой, иммунитет к этой болезни остается на всю жизнь.
Общие сведения
Ветрянка (или ветряная оспа) — это заболевание инфекционной природы, которое вызывается вирусом герпеса и проявляется в виде пузырьковой сыпи. Распространение ветрянки происходит воздушно-капельным путем, а также вследствие прямых контактов с выделениями из дыхательной системы зараженного человека и жидкостью, которая содержится в кожных высыпаниях больных людей.
Иногда ветряная оспа может передаваться и через зараженные бытовые предметы, одежду. Те, кто уже переболел ветрянкой, получают стойкий иммунитет к этой болезни, случаи повторного заболевания ветряной оспой крайне редки. Однако вирус какое-то время еще находится в организме, и способен вызывать опоясывающий лишай, почти в 15% случаев.
Обычно ветрянкой болеют практически все дети в возраст от 7 до 14 лет, однако в последнее время это заболевание поражает взрослых людей, и протекает в тяжелых формах. Малыши в возрасте до 6-ти месяцев болеют очень редко, т.к. обычно имеют антитела переболевшей ветрянкой матери. Если ветрянкой заболела женщина на ранних сроках беременности, то в большинстве случаев развивается порок плода, а если на последних месяцах — то это приводит к заболеванию плода. Нужно заметить, что восприимчивость к заболеванию очень высокая.
Как правило, инкубационный период заболевания длится от 10 до 20 дней, и на начальном этапе симптомы отсутствуют. Ветрянка проявляется сыпью на лице, а потом и на всем теле, включая слизистые, примерно на 10-14 день после первого контакта с зараженным человеком, а также резким повышением температуры тела до 38, и даже 39 градусов. Врачи сравнивают сыпь, образующуюся при ветрянке, с каплями воды, пролитой на раскаленную сковороду. Чаще всего такая сыпь держится от одной до двух недель, после чего пузырьки лопаются, образуются желтоватые корочки, постепенно отпадают, не оставляя на коже шрамов, однако может появиться пигментация.
В большинстве случаев заболевание протекает достаточно легко. В сложных случаях, у новорожденных, особенно при наличии сопутствующих заболеваний, вирус может поражать печень и почки, легкие, и даже костный мозг, могут наблюдаться судороги, поражения нервной системы, вплоть до летального исхода.
Источником болезни является человек, болеющий ветрянкой. Он опасен для окружающих с начала заболевания и еще несколько дней после образования последних пузырьков. Обычно подхватить ветряную оспу можно через воздушно-капельный путь, во время кашля или чихания больного человека, от прикосновений к жидкости из ветряного пузырька, сам вирус живуч, и может проникать по вентиляционным системам в соседние квартиры.
Симптомы ветряной оспы
 Первым симптомом ветряной оспы является сыпь, при одновременном повышении температуры до 37,5-39 градусов. Одновременно больного беспокоит головная боль, слабость, иногда — боль в горле и рвота, т.е. симптомы интоксикации.
Первым симптомом ветряной оспы является сыпь, при одновременном повышении температуры до 37,5-39 градусов. Одновременно больного беспокоит головная боль, слабость, иногда — боль в горле и рвота, т.е. симптомы интоксикации.
Сыпь появляется примерно через 7-14 дней после контакта с больным ветряной оспой. Изначально симптомом ветрянки является появление округлых розовых пятнышек, которые постепенно начинают возвышаться над кожей, образовывая пузырьки с прозрачной жидкостью (их диаметр — от 1 до 5 мм). Вокруг пузырьков, напоминающих капли воды, образуются розово-красные ободки. В самой жидкости содержаться живые вирусы. Постепенно они лопаются, покрываются желтыми корочками, примерно через две недели, и отпадают. Располагаются высыпания на лице и коже головы, и быстро распространяются по телу и слизистым рта, половых органах.
Новые пузырьки появляются постоянно, они располагаются между старыми, и поэтому сыпь выглядит неоднородно. Одновременно есть покраснения, пузырьки и корочки. И каждая новая волна высыпаний сопровождается увеличением температуры тела. Обычно больного беспокоит зуд, а особенные неудобства доставляют высыпания на слизистых. Поэтому лечение ветряной оспы больше симптоматическое. Многие дети, и особенно маленькие, расчесывают пузырьки и сдирают корочки. Помните, что от этого могут образовываться гнойнички, а впоследствии – и рубцы на коже. Однако при неосложненном течении ветрянки рубцы не остаются, возможна лишь временная пигментация.
Диагностика ветряной оспы
Это заболевание диагностировать очень просто. Для постановления диагноза «ветрянка» необходимо обнаружить типичные элементы сыпи. Остальные методы исследования, например анализы крови, мочи, дополнительной информации не дадут. Если обнаружены симптомы ветряной оспы у беременной женщины, а также у взрослых страдающим хроническими заболеваниями, следует сразу же обратиться к врачу.
Лечение ветряной оспы
 Обычно лечение ветряной оспы происходит в домашних условиях, желателен постельный режим, питье как можно большего количества жидкости и надлежащий гигиенический уход. Постельное белье должно быть чистым. Для ускорения подсыхания пузырьков, их нужно смазывать 1% раствором зеленки (бриллиантового зеленого), 10% раствором марганцовки (перманганата калия) или раствором метиленового синего. Эти вещества подсушивают высыпания и дезинфицируют ранки.
Обычно лечение ветряной оспы происходит в домашних условиях, желателен постельный режим, питье как можно большего количества жидкости и надлежащий гигиенический уход. Постельное белье должно быть чистым. Для ускорения подсыхания пузырьков, их нужно смазывать 1% раствором зеленки (бриллиантового зеленого), 10% раствором марганцовки (перманганата калия) или раствором метиленового синего. Эти вещества подсушивают высыпания и дезинфицируют ранки.
Для уменьшения зуда могут назначаться противоаллергические препараты, такие как Диазолин и Тавегил. Одновременно можно обрабатывать кожу водой с добавлением уксуса и припудриванием тальком. После того, как пузырьки подсохнут, полезными будут теплые ванны. Если больного беспокоят симптомы интоксикации, то для предотвращения развития тяжелых форм ветрянки может назначаться ацикловир.
Для избежания расчесывания пузырьков и занесения в них инфекции, вовремя состригайте ногти и держите руки в чистоте.
При осложненных формах течения болезни, в качестве лечения ветрянки, а также беременным женщинам на поздних сроках могут вводить иммуноглобулин, который способствует выделению антител к ветрянке.
Доктора
Лекарства
Осложнения ветрянки
Осложнения ветрянки наблюдаются при тяжелых вариантах ее течения. У детей старшего возраста может развиться острая мозжечковая атаксия, вызывающая проблемы с мышечной координацией, у взрослых симптомы ветряной оспы дополнятся проявлениями ветряная пневмония. Иногда могут развиваться поражения почек, суставов, сердца и легких. Бактериальные осложнения возникают из-за инфицирования пузырьков во время расчесывания, и чаще всего встречаются у ослабленных детей.
Считается, что гораздо лучше переболеть ветрянкой в детстве, чем во взрослом возрасте, поэтому прививка против ветрянки не является обязательной для вакцинации детей.
Диета, питание при ветряной оспе

Диета при ветрянке
- Эффективность: лечебный эффект через 5-7 суток
- Сроки: не более 14 дней
- Стоимость продуктов: 1500-1600 рублей в неделю
Список источников
- Андерсон, Т. Инфекционные болезни человека. Динамика и контроль: пер. с англ. / Т. Андерсон, Р. Мэй, под ред. ГИ. Марчука. — М.: Мир, Научный мир, 2004.
- Юнусова Х.А. Ветряная оспа / Х.А. Юнусова, Ф.С. Шамсиев. — М.: Вузовская книга, 1999.
- Кускова Т. К., Белова Е. Г., Мигманов Т. Э. Ветряная оспа // Лечащий врач. — 2004. — № 1.
- Учайкин В. ф. Руководство по инфекционным болезням у детей. — М.: ГЭОТАР Медицина, 2004.
Медицинский эксперт статьи
Новые публикации
Ветрянка (ветряная оспа)
, медицинский редактор
Последняя редакция: 17.10.2021

х
Весь контент iLive проверяется медицинскими экспертами, чтобы обеспечить максимально возможную точность и соответствие фактам.
У нас есть строгие правила по выбору источников информации и мы ссылаемся только на авторитетные сайты, академические исследовательские институты и, по возможности, доказанные медицинские исследования. Обратите внимание, что цифры в скобках ([1], [2] и т. д.) являются интерактивными ссылками на такие исследования.
Если вы считаете, что какой-либо из наших материалов является неточным, устаревшим или иным образом сомнительным, выберите его и нажмите Ctrl + Enter.
- Код по МКБ-10
- Эпидемиология
- Причины
- Возбудители
- Патогенез
- Симптомы
- Формы
- Осложнения и последствия
- Диагностика
- Что нужно обследовать?
- Как обследовать?
- Какие анализы необходимы?
- Дифференциальная диагностика
- Лечение
- К кому обратиться?
- Дополнительно о лечении
- Профилактика
Ветрянка (ветряная оспа) является острым системным заболеванием, обычно у детей, вызываемым вирусом варицелла зостер (герпесвирус человека 3-го типа). Заболевание обычно начинается с умеренных общих симптомов, за которыми быстро появляются высыпания на коже, быстро распространяющиеся и проявляющиеся пятном, папулой, везикулой и корочкой. Диагноз клинический. Лица с риском осложнений получают постэкспозиционную профилактику иммуноглобулином и, если заболевание развивается, лечатся противовирусными препаратами (валацикловир, фамцикловир, ацикловир). Вакцинация эффективна.
 [1], [2], [3]
[1], [2], [3]
Код по МКБ-10
B01 Ветряная оспа [varicella]
Эпидемиология
Источник вируса — больной от последнего дня инкубационного периода до 5-го дня после появления последних высыпаний. Основной путь передачи — воздушно-капельный. Вирус способен распространяться на расстояния до 20 м (через коридоры в соседние комнаты квартиры и даже с одного этажа на другой). Возможен вертикальный механизм передачи вируса через плаценту. Восприимчивость к ветряной оспе очень высокая (минимум 90%), за исключением детей первых 3 мес жизни, у которых сохраняется пассивный иммунитет.
Заболеваемость характеризуется выраженной сезонностью, достигая максимума в осенне-зимние месяцы. Болеют преимущественно дети. Постинфекционный иммунитет напряжённый, поддерживается персистенцией вируса в организме. При снижении его напряжённости возникает опоясывающий герпес.
[4], [5], [6], [7], [8], [9], [10], [11], [12]
Причины ветрянки
Причина ветряной оспы — вирус ветрянки Varicella zoster virus семейства Herpesviridae. Размер вируса от 150 до 200 нм, он находится в ветряночных пузырьках в первые 3-4 дня болезни; после 7-го дня обнаружить вирус не удаётся. Геном имеет двуспиральную линейную молекулу ДНК, липидную оболочку. Вирус репродуцируется только в ядре инфицированных клеток человека. Установлена идентичность вируса, вызывающего опоясывающий герпес, и вируса ветряной оспы. В окружающей среде вирус неустойчив и быстро погибает, в капельках слизи, слюны вирус сохраняется не более 10-15 мин. Нагревание, солнечные лучи, УФ-излучение быстро инактивируют его.
Ветрянка очень контагиозна и распространяется воздушно-капельным путем, особенно во время продрома и во время раннего периода высыпаний. Заразный период определяется от 48 часов с момента первых высыпаний до появления корочек. Прямая передача (от носителей) невозможна.
Эпидемические вспышки возможны зимой и ранней весной и имеют 3-4 цикла. У новорожденных может быть иммунитет, вероятно, трансплацентарный, до 6 месяцев.
[13], [14], [15], [16], [17], [18]
Возбудители
Патогенез
Входные ворота вируса ветрянки — слизистые оболочки верхних дыхательных путей, где происходит репликация вируса, далее по лимфатическим путям возбудитель проникает в кровь. В конце инкубационного периода развивается виремия. Вирус фиксируется в клетках эктодермального происхождения, преимущественно в эпителиальных клетках кожи и слизистых оболочек дыхательных путей, ротоглотки. Возможно поражение межпозвоночных ганглиев, коры мозжечка и больших полушарий, подкорковых ганглиев. В редких случаях при генерализованной форме поражается печень, лёгкие, ЖКТ. В коже вирус вызывает формирование пузырьков, заполненных серозным содержимым, в котором вирус находится в высокой концентрации. При тяжёлых генерализованных формах болезни везикулы и поверхностные эрозии обнаруживают на слизистых оболочках ЖКТ, трахеи, мочевого пузыря и почечных лоханок, уретры, конъюнктивь: глаз. В печени, почках, лёгких и ЦНС выявляют мелкие очаги некроза с кровоизлияниями по периферии.
В патогенезе значительную роль отводят клеточному иммунитету, в основном системе Т-лимфоцитов, при угнетении которой наблюдают более тяжёлое течение болезни. После стихания острых проявлений первичной инфекции вирус пожизненно персистирует в спинальных нервных ганглиях.
[19], [20], [21], [22], [23], [24], [25], [26], [27], [28], [29]
Симптомы ветрянки
Инкубационный период ветряной оспы длится от 10 до 21 дня, при введении нормального иммуноглобулина человека может удлиняться до 28 дней.
Продромальные симптомы ветрянки чаще отсутствуют, редко отмечают кратковременный субфебрилитет на фоне ухудшения общего самочувствия. Везикулы появляются обычно одновременно с повышением температуры или на несколько часов позднее. При обильной экзантеме температура может повышаться до 39 С и выше. Высыпания появляются волнами на протяжении 2-4 дней и сопровождаются подъёмом температуры. Сыпь локализована на лице, волосистой части головы, туловище и конечностях.
На ладонях и подошвах она встречается только при обильных высыпаниях. Элементы сыпи вначале имеют вид мелких макуло-папул, которые в течение нескольких часов превращаются в везикулы круглой или овальной формы, и размер 2-5 мм. Они располагаются поверхностно и на неинфильтрированном основании, стенка их напряжена, блестяща, содержимое прозрачно, но в некоторых везикулах мутнеет. Большинство везикул окружено узкой каймой гиперемии. Везикулы подсыхают через 2-3 дня. на их месте образуются корочки, которые отпадают через 2-3 нед. После отпадения корочек рубцов, как правило, не остаётся. Высыпания наблюдаются и на конъюнктиве, слизистых оболочках ротоглотки, иногда гортани, половых органов. Пузырьки на слизистых быстро превращаются в эрозии с желтовато-серым дном, которые через несколько дней эпителизируются. Высыпания на слизистой оболочке гортани и трахеи, сопровождаемые отёком слизистой оболочки, могут вызывать грубый кашель, охриплость голоса, в редких случаях явления крупа. Высыпания на слизистой оболочке половых губ представляют угрозу развития вульвовагинита. Высыпания часто сопровождаются увеличением лимфатических узлов.
К концу первой недели болезни одновременно с подсыханием везикул нормализуется температура, улучшается самочувствие больного. В это время многих больных беспокоит кожный зуд.
В гемограмме в период высыпания наблюдают небольшую лейкопению и относительный лимфоцитоз. СОЭ обычно не увеличена.
У иммунокомпетентных детей ветряная оспа редко протекает тяжело. У взрослых и иммуноскомпрометированных детей инфекция может иметь тяжелое течение. Умеренная головная боль, невысокая температура и недомогание могут быть выраженны 11-15 дней после заражения и длятся около 24-36 часов с момента появления высыпаний. Эти проблемы наиболее вероятны у пациентов в возрасте старше 10 лет и особенно тяжело протекают у взрослых.
[30], [31]
Формы
Различают следующие клинические формы ветряной оспы:
По течению:
- типичные;
- атипичные:
- рудиментарная;
- геморрагическая;
- гангренозная;
- генерализованная.
По тяжести:
- лёгкие;
- среднетяжёлые;
- тяжёлые:
- с выраженной общей интоксикацией;
- с выраженными изменениями на коже.
Выделяется типичная и атипичная ветрянка (ветряная оспа). К типичной относят случаи с характерной сыпью. Чаще всего типичная ветрянка протекает в лёгкой и среднетяжёлой форме. Тяжёлая форма болезни возникает редко, чаще у ослабленных детей и взрослых, для неё характерна длительная ремиттирующая лихорадка до 6-8 сут. Отмечают такие симптомы ветрянки, как: головную боль, возможна рвота, менингеальный синдром, нарушение сознания, артериальная гипотензия, судороги. Сыпь обильная, крупная, метаморфоз её замедлен, возможны элементы с пупковидным вдавлением в центре, напоминающие элементы сыпи при натуральной оспе.
К атипичным формам относят рудиментарную, буллёзную, геморрагическую, гангренозную и генерализованную ветряные оспы.
Рудиментарную форму чаще наблюдают у детей, получавших иммуноглобулины, плазму в период инкубации. Сыпь необильная, розеолёзно-папулёзная с единичными очень мелкими везикулами. Общее состояние не нарушается.
Геморрагическая форма ветрянки встречается очень редко у резко ослабленных больных, страдающих гемабластозом или геморрагическими диатезами, на фоне приёма глюкокортикоидов и цитостатиков. На 2-3-й день высыпания содержимое пузырьков приобретает геморрагический характер. Появляются кровоизлияния в кожу и слизистые оболочки, носовые кровотечения и другие проявления геморрагического синдрома. Возможен летальный исход.
Очень редко встречается гангренозная форма ветряной оспы. Она развивается у истощённых больных, при плохом уходе, создающем возможность возникновения вторичной инфекции. Вначале отдельные пузырьки принимают геморрагический характер, затем в окружении их возникает значительная воспалительная реакция. В последующем образуется геморрагический струп, после отпадения которого обнажаются глубокие язвы с грязным дном и крутыми или подрытыми краями. Язвы, вследствие прогрессирующего гангренозного распада ткани, увеличиваются, сливаются, принимая значительные размеры. Нередко возникают осложнения гнойно-септического характера. Общее состояние больного тяжёлое, течение болезни длительное.
Генерализованная (висцеральная) форма. Встречается главным образом у новорождённых, иногда у взрослых с иммунодефицитом. Характерна гипертермия, интоксикация, поражение внутренних органов. Летальность высокая. На вскрытии обнаруживают мелкие очаги некроза в печени, лёгких, поджелудочной железе, надпочечниках, тимусе, селезёнке, костном мозге.
Ветрянка представляет опасность для плода и новорождённого. Если заболевание у женщины возникло в конце беременности, возможны преждевременные роды и мертворождения. При заболевании ветряной оспой в ранние сроки беременности может произойти внутриутробное заражение плода с развитием у него различных пороков развития. Вероятность заболевания новорождённых составляет 17%, их гибели — 30%. Врождённая Ветрянка (ветряная оспа) протекает тяжело. сопровождаясь тяжёлыми висцеральными поражениями.
[32], [33], [34]
Осложнения и последствия
Может присоединяться вторичная бактериальная инфекция (стрептококки и стафилококки), вызывает целлюлит и редко стрептококковый токсический шок. Самое частое осложнение ветрянки (ветряной оспы) — бактериальная суперинфекция, вызванная Streptococcus pyogenes и Staphylococcus aureus. При этом содержимое везикул нагнаивается, формируя пустулы. Возможно развитие импетиго или буллёзной пиодермии.
Пневмония может осложнять тяжелую ветряную оспу у взрослых, новорожденных и иммуноскомпрометированных лиц любого возраста, но не у маленьких детей с достаточной иммунокомпетентностью. Описаны случаи «ветряночной» (вирусной) пневмонии, которая развивается в первые 3-4 дня болезни. Больные жалуются на одышку, боль в грудной клетке при дыхании, кашель с кровянистой мокротой, высокую температуру. Объективно отмечают цианоз кожного покрова, признаки бронхита, бронхиолита, а в некоторых случаях может развиться отёк лёгких. Патологическая картина в лёгких может напоминать милиарный туберкулёз (так как в лёгких выявляют множественные милиарные узелки). Из специфических осложнений наиболее серьёзными считают поражения нервной системы различной локализации — энцефалиты, менингоэнцефалиты, оптикомиелиты и миелиты, полирадикулоневриты, серозные менингиты. Наиболее характерен ветряночный энцефалит, на долю которого приходится около 90% неврологических осложнений.
Могут встречаться миокардиты, транзиторные артриты и гепатиты, геморрагические осложнения.
Энцефалопатия встречается менее чем в 1 случае на 1000 больных, обычно при разрешении болезни или в течение первых двух недель. Чаще всего эти симптомы ветрянки (ветряной оспы) разрешаются, хотя редко могут продолжаться длительно или привести к смерти. Одним из наиболее частых неврологических осложнений является острая постинфекционная мозжечковая атаксия. Поперечный миелит, паралич черепных нервов, проявления, подобные множественному склерозу, также могут иметь место. Редким, но очень тяжелым осложением у детей может быть синдром Рея, который начинается на 3-8-й день после начала сыпи, прием аспирина увеличивает риск. У взрослых в 1-2 случаях на 1000 больных встречается энцефалит, который может угрожать жизни.
Частота развития энцефалита не зависит от тяжести течения болезни. Чаще всего осложнения возникают на 5-8-й дни болезни. Описаны случаи развития энцефалита во время высыпания и даже до появления сыпи. Отмечено, что чем раньше начинается энцефалит, тем тяжелее он протекает. Энцефалит манифестирует остро с нарушения сознания, судорогами лишь у 15-20% больных. В остальных случаях доминирует очаговая симптоматика, которая нарастает в течение нескольких дней. Наиболее характерны мозжечковые и вестибулярные нарушения. Отмечают атаксию, тремор головы, нистагм, скандированную речь, интенционный тремор, дискоординацию. Возможны пирамидные знаки, гемипарезы, парезы черепных нервов. Редко наблюдают спинальную симптоматику. в частности, тазовые расстройства. Менингеальный синдром выражен слабо или отсутствует. У части больных в спинно-мозговой жидкости обнаруживают лимфоцитарный плеоцитоз, увеличение количества белка и глюкозы. Течение болезни доброкачественное так как нейроциты страдают редко, лишь при развитии энцефалита в ранние сроки. Неблагоприятные отдалённые последствия редки.
[35], [36], [37], [38], [39], [40]
Диагностика ветрянки
Диагностика ветряной оспы в обычных случаях не представляет затруднений. Диагноз устанавливают, главным образом, на основании клинических данных, при этом учитывают эпидемиологический анамнез. Ветряная оспа (ветрянка) должна быть заподозрена у пациентов с характерной сыпью. Следует помнить, что подобная сыпь встречается у других больных, с вирусными поражениями кожи.
При необходимости и в диагностически неясных случаях используют вирусоскопический, вирусологический, серологический и молекулярно-биологический методы. Вирусоскопическая диагностика ветрянки заключается в окрашивании содержимого пузырька серебрением (по М.А. Морозову) для выявления вируса с помощью обычного светового микроскопа. Вирусологический метод практически не используют. Из серологических методов применяют РСК, РИМФ, ИФА. Основной метод лабораторной диагностики — молекулярно-биологический метод (ПЦР).
[41], [42], [43], [44], [45], [46]
Что нужно обследовать?
Как обследовать?
Какие анализы необходимы?
Дифференциальная диагностика
Дифференциальная диагностика ветрянки проводится с герпетической сыпью при простом герпесе, опоясывающим герпесом, везикулёзным риккетсиозом, импетиго и натуральной оспой. Необходимо исключать герпетическую экзему Капоши, а также инфекции, вызванные вирусами Коксаки и ECHO.
Начало с кратковременного недомогания, слабости, субфебрильной температуры тела, першения в горле в течение 2 дней
ЕСТЬ
Исследование продолжается
Появление сыпи на I-3-й день болезни на лице, волосистой части головы с распространением на туловище и конечности, слизистые оболочки. Одновременное ухудшение самочувствия, повышение температуры тела, появление симптомов интоксикации (головной боли, слабости, рвоты)
ЕСТЬ
Исследование продолжается
Полиморфный характер сыпи. На одном участке кожи можно увидеть пятно, папулы, везикулы, пустулы, корочки (ложный полиморфизм сыпи)
ЕСТЬ
Исследование продолжается
В анамнезе контакт с больным ветряной оспой за 2 недели до болезни
ЕСТЬ
Ставится клинический диагноз: «Ветряная оспа, среднетяжёлое течение»
Показания к консультации других специалистов
При развитии осложнений, связанных с поражением нервной системы, показана консультация невролога (энцефалиты, менингоэнцефалиты, оптикомиелиты и миелиты, полирадикулоневриты, серозные менингиты).
Консультация хирурга при глубоком поражении кожи и подкожной клетчатки.
К кому обратиться?
Лечение ветрянки
Госпитализируют больных при тяжёлом, осложнённом течении болезни и по эпидемиологическим показаниям.
Ветрянка у детей редко бывает тяжелой. Тяжелая или фатальная болезнь чаще бывает у взрослых больных с депрессией Т-клеточного иммунитета (например, лимфоретикулярная опухоль), у получающих глюкокортикоиды или химиотерапию.
Ветрянка (ветряная оспа) в среднетяжелых случаях требует только симптоматического лечения. Мероприятия, направленные на снижение зуда и предотвращение срыва корок, которые предрасполагают к вторичной инфекции, иногда трудновыполнимы. Могут быть полезны марлевые компрессы или, при сильном зуде, системные антигистаминные препараты, слизистые овсяные ванны. Одномоментное введение больших доз системных антигистаминных препаратов может вызвать энцефалопатию и недопустимо.
Для предотвращения вторичной бактериальной инфекции больные должны регулярно принимать ванну, содержать в чистоте белье и руки, иметь коротко подстриженные ногти. Антисептики не используются, если нет инфицирования; инфекция лечится антибиотиками.
Антивирусные препараты, назначаемые внутрь больным с сохраненным иммунитетом в течение 24 часов от начала сыпи, позволяет снизить длительность и тяжесть симптомов. Однако поскольку чаще болеют дети, антивирусное лечение ветрянки не является рутинным. Прием внутрь валацикловира, фамцикловира, ацикловира рекомендуется иммуноскомпрометированным больным, здоровым лицам с риском тяжелой болезни, включая всех пациентов старше 12 лет с кожными заболеваниями (особенно экзема) или хроническими болезнями легких, а также получающих салицилаты или глюкокортикоиды. Фамцикловир применяют по 500 мг 3 раза в день, валацикловир 1 г 3 раза. Ацикловир менее желателен в применении, поскольку биодоступность его при приеме внутрь ниже, но он может даваться в дозе 20 мг/кг 4 раза в день до максимальной дозы 3200 мг. Иммуноскомпрометированные дети старше 1 года должны получать 500 мг/м2 каждые 8 часов. Пациенты не должны ходить в школу и на работу, пока есть корочки.
При развитии ветряночной пневмонии показаны ингаляции интерферона лейкоцитарного человеческого (лейкинферон).
Местное лечение ветряной оспы заключается в использовании 5-10% раствора калия перманганата или 1% спиртового раствора бриллиантового зелёного с целью предотвращения присоединения вторичной инфекции и более быстрого подсыхания пузырьков. Для уменьшения зуда кожу смазывают глицеролом или обтирают водой с уксусом или спиртом. Назначают антигистаминные препараты (клемастин, дифенгидрамин, цетиризин, акривастин). При геморрагических формах показаны викасол, рутин, кальция хлорид.
Физиотерапевтическое лечение ветрянки заключается в использовании УФ-облучения в течении 2-3 дней для ускорения отпадения корочек.
Диспансерное наблюдение в течение месяца.
Примерные сроки нетрудоспособности — 10 дней.
Следует ограничивать физическую нагрузку, избегать переохлаждений, питаться сбалансированно.
Дополнительно о лечении
Профилактика
Перенесенная ветрянка обеспечивает пожизненный иммунитет. Все здоровые дети и неболевшие взрослые должны быть иммунизированы живой аттенуированной вакциной. Вакцинация особенно важна у женщин в детородном возрасте и взрослых, имеющих хронические заболевания. Серологические исследования для определения иммунного статуса перед вакцинацией обычно не требуются. Вакцинация противопоказана больным с тяжелыми заболеваниями или заболеваниями средней тяжести, иммуноскомпрометированных пациентов, беременных женщин, принимающих большие дозы глюкокортикоидов, у детей, принимающих салицилаты. Хотя вакцина может вызывать симптомы ветряной оспы у здоровых пациентов, болезнь обычно легкая (меньше 10 папул или везикул) и непродолжительная.
После контакта ветряная оспа (ветрянка) может быть предотвращена или ослаблена внутримышечным введением иммуноглобулина, приготовленного из пула плазмы с высокими титрами специфических антител. Такая профилактика должна быть проведена у больных с лейкемией, иммунодефицитами и ослабленных пациентов; непривитых беременных; новорожденных, у чьих матерей была ветряная оспа за 5 дней до и в течение 2 дней после родов. Иммуноглобулин дается внутримышечно в течение 4 дней после контакта в дозе от 12,5 ЕД/кг (100 ЕД/мл), но не более 625 ЕД. Постконтактная вакцинация может ослабить или предотвратить болезнь, если применяется в течение 3 дней и возможна до 5 дней после контакта. Люди, не имеющие иммунитета против ветряной оспы, должны избегать контактов с больными.
Вирус нестойкий, поэтому дезинфекцию не проводят. Изоляции подлежат больные опоясывающим герпесом. Описаны попытки применения активной иммунизации. Прививка от ветряной оспы должна проводиться насколько возможно быстро. Разработаны живые аттенуированные вакцины, которые, по наблюдениям их авторов, обеспечивают хороший эффект. Однако большинство специалистов считает проведение массовой вакцинации нецелесообразным.
[47], [48], [49], [50]